Schizophrenia: Clinical Aspects Flashcards
Neurosis vs Psychosis
- Which of these fall under neurosis, which fall under psychosis?
- OCD
- Depressive disorder
- Anxiety disorder
- Schizophrenia
- Depressive psychosis
- Somatisation disorders
- Organic
- Adjustment disorder
- Bipolar disorders
-
Neurosis
- Anxiety disorder
- Depressive disorder
- OCD
- Adjustment disorders
- Somatisation disorders
-
Psychosis
- Organic
- Schizophrenia
- Bipolar disorders
- Depressive psychosis
….: respond to antidepressant or SSRI vs ….: respond to antipsychotic medication
Neurosis: respond to antidepressant or SSRI vs Psychosis: respond to antipsychotic medication
Neurosis: respond to … or … vs Psychosis: respond to … medication
Neurosis: respond to antidepressant or SSRI vs Psychosis: respond to antipsychotic medication
What is Psychosis?
- An illness characterised by a loss of boundaries with … and loss of …, with primary features of …, …. and conceptual disorganisation.
- A psychotic episode is deemed to be 1 week duration of either of these symptoms at significant severity
- Often associated with some sort of … disturbance
- An illness characterised by a loss of boundaries with reality and loss of insight, with primary features of delusions, hallucinations and conceptual disorganisation.
- A psychotic episode is deemed to be 1 week duration of either of these symptoms at significant severity
- Often associated with some sort of behavioural disturbance
What is Psychosis?
- An illness characterised by a loss of boundaries with reality and loss of insight, with primary features of delusions, hallucinations and conceptual ….
- A psychotic episode is deemed to be … … duration of either of these symptoms at significant severity
- Often associated with some sort of behavioural disturbance
- An illness characterised by a loss of boundaries with reality and loss of insight, with primary features of delusions, hallucinations and conceptual disorganisation.
- A psychotic episode is deemed to be 1 week duration of either of these symptoms at significant severity
- Often associated with some sort of behavioural disturbance
What is a Delusion?
- … held firmly but on … grounds, not affected by … argument or evidence to the contrary, and … shared by someone of similar age, educational, cultural, religious or social background
- Types of delusion include: primary (Delusional perception), secondary, persecutory, -of reference, grandiose, -of guild, nihilistic, -of passivity etc.
- Belief held firmly but on inadequate grounds, not affected by rational argument or evidence to the contrary, and not shared by someone of similar age, educational, cultural, religious or social background
- Types of delusion include: primary (Delusional perception), secondary, persecutory, -of reference, grandiose, -of guild, nihilistic, -of passivity etc.
What is a Delusion?
- Belief held … but on inadequate grounds, not affected by rational argument or … to the contrary, and not shared by someone of similar …, educational, cultural, … or … background
- Types of delusion include: primary (Delusional perception), secondary, persecutory, -of reference, grandiose, -of guild, nihilistic, -of passivity etc.
- Belief held firmly but on inadequate grounds, not affected by rational argument or evidence to the contrary, and not shared by someone of similar age, educational, cultural, religious or social background
- Types of delusion include: primary (Delusional perception), secondary, persecutory, -of reference, grandiose, -of guild, nihilistic, -of passivity etc.
Types of delusion include: … (Delusional perception), secondary, …, -of reference, …, -of guilt, nihilistic, -of passivity etc.
Types of delusion include: primary (Delusional perception), secondary, persecutory, -of reference, grandiose, -of guilt, nihilistic, -of passivity etc.
Types of delusion include: primary (… perception), …, persecutory, -of reference, grandiose, -of guilt, …, -of passivity etc.
Types of delusion include: primary (Delusional perception), secondary, persecutory, -of reference, grandiose, -of guilt, nihilistic, -of passivity etc.
Grandiose Delusion - what is this?
Grandiose - mania or related mood, may think they are put on earth for a particular purpose
… delusions occur when someone believes others are out to harm them despite evidence to the contrary.
Persecutory delusions occur when someone believes others are out to harm them despite evidence to the contrary.
What is a Nihilistic delusion?
A delusion that nothing exists, or that a significant aspect of the self (such as one’s brain or the outside world) does not exist - associated with very low mood/psychotic depression
What is a Delusion of passivity?
feel that you are under control of something externally - making you do things
Delusion
- ?Due to error of … of …
- Pay attention to something you see - attribute with more value than someone who is healthy
- E.g. stones outside window - think stones are looking at you in strange way - if healthy, may think stones are weird but would dismiss these thoughts
- ?Due to error of salience of attribution
- Pay attention to something you see - attribute with more value than someone who is healthy
- E.g. stones outside window - think stones are looking at you in strange way - if healthy, may think stones are weird but would dismiss these thoughts
Delusion
- ?Due to … of salience of attribution
- Pay attention to something you see - attribute with more … than someone who is healthy
- E.g. stones outside window - think stones are looking at you in strange way - if healthy, may think stones are weird but would dismiss these thoughts
- ?Due to error of salience of attribution
- Pay attention to something you see - attribute with more value than someone who is healthy
- E.g. stones outside window - think stones are looking at you in strange way - if healthy, may think stones are weird but would dismiss these thoughts
Delusion content often has particular relevance, for example:
- Religious - persecution by devil
- Persecution by authority figure/govt
- Controlled by implant
- Responsibility for world tragedy
- Followed by seagulls
A Hallucination is a perception experienced in the absence of ….
an external stimulus
Define Hallucination
A perception experienced in the absence of an external stimulus
Hallucination
- A … experienced in the absence of an external stimulus
- In any sensory modality but … commonest in psychosis
- ? Due to internal … attribution error
- A perception experienced in the absence of an external stimulus
- In any sensory modality but auditory commonest in psychosis
- ? Due to internal perception attribution error
A hallucination can be in any sensory modality but auditory is commonest in …
psychosis
This brain scan shows someone experiencing a …

hallucination
Conceptual Disorganisation
- … processes are confused, disconnected or disorganized as demonstrated by what they say.
- This is something … and not … of by the individual.
- Also called Loosening of associations (of thought) or Knight’s move thought or Schizophrenic thought disorder or Disorder of form of thought or Formal thought disorder
- Thought processes are confused, disconnected or disorganized as demonstrated by what they say.
- This is something observed and not complained of by the individual.
- Also called Loosening of associations (of thought) or Knight’s move thought or Schizophrenic thought disorder or Disorder of form of thought or Formal thought disorder
Conceptual Disorganisation
- Thought processes are confused, disconnected or disorganized as demonstrated by what they say.
- This is something observed and not complained of by the individual.
- Also called …. of associations (of thought) or Knight’s move thought or … thought disorder or Disorder of form of thought or Formal thought disorder
- Thought processes are confused, disconnected or disorganized as demonstrated by what they say.
- This is something observed and not complained of by the individual.
- Also called Loosening of associations (of thought) or Knight’s move thought or Schizophrenic thought disorder or Disorder of form of thought or Formal thought disorder
Development of the entity of schizophrenia within ‘psychosis’
- Esquirol 1838 - Described course and prognosis of … and separated it from the diagnostic group of mood disturbances (melancholia) which had a better outcome.
- Melancholia - severe …/ deep …
- Esquirol 1838 - Described course and prognosis of insanity and separated it from the diagnostic group of mood disturbances (melancholia) which had a better outcome.
- Melancholia - severe depression/ deep sadness
Development of the entity of schizophrenia within ‘psychosis’
- Kraepelin 1898 - Defined ‘dementia …’ with onset in adolescence of progressive, irreversible decline in mental function. Different forms:
- Hebephrenic - silly, giggly, odd ideas
- … - movement problems, stiff, still
- Paranoid - delusions
- Simplex - negative symptoms, detachment, inner world
- Distinguished … from manic depressive illness
- Kraepelin 1898 - Defined ‘dementia praecox’ with onset in adolescence of progressive, irreversible decline in mental function. Different forms:
- Hebephrenic - silly, giggly, odd ideas
- Catatonic - movement problems, stiff, still
- Paranoid - delusions
- Simplex - negative symptoms, detachment, inner world
- Distinguished schizophrenia from manic depressive illness
Kraepelin 1898
- Defined ‘… praecox’ with onset in adolescence of progressive, irreversible decline in mental function.
- Different forms:
- … - silly, giggly, odd ideas
- Catatonic - movement problems, stiff, still
- Paranoid - delusions
- … - negative symptoms, detachment, inner world
- Distinguished schizophrenia from manic … illness
- Defined ‘dementia praecox’ with onset in adolescence of progressive, irreversible decline in mental function.
- Different forms:
- Hebephrenic - silly, giggly, odd ideas
- Catatonic - movement problems, stiff, still
- Paranoid - delusions
- Simplex - negative symptoms, detachment, inner world
- Distinguished schizophrenia from manic depressive illness
Bleuler 1911
- Coined the term … ‘splitting of the mind’ - nothing to do with what we now know about psychosis - and described fundamental symptoms: abnormal associations, autism, abnormal affect, ambivalence
- Coined the term schizophrenia ‘splitting of the mind’ - nothing to do with what we now know about psychosis - and described fundamental symptoms: abnormal associations, autism, abnormal affect, ambivalence
Schneider 1946
- Defined … … Symptoms pathognomic of schizophrenia
- Defined First Rank Symptoms pathognomic of schizophrenia
… - (of a sign or symptom) specifically characteristic or indicative of a particular disease or condition.
Pathognomic - (of a sign or symptom) specifically characteristic or indicative of a particular disease or condition.
Schneider’s First Rank Symptoms (1946)
- ‘In the absence of organic disease signify …’
- … hallucinations:
- Thoughts spoken aloud
- Third person hallucinations
- Running commentary
- S… hallucinations
- … insertion - new thought arises that isnt your own, withdrawal -taken out of your mind, by antenna? or broadcast - known to others
- … phenomena - not under your control. Made acts/ impulses/ affects
- Delusional perception - first delusion - believe something is happening e.g. aliens landing due to change in traffic light
- ‘In the absence of organic disease signify schizophrenia’
-
Auditory hallucinations:
- Thoughts spoken aloud
- Third person hallucinations
- Running commentary
- Somatic hallucinations
- Thought insertion - new thought arises that isnt your own, withdrawal -taken out of your mind, by antenna? or broadcast - known to others
- Passivity phenomena - not under your control. Made acts/ impulses/ affects
- Delusional perception - first delusion - believe something is happening e.g. aliens landing due to change in traffic light
Schneider’s First Rank Symptoms (1946)
- ‘In the absence of … disease signify schizophrenia’
- Auditory hallucinations:
- Thoughts spoken aloud
- Third person hallucinations
- Running commentary
- Somatic hallucinations
- Thought … - new thought arises that isnt your own, withdrawal -taken out of your mind, by antenna? or broadcast - known to others
- Passivity phenomena - not under your control. Made acts/ impulses/ affects
- … perception - first delusion - believe something is happening e.g. aliens landing due to change in traffic light
- ‘In the absence of organic disease signify schizophrenia’
- Auditory hallucinations:
- Thoughts spoken aloud
- Third person hallucinations
- Running commentary
- Somatic hallucinations
- Thought insertion - new thought arises that isnt your own, withdrawal -taken out of your mind, by antenna? or broadcast - known to others
- Passivity phenomena - not under your control. Made acts/ impulses/ affects
- Delusional perception - first delusion - believe something is happening e.g. aliens landing due to change in traffic light
Schneider’s First Rank Symptoms (1946)
- ‘In the absence of organic disease signify schizophrenia’
- Auditory hallucinations:
- Thoughts spoken aloud
- Third person hallucinations
- Running commentary
- Somatic hallucinations
- Thought insertion - new thought arises that isnt your own, withdrawal -taken out of your mind, by antenna? or broadcast - known to others
- Passivity phenomena - not under your control. Made acts/ impulses/ affects
- Delusional perception - first delusion - believe something is happening e.g. aliens landing due to change in traffic light
- ‘In the absence of organic disease signify schizophrenia’
- Auditory hallucinations:
- Thoughts spoken aloud
- Third person hallucinations
- Running commentary
- Somatic hallucinations
- Thought insertion - new thought arises that isnt your own, withdrawal -taken out of your mind, by antenna? or broadcast - known to others
- Passivity phenomena - not under your control. Made acts/ impulses/ affects
- Delusional perception - first delusion - believe something is happening e.g. aliens landing due to change in traffic light
ICD 10 Diagnosis of schizophrenia
- A minimum of … of a-d or … of e-h for at least 1 month:
- a) Thought echo, insertion, withdrawal or broadcast
- b) Delusion of passivity or delusion perception
- c) Running commentary hallucination or 2 voices discussing the patient
- d) Persistent delusions of other kinds
- e) Persistent hallucinations in any modality with accompanying brief delusions
- f) Breaks in thought resulting in abnormal speech (E.g. incoherent, neologisms)
- g) Catatonic behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) Negative symptoms not due to depression or medication
- In the absence of an organic disorder
- A minimum of one of a-d or two of e-h for at least 1 month:
- a) Thought echo, insertion, withdrawal or broadcast
- b) Delusion of passivity or delusion perception
- c) Running commentary hallucination or 2 voices discussing the patient
- d) Persistent delusions of other kinds
- e) Persistent hallucinations in any modality with accompanying brief delusions
- f) Breaks in thought resulting in abnormal speech (E.g. incoherent, neologisms)
- g) Catatonic behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) Negative symptoms not due to depression or medication
- In the absence of an organic disorder
ICD 10 Diagnosis of schizophrenia
- A minimum of one of a-d or two of e-h for at least 1 month:
- a) Thought echo, insertion, withdrawal or broadcast
- b) Delusion of passivity or delusion perception
- c) Running … hallucination or 2 voices discussing the patient
- d) Persistent … of other kinds
- e) Persistent … in any modality with accompanying brief delusions
- f) Breaks in thought resulting in abnormal speech (E.g. incoherent, neologisms)
- g) Catatonic behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) Negative symptoms not due to depression or medication
- In the absence of an organic disorder
- A minimum of one of a-d or two of e-h for at least 1 month:
- a) Thought echo, insertion, withdrawal or broadcast
- b) Delusion of passivity or delusion perception
- c) Running commentary hallucination or 2 voices discussing the patient
- d) Persistent delusions of other kinds
- e) Persistent hallucinations in any modality with accompanying brief delusions
- f) Breaks in thought resulting in abnormal speech (E.g. incoherent, neologisms)
- g) Catatonic behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) Negative symptoms not due to depression or medication
- In the absence of an organic disorder
ICD 10 Diagnosis of schizophrenia
- A minimum of one of a-d or two of e-h for at least 1 month:
- a) … echo, insertion, withdrawal or broadcast
- b) Delusion of … or delusion …
- c) Running commentary hallucination or 2 voices discussing the patient
- d) Persistent delusions of other kinds
- e) Persistent hallucinations in any modality with accompanying brief delusions
- f) Breaks in thought resulting in abnormal speech (E.g. incoherent, neologisms)
- g) … behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) Negative symptoms not due to depression or medication
- In the absence of an organic disorder
- A minimum of one of a-d or two of e-h for at least 1 month:
- a) Thought echo, insertion, withdrawal or broadcast
- b) Delusion of passivity or delusion perception
- c) Running commentary hallucination or 2 voices discussing the patient
- d) Persistent delusions of other kinds
- e) Persistent hallucinations in any modality with accompanying brief delusions
- f) Breaks in thought resulting in abnormal speech (E.g. incoherent, neologisms)
- g) Catatonic behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) Negative symptoms not due to depression or medication
- In the absence of an organic disorder
ICD 10 Diagnosis of schizophrenia
- A minimum of one of a-d or two of e-h for at least 1 month:
- a) Thought echo, insertion, withdrawal or broadcast
- b) Delusion of passivity or delusion perception
- c) Running commentary hallucination or 2 voices discussing the patient
- d) Persistent delusions of other kinds
- e) Persistent hallucinations in any modality with accompanying brief delusions
- f) Breaks in thought resulting in … speech (E.g. incoherent, neologisms)
- g) Catatonic behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) … symptoms not due to depression or medication
- In the absence of an organic disorder
- A minimum of one of a-d or two of e-h for at least 1 month:
- a) Thought echo, insertion, withdrawal or broadcast
- b) Delusion of passivity or delusion perception
- c) Running commentary hallucination or 2 voices discussing the patient
- d) Persistent delusions of other kinds
- e) Persistent hallucinations in any modality with accompanying brief delusions
- f) Breaks in thought resulting in abnormal speech (E.g. incoherent, neologisms)
- g) Catatonic behaviour e.g. excitement, posturing, waxy flexibility, negativism
- h) Negative symptoms not due to depression or medication
- In the absence of an organic disorder
People with … symptoms in schizophrenia exhibit unusual styles and levels of physical movement
People with catatonic symptoms in schizophrenia exhibit unusual styles and levels of physical movement
Differential Diagnosis - Schizophrenia
- … psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
- … psychosis:
- Epilepsy (temporal lobe)
- Infections: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- Cerebral trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- Endocrine: thyroid disorders (hyper and hypo), Cushing’s syndrome
- Metabolic: hepatic failure, uraemia
- Immunological: SLE
- Acute drug intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
- … disorder
- May describe hallucinations, hard to distinguish
- Eating disorder - strong and unusual ideas - hard to distinguish
-
Affective psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
-
Organic psychosis:
- Epilepsy (temporal lobe)
- Infections: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- Cerebral trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- Endocrine: thyroid disorders (hyper and hypo), Cushing’s syndrome
- Metabolic: hepatic failure, uraemia
- Immunological: SLE
- Acute drug intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
-
Personality disorder
- May describe hallucinations, hard to distinguish
- Eating disorder - strong and unusual ideas - hard to distinguish
Differential Diagnosis - Schizophrenia
- Affective psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
- Organic psychosis:
- E… (temporal lobe)
- Infections: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- C… trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- Endocrine: thyroid disorders (hyper and hypo), Cushing’s syndrome
- …: hepatic failure, uraemia
- Immunological: SLE
- Acute drug intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
- Personality disorder
- May describe hallucinations, hard to distinguish
- Eating disorder - strong and unusual ideas - hard to distinguish
- Affective psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
- Organic psychosis:
- Epilepsy (temporal lobe)
- Infections: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- Cerebral trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- Endocrine: thyroid disorders (hyper and hypo), Cushing’s syndrome
- Metabolic: hepatic failure, uraemia
- Immunological: SLE
- Acute drug intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
- Personality disorder
- May describe hallucinations, hard to distinguish
- Eating disorder - strong and unusual ideas - hard to distinguish
Differential Diagnosis - Schizophrenia
- Affective psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
- Organic psychosis:
- Epilepsy (temporal lobe)
- …: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- Cerebral trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- …: thyroid disorders (hyper and hypo), Cushing’s syndrome
- Metabolic: hepatic failure, uraemia
- Immunological: SLE
- Acute … intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
- Personality disorder
- May describe hallucinations, hard to distinguish
- Eating disorder - strong and unusual ideas - hard to distinguish
- Affective psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
- Organic psychosis:
- Epilepsy (temporal lobe)
- Infections: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- Cerebral trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- Endocrine: thyroid disorders (hyper and hypo), Cushing’s syndrome
- Metabolic: hepatic failure, uraemia
- Immunological: SLE
- Acute drug intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
- Personality disorder
- May describe hallucinations, hard to distinguish
- Eating disorder - strong and unusual ideas - hard to distinguish
Differential Diagnosis - Schizophrenia
- Affective psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
- Organic psychosis:
- Epilepsy (temporal lobe)
- Infections: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- Cerebral trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- Endocrine: thyroid disorders (hyper and hypo), Cushing’s syndrome
- Metabolic: hepatic failure, uraemia
- Immunological: SLE
- Acute drug intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
- Personality disorder
- May describe hallucinations, hard to distinguish
- … disorder - strong and unusual ideas - hard to distinguish
- Affective psychosis:
- Bipolar disorder
- Depressive psychosis
- Schizoaffective disorder
- Organic psychosis:
- Epilepsy (temporal lobe)
- Infections: encephalitis, subacute sclerosing panencephalitis, neurosyphillis, HIV
- Cerebral trauma
- Cerebrovascular disease
- Demyelination: MS etc
- Neurodevelopmental disorders: velocardiofacial symptoms
- Endocrine: thyroid disorders (hyper and hypo), Cushing’s syndrome
- Metabolic: hepatic failure, uraemia
- Immunological: SLE
- Acute drug intoxication: e.g. Ketamine, Cannabis, LSD, PCP, Amphetamine, MDM
- Toxins e.g. lead
- Dementias
- Personality disorder
- May describe hallucinations, hard to distinguish
- Eating disorder - strong and unusual ideas - hard to distinguish
Are there signs of schizophrenia?
- Bizarre appearance or behaviour
- Self …
- ‘talking to …’
- Social disturbance including … violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- Parkinsonian symptoms: tremor, rigidity, bradykinesia
- Tardive dyskinesias including orofacial, athetosis, dystonias
- Skin discolouration
- Severe weight gain
- Bizarre appearance or behaviour
- Self neglect
- ‘talking to themselves’
- Social disturbance including unprovoked violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- Parkinsonian symptoms: tremor, rigidity, bradykinesia
- Tardive dyskinesias including orofacial, athetosis, dystonias
- Skin discolouration
- Severe weight gain
Are there signs of schizophrenia?
- Bizarre appearance or behaviour
- Self neglect
- ‘talking to themselves’
- Social disturbance including unprovoked violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- … symptoms: tremor, rigidity, bradykinesia
- Tardive … including orofacial, athetosis, dystonias
- Skin discolouration
- Severe weight gain
- Bizarre appearance or behaviour
- Self neglect
- ‘talking to themselves’
- Social disturbance including unprovoked violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- Parkinsonian symptoms: tremor, rigidity, bradykinesia
- Tardive dyskinesias including orofacial, athetosis, dystonias
- Skin discolouration
- Severe weight gain
Are there signs of schizophrenia?
- Bizarre appearance or behaviour
- Self neglect
- ‘talking to themselves’
- Social disturbance including unprovoked violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- Parkinsonian symptoms: T…, R…, bradykinesia
- Tardive dyskinesias including orofacial, athetosis, dystonias
- Skin …
- Severe weight gain
- Bizarre appearance or behaviour
- Self neglect
- ‘talking to themselves’
- Social disturbance including unprovoked violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- Parkinsonian symptoms: tremor, rigidity, bradykinesia
- Tardive dyskinesias including orofacial, athetosis, dystonias
- Skin discolouration
- Severe weight gain
Are there signs of schizophrenia?
- Bizarre appearance or behaviour
- Self neglect
- ‘talking to themselves’
- Social disturbance including unprovoked violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- Parkinsonian symptoms: tremor, rigidity, bradykinesia
- Tardive dyskinesias including orofacial, athetosis, dystonias
- … discolouration
- Severe weight …
- Bizarre appearance or behaviour
- Self neglect
- ‘talking to themselves’
- Social disturbance including unprovoked violent acts
- Posturing
- Clothing
- Perplexity
- Side effects of medication
- Parkinsonian symptoms: tremor, rigidity, bradykinesia
- Tardive dyskinesias including orofacial, athetosis, dystonias
- Skin discolouration
- Severe weight gain
Signs of schizophrenia?
- None of the signs are … to schizophrenia
- Hence no objective pathognomonic signs
- … interview is required for diagnosis
- No lab tests/ predictive imaging
- Genetics on track to identify vulnerability only…
- None of the signs are specific to schizophrenia
- Hence no objective pathognomonic signs
- Clinical interview is required for diagnosis
- No lab tests/ predictive imaging
- Genetics on track to identify vulnerability only…
Signs of schizophrenia?
- None of the signs are specific to schizophrenia
- Hence no objective … signs
- Clinical interview is required for diagnosis
- No … tests/ … imaging
- Genetics on track to identify … only…
- None of the signs are specific to schizophrenia
- Hence no objective pathognomonic signs
- Clinical interview is required for diagnosis
- No lab tests/ predictive imaging
- Genetics on track to identify vulnerability only…
Signs of schizophrenia all lead to …
stigma
Mental State Examination findings in the Acute Syndrome (… symptoms) - Schizophrenia
- Appearance: Preoccupied and withdrawn to restless and unpredictable
- Mood: Blunting of mood, disinhibition, perplexed, anxious
- Disorder of thinking: Vague, formal thought disorder (loosening of associations), Disorders of stream (thought block)
- Delusions: Primary, secondary
- Hallucinations: Auditory, visual, tactile (somatic), olfactory, gustatory
- Insight: Impaired
- Cognition: Normal orientation and memory (initially)
- Positive symptoms:
- Appearance: Preoccupied and withdrawn to restless and unpredictable
- Mood: Blunting of mood, disinhibition, perplexed, anxious
- Disorder of thinking: Vague, formal thought disorder (loosening of associations), Disorders of stream (thought block)
- Delusions: Primary, secondary
- Hallucinations: Auditory, visual, tactile (somatic), olfactory, gustatory
- Insight: Impaired
- Cognition: Normal orientation and memory (initially)
Mental State Examination findings in the Acute Syndrome (Positive symptoms) - Schizophrenia
- Appearance: … and withdrawn to restless and unpredictable
- Mood: … of mood, disinhibition, perplexed, anxious
- Disorder of ..: Vague, formal thought disorder (loosening of associations), Disorders of stream (thought block)
- …: Primary, secondary
- Hallucinations: Auditory, visual, tactile (somatic), olfactory, gustatory
- Insight: …
- Cognition: Normal orientation and memory (initially)
- Appearance: Preoccupied and withdrawn to restless and unpredictable
- Mood: Blunting of mood, disinhibition, perplexed, anxious
- Disorder of thinking: Vague, formal thought disorder (loosening of associations), Disorders of stream (thought block)
- Delusions: Primary, secondary
- Hallucinations: Auditory, visual, tactile (somatic), olfactory, gustatory
- Insight: Impaired
- Cognition: Normal orientation and memory (initially)
Mental State Examination findings in the Acute Syndrome (… symptoms) - Schizophrenia
- Appearance: Lack of drive and activity. Social withdrawal. Self neglect
- Movement abnormalities: Stupor, catatonia, abnormal movements and tone
- Mood: Blunting of mood. Depression
- Delusions: As in acute syndrome but may be less evident
- Hallucinations: As in acute syndrome but may be less evident
- Insight: Impaired as in acute syndrome
- Cognition: Normal orientation. Disturbed attention. Later cognitive decline.
- Negative Symptoms
- Appearance: Lack of drive and activity. Social withdrawal. Self neglect
- Movement abnormalities: Stupor, catatonia, abnormal movements and tone
- Mood: Blunting of mood. Depression
- Delusions: As in acute syndrome but may be less evident
- Hallucinations: As in acute syndrome but may be less evident
- Insight: Impaired as in acute syndrome
- Cognition: Normal orientation. Disturbed attention. Later cognitive decline.
Mental State Examination findings in the Acute Syndrome (negative symptoms)
- Appearance: Lack of drive and activity. Social …. Self …
- Movement abnormalities: Stupor, c…, abnormal movements and tone
- Mood: … of mood. Depression
- Delusions: As in acute syndrome but may be … evident
- Hallucinations: As in acute syndrome but may be … evident
- Insight: Impaired as in acute syndrome
- Cognition: Normal orientation. Disturbed attention. Later cognitive …
- Appearance: Lack of drive and activity. Social withdrawal. Self neglect
- Movement abnormalities: Stupor, catatonia, abnormal movements and tone
- Mood: Blunting of mood. Depression
- Delusions: As in acute syndrome but may be less evident
- Hallucinations: As in acute syndrome but may be less evident
- Insight: Impaired as in acute syndrome
- Cognition: Normal orientation. Disturbed attention. Later cognitive decline.
Epidemiology of Schizophrenia
- Prevalence:
- 0.2-0.7%
- Incidence:
- …./10,000 per year. Increasing in S London.
- Geography:
- Incidence up to …x variation worldwide
- Increased rate in … (particularly African Caribbean - culturally isolated Europe)
- More prevalent in … than … areas (increased rates the larger the town and longer lived there)
- Sex:
- … have earlier onset and more negative symptoms
- Onset:
- Male peak onset 21-26
- Female peak onset 25-32
- Social class:
- Lower ‘social drift hypothesis’
- Prevalence:
- 0.2-0.7%
- Incidence:
- 2/10,000 per year. Increasing in S London.
- Geography:
- Incidence up to 5x variation worldwide
- Increased rate in migrants (particularly African Caribbean - culturally isolated Europe)
- More prevalent in urban than rural areas (increased rates the larger the town and longer lived there)
- ‘urban drift’
- Sex:
- Men have earlier onset and more negative symptoms
- Onset:
- Male peak onset 21-26
- Female peak onset 25-32
- Social class:
- Lower ‘social drift hypothesis’
What is the prevalence of Schizophrenia?
0.2-0.7%
Incidence - Schizophrenia
- …/10,000 per year. Increasing in … London.
- 2/10,000 per year. Increasing in S London.
What gender have earlier onset of schizophrenia and more negative symptoms?
men
Onset of schizophrenia
- Male peak onset …-…
- Female peak onset …-…
- Male peak onset 21-26
- Female peak onset 25-32
Onset of schizophrenia
- … peak onset 21-26
- … peak onset 25-32
- Male peak onset 21-26
- Female peak onset 25-32
Schizophrenia is more prevalent in what areas? (rural vs urban)
More prevalent in urban than rural areas (increased rates the larger the town and longer lived there)
… … hypothesis, concerning the relationship between mental illness and social class, is the argument that illness causes one to have a … … in social class.
Social Drift hypothesis, concerning the relationship between mental illness and social class, is the argument that illness causes one to have a downward shift in social class.
Prognosis of Schizophrenia
- … outcome in 3rd world and with introduction of … … Services
- …% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >…% have a relapsing remitting illness with some functional impairment between episodes. Line C
- Recurrent episodes may lead to progressive deterioration
- Functional recovery lags behind symptom recovery
- Suicide in 5-10% particularly men within 3 years of onset

- Better outcome in 3rd world and with introduction of Early Intervention Services
- 20% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >50% have a relapsing remitting illness with some functional impairment between episodes. Line C
- Recurrent episodes may lead to progressive deterioration
- Functional recovery lags behind symptom recovery
- Suicide in 5-10% particularly men within 3 years of onset
Prognosis of Schizophrenia
- Better outcome in 3rd world and with introduction of Early Intervention Services
- 20% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >50% have a relapsing remitting illness with some functional impairment between episodes. Line C
- … episodes may lead to progressive deterioration
- … recovery lags behind symptom recovery
- Suicide in 5-10% particularly … within 3 years of onset

- Better outcome in 3rd world and with introduction of Early Intervention Services
- 20% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >50% have a relapsing remitting illness with some functional impairment between episodes. Line C
- Recurrent episodes may lead to progressive deterioration
- Functional recovery lags behind symptom recovery
- Suicide in 5-10% particularly men within 3 years of onset
Prognosis of Schizophrenia
- Better outcome in … world and with introduction of Early Intervention Services
- 20% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >50% have a relapsing remitting illness with some functional impairment between episodes. Line C
- Recurrent episodes may lead to … deterioration
- Functional recovery lags behind symptom recovery
- … in 5-10% particularly men within 3 years of onset

- Better outcome in 3rd world and with introduction of Early Intervention Services
- 20% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >50% have a relapsing remitting illness with some functional impairment between episodes. Line C
- Recurrent episodes may lead to progressive deterioration
- Functional recovery lags behind symptom recovery
- Suicide in 5-10% particularly men within 3 years of onset
Prognosis of Schizophrenia
- 20% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >50% have a … … illness with some functional impairment between episodes. Line C
- Suicide in …-…% particularly men within 3 years of onset

- Better outcome in 3rd world and with introduction of Early Intervention Services
- 20% complete recovery and off treatment, demonstrated by line a
- 25% have persistent symptoms after first episode or what was originally described as ‘dementia praecox’ Line B
- >50% have a relapsing remitting illness with some functional impairment between episodes. Line C
- Recurrent episodes may lead to progressive deterioration
- Functional recovery lags behind symptom recovery
- Suicide in 5-10% particularly men within 3 years of onset
What % of those with schizophrenia commit suicide?
- Suicide in 5-10% particularly men within 3 years of onset
Functional recovery of schizophrenia lags behind … recovery
Functional recovery of schizophrenia lags behind symptom recovery
Prognosis of Schizophrenia - Good vs bad outcomes
- Highlight whether Good outcomes in:
- Male/Female?
- Married/single?
- Family history of affective disorder or Schizophrenia?
- Good premorbid function
- Acute/Slow onset?
- Life event at onset
- Early treatment/ Long duration untreated?
- Affective/ Negative symptoms?
- Good treatment response?
- Obsessions?
- Premorbidly schizoid?
- High expressed emotion in the family?
- Substance misuse?
- Good outcomes in:
- Male/Female?
- Married/single?
- Family history of affective disorder or Schizophrenia?
- Good premorbid function
- Acute/Slow onset?
- Life event at onset
- Early treatment/ Long duration untreated?
- Affective/ Negative symptoms?
- Good treatment response? Yes
- Obsessions? No
- Premorbidly schizoid? No
- High expressed emotion in the family? No
- Substance misuse? No
Poor prognosis of Schizophrenia in the following groups:
- Male
- Single
- Family history of schizophrenia
- Premorbidly schizoid
- Slow onset
- Long duration untreated
- Negative symptoms
- Obsessions
- High expressed emotion in the family
- Substance misuse
Good prognosis of Schizophrenia in the following groups
- Female
- Married
- Family history of affective disorder
- Good premorbid function
- Acute onset
- Life event at onset
- Early treatment
- Affective symptoms
- Good treatment response
Substance-induced harm

- Majority can smoke cannabis but in those predisposed to psychosis,can cause lots of problems
Cannabis increases vulnerability to psychosis
- Impact of cannabis on developing brain is more potent (
- … patients more sensitive to cannabis than controls
- … liability for psychosis is expressed as differential sensitivity to cannabis
- … use sensitises to effect and increases vulnerability to psychosis
- Many new cannabinoid analogues available
- ? Effect of … on psychosis
- Impact of cannabis on developing brain is more potent (<14 years)
- Schizophrenia patients more sensitive to cannabis than controls
- Familial liability for psychosis is expressed as differential sensitivity to cannabis
- Chronic use sensitises to effect and increases vulnerability to psychosis
- Many new cannabinoid analogues available
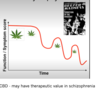
- ? Effect of CBD on psychosis

Cannabis … vulnerability to psychosis
- Cannabis increases vulnerability to psychosis
- Impact of cannabis on developing brain is more potent (<14 years)
- Schizophrenia patients more sensitive to cannabis than controls
- Familial liability for psychosis is expressed as differential sensitivity to cannabis
- Chronic use sensitises to effect and increases vulnerability to psychosis
- Many new cannabinoid analogues available
- ? Effect of CBD on psychosis
Genetic vulnerability to psychosis - … is the most likely current social determinant of transition to psychosis -> first episode psychosis
Genetic vulnerability to psychosis - cannabis is the most likely current social determinant of transition to psychosis -> first episode psychosis
