OSPE - Pathology tutorial pictures Flashcards

New Epidermis on the top



What type of healing and label


What type of healing?

Secondary Intention:
- closure of the wound edge isn’t possible and a large deficit is present.
- additional step with wound contraction. Modified fibroblasts termed myofibroblasts contract, reducing the size of the deficit to be replaced
What’s this?

Keloid - overgrowth of scar tissue. Overgrowth of collagen.
Overgrowth of scar tissue is ‘proud flesh’ - looks different

What’s happened here?

Wound dehiscence in a failed primary closure
dehisce = (of a pod or seed vessel, or a cut or wound) gape or burst open:

P = periosteum
C = cortical bone (lamellar bone)
O = osteocytes in lacunae
H = haversian canal




What’s going on here?

Non-union (bone ends are too far apart, fibrous union is when bone ends are joined by fibrous tisseu and bone’s failed to from) of femoral shaft following internal fixation
What’re these two conditions and what’re the common features seen?

Acute meningitis and acute appendicitis
Can see:
- vasodilation and congestion
- redness
- pus associated with meningitis
What’s this? And what can you see going on?

Subarachnoid space - congested vessels, background of stringy proteinaceous exudate and neutrophils
That vessel - dilated and lots of cells around - mostly neutrophils


This is a close up of the subarachnoid space in the brain. Normally this contains clear fluid and a scant number of cells
What’re the signs of acute inflammation seen in this photo?

Swelling, redness and pus
It’s actually carbuncle: a severe abscess or multiple boil in the skin, typically infected with staphylococcus bacteria (staph aureus)
Vessel that shows acute inflammation
- what are the cells lining the vessels?
- what’s the organisation of these cells?
- what adhesion molecues are involved?


How will these leisons heal?

Primary intetion - the skin edges are placed in close proximity. If you leave it like the one on the left, you’ll get a big scar
- How will this type of wound be treated?
- What options could be considered?


Label what you can

Wound contraction by myofibroblasts


The middle part - hard callous bc bone comes up pink

Name the tissues X, Y, Z and the cells a and b

X is cartilage because open tissue and grey/blue with frog eyes so those are chondrocytes/blasts

What cells are responsible for producing new bone?
Pluripotent cell derived from periosteum and bone marrow
5 months later - what’s happened?

Non union has occured - they haven’t healed together (bone ends too far apart)
What is this a histology preparation from? What’s S and T?
What’s the diagnosis?
What’re some of the reasons that this has occured?
5 months later, still bad - what’re you gonna do?

From area of non union. S is fibrous connective tissue and T is woven bone. This is fibrous non union:
- Okay, so this is fibrous (mal)union - fibrous tissue connects the bone ends. Misalinged union of fracture by fibrous tissue. Surgery required to correct alignment and remove the fibrosis tissue. Bone grafting used to reproduce the haemotoma and start the healing process
- Non union is just wheh the bones are too far apart so probably dont get FCT?
Reasons it has happened:
- Excessive movement
- Not enough movement
- Infection
- Poor blood supply
- Poor nutrition
- Medications
After 5 months: reoperate and debride the connective tisse and create a new soft callus
Label
What condition is this?

Rheumatoid Arthritis

What’s this diagnosis - what’s actually going on?

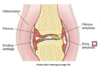
What’s this and what’s going on?

This knee shows the attachment of the pannus (hyperplastic synovium) as the very red material at the periphery of the joint and centrally
The cartilage is pitted and fkaling off in parts, exposing the underlying bone
This is RA

What’s this an x ray of?
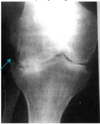
Shows the loss of joint space due to loss of the articular cartilage. There are erosions at the periphery of the joint in the area where the pannus would have originated from
RA
What’s each?

RA

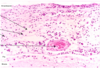
What’re these? What do they arise from? What’re they part of?

RA: subcutaneous nodules - painless pumps arising in the subcutaneous tissue of skin in areas which are subjected to pressure. Rarely they may occur on visceral surfaces. Occur in people with severe disease
These nodules have a fibroid necrotic core which is surrounded by a palisade of macrophages (epitheloid cells) lymphocytes and plasma cells
So in this picture, the star is the fibrinoid necrosis and the triangle is epitheloid cells

What’s happened here?

Left: normal articular cartialge
Right: fibriliation of articular cartilage
- Cartialage degeneration seen as a change in staining, from the normal blue/grey colour to a very pale blue/pink (due to changes in ground substance)
- Cartilage beings to break down: the exposed surface becomes frayed (fibrillated) and eventually the cartialge will be lost completely
This is OA
Label and what’s the condition?


Label the three and tell me the condition

1 = Eburnated articular surface exposing the subchondral bone
2 = Subchondral cyst
3 = Residual articular cartilage
OA
What’s going on here?

OA - Subchondral cyst
OA

What does the arrow indicate?

Indicates the subchondral cyst
OA
What’s going on here?

Osteophyte in the knee where the arrow is
OA
What’s this?

Gout

What’s this?
Gout

What’s this?

Osteomyelitis

Involucrum: new bone laid down beneath the periosteum and may, if large enough, encase the dead bone
Sequestrum: dead bone resulting from either pressure within the marrow cavity or due to loss of the bone supply because of lifting of the periosteum
Osteomyelitis

What’s this procedure called?

Debridement - clean the dead tissue and pus
For osteomyelitis
The bone has been exposed and the cortex removed and the medullary bone being debrided
Healing will not occur if there is dead tissue present which is avascular and may harbour organisms
What’s going on here?


What about here?

Osteomyelitis

Describe the abnormality in these knees

OA:
- varus deformity (bow legs)
- quadriceps muscles wasted
- on examination: decreased range of movement - osteophyte formation
- crepitus
- pain
What does this x-ray show?

X-ray of osteoarthritis
- loss of joint space medially
- sclerosis of the adjacent bone
- osteophytes
Like, laterally there is normal cartilage and synovial fluid. Osteophyte on the media side like right at the edge
Describe this patella and femoral condyles as well as the condition

The articular cartilage on both is pitted with erosion of the cartilage exposing the underlying bone on the right femoral condyle
-OA
Describe this femoral head

Can see the lip of the intact cartilage
OA

Describe the changes in the cartilage

Loss of the typical bluish staining
Small islands of hyperplasia of the chondrocytes on the right
On the left surface has become frayed - fibrillation
Bits of cartialge may dislodge from here to form ‘joint mice’
- multiple chondrocytes in lacunae
- dried out and cracks can form
OA
Label

OA

Where is this from?

On top - nothing in osteocytes so cancellous bone on top is dead
the white blob - fat (normal)
Osteomylitis
Acute inflammation so pus

What’re the x ray changes here?

RA - main feature is the erosion of the bone at the periphery of the joint
Why have the changes occured in this position? Pannus is modified synovium which is situatied at the periphery of the joint
What’s this material?

RA

Describe this histology:

Pannus - RA
So the right is a medium power of the pannus and the left is a magnified version
if = inflammatory cells
f = fibrovascular
-fleshy fronds of synovium with the darkly staining areas representing chronic inflammatory cells

This is a higher magnification of something

Pannus

What clinical case does this correspond to?

Acute gout - inflammation at the great toe but whole foot swells
Systemically you’ll experience fever, rasied ESR etc



What’s this leison?

Gout - pinna of an ear with a soft tissue tophus

What’re these crystals?

Uric acid crystals as tophi on soft tissue and if dissolve in joint space = inflammation
Fluid aspirated from an infected joint - what will it show when examined under a microscope? Which clinical case does this correspond to?

Fibrous protein exudate and a cellular exudate comprising neutrophils and macrophages
Gram stain may show which organisms
Septic arthritis
What’s this organism?

Gram -ve diplococcus so neisseria meningitidis
What’re the causative agents (bacteria) of meningitis in neonates, infants, adolescents and elderly?

What’s this?

Granuloma!

What’s the CSF meant to look like in
- Acute bacterial
- Acute viral
- Chronic tuberculosis
in terms of colour/turbidity, pressure, cells, protein, glucose and gram stain of CSF
- Creamy bc purulent, increased pressure, increased cell count, increased protein (because inflammatory exudate), glucose decreased as neutrophils and organisms use energy source, gram stain will allow identification
- clear to cloudy, mild to moderate increase pressure, increased cells (mainly mononuclear), protein is moderately increased, glucose is normal and gram stain negative (can’t culture)
- Cloudy - not purulent!, mild to moderate increase pressure, cells increase (mainly mononuclear), mild increase in protein, glucose mild to moderate DECREASE, gram stain negative (can be identified by PCR and/or grown on special culture medium)
What’s going on?

Acute meningitis - the brain is swollen, marked vasocongestion and dilation of the vessels, pus in the subarachnoid space especially around the brain stem and cerebellum
Repeated but yeah: what’s up?


What’s this?


Is this meninges normal or abnormal?

Normal
Just confirming you know, what’s this?
Acute inflammation from meningitis

What’re the abnormalities?

- Small nodules throughout the meninges are granulomata
- TB
- CSF has raised protein and reduced glucose
- chronic inflammation
What’s up?

So purple part is meninges on the right and it’s thickened

What’s this?

Granuloma showing features of
- central caseous necrosis (a condition characteristic of tuberculosis, in which diseased tissue forms a firm, dry mass like cheese in appearance)
- surrounding infiltrate of epitheloid cells (modified macrophages) and occasional giant cells (fusion of macrophages)
- scattered mononuclear cells at periphery
p = pink sheet - epitheloid sheet of cells etc
d = dead necrotic material
w = wall formed by mononuclear cells recrutiment
g = giant cell (fusion of macrophages - do this when come across something indigestable)
s = epithelpid cells
Granuloma - body comes across something it can’t destroy. In TB, it’s type 4 hypersensitivity - cell mediated immunity - cytokines produced by T cells - instruct macrophages to become epitheloid or giant cells. Oragnism gets entrapped in gramuloma or macrophage combine resources to eat it so roganism in either giant cells or surrounded by macrophae. T cells release cytokines to recruit macro and monocytes

What does this blood film show?

Central neutrophil containing diplococcus organisms - absense of platelets
This is a gram stain - what does it show?


What’s up?
DIC



Glomeruli of a women with DIC - red is fibrin

