DIT review - Cardiology 3 Flashcards
In the cardiac cycle graph, show were mitral and aortic valve opening and closing occur


What causes S1 and S2 heart sound
S1 = closing of mitral valve
S2 = closing of aortic valve
What causes S3 heart sound
- S3 = rapid flow of blood from the atria to the ventricles
- Occurs right after mitral valve opens
- Normal in children but not heard in adults
- Presence of S3 in adults indicates volume overload (e.g. congestive heart failure, advanced mitral or tricuspid regurgitation) or dilated ventricles
- Causes of S3 heart sound:
- Dilated cardiomyopathy, congestive heart failure, mitral regurgitation, L-to-R shunting
What causes S4 heart sound
- S4 = atrial contraction
- Not present in normal adults
- Caused by atrium contracting against a stiffened ventricle
- Causes of S4:
- Hypertrophic cardiomyopathy, aortic stenosis, chronic HTN with LV hypertrophy, post-MI
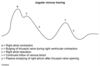
Label the jugular venous tracing graph

- A wave = atrial contraction
- C wave = ventricular contraction
- V wave = atrial filling against closed tricuspid valve
Describe what normal heart sound splitting is
- Inspiration = decreased intrathoracic pressure = increased venous return = increased RV filling = increased RV stroke volume = increased RV ejections time = delayed closure of pulmonic valve

Describe wide splitting
- Splitting occurs both in inspiration and expiration (but still more on inspiration)
- Due to conditions that delay RV emptying (e.g. Pulmonic stenosis, R bundle branch block)

Describe fixed splitting
- Occurs during right heart overload (e.g. atrial septal defect)
- ASD = L-to-R shunt = increased RA and RV volumes = increased flow through pulmonic valve such that, regardless of breath, pulmonic closure is delayed

Describe paradoxical splitting
- Due to conditions that delay aortic valve closure (e.g aortic stenosis, left bundle branch block)
- Normal order of valve closure is reversed so that P2 occurs before delayed A2
- On inspiration, P2 closes later and moves closer to A2, thereby “paradoxically” eliminated the split

What valves associate to what auscultation locations on the chest?

What murmurs are increased by inspiration?
- This decreases intrathoracic pressure, thus increased venous return to the heart
- Increased intensity of R heart sounds (e.g. Tricuspid murmur)
What murmur are increased by hand grip?
- This increases SVR, this increasing afterload
- Increased intensity of mitral regurgitation, aortic regurgitation, and VSD
What murmurs are increased by Valsalva maneuver?
- This increases intrathoracic pressure, thus decreasing preload (opposite of inspiration)
- Decreases the intensity of most murmurs EXCEPT increases intensity of hypertrophic cardiomyopathy
Holosystolic, high-pitched “blowing” murmur best heard at apex
Mitral regurgitation
Causes of mitral regurgitaton
- Rheumatic heart disease, endocarditis, ischemic heart disease, LV dilation, mitral valve prolapse
What maneuver enhances mitral regurg vs. tricuspid regurg
Mitral regurg enhanced by increased afterload (e.g. hand grop or squatting)
Tricuspid regurg enhanced by inspiration
High-pitched “blowing” early diastolic decrescendo murmur
Aortic/pulmonic regurgitation
Common presentation of aortic regurgitation
- Wide pulse pressure with head bobbing – bounding pulses
Causes of aortic regurgitation
- Aortic root dilation (e.g. syphilis or Marfan)
- Bicuspid aortic valve
- Endocarditis
- Rheumatic fever
Holosystolic, harsh-sounding murmur loudest at tricuspid area
Tricuspid regurg or VSD
Differentiate due to clinical picture:
Tricuspid regurg = IV drug user
VSD = murmur present at birth
Late systolic cresecendo murmur, preceded by a mid-systolic click
Mitral valve prolapse
Delayed, rumbling mid-to-late diastolic murmur following an opening snap
Mitral/tricuspid stenosis
Continuous, machine-like murmur (heard through systole and diastole)
Patent ductus arteriosus


