Nerve Palsies in the Limbs Flashcards
Every peripheral nerve starts from the __________ - eg. the sciatic nerve is often over 1 metre long from origin to terminal branches
spinal cord
what is a dermatome?
- sensory area of skin supplied by a single spinal nerve
- adjacent dermatomes overlap considerably
- embryological development of limb buds growing out from body wall results in axial lines (anterior and posterior) - there is no overlap between adjacent pre- and post-axial dermatomes

what are the dermatomes like in the lower limbs?
- lower limb dermatomes distorted by rotation and extension, and “borrowing” of skin from trunk
- STAND on S1
- SLEEP on S2
- SIT on S3
**** on S4 !

what is hiltons law?
“The nerves crossing a joint supply the muscles acting on it and the joint itself.”
n.b. may supply 2 joints, eg. hip and knee supplied by femoral, sciatic and obturator nerves –
HIP DISEASE MAY GIVE RISE TO KNEE PAIN
what is a myotome?
•group of muscles supplied by one segment of spinal cord
what is the brachial plexus?
- large network of nerves supplying the upper limb, extending from the cervical spine to the axilla
- anatomical variations common -eg. C4-8 = pre-fixed plexus, C6-T2 = post-fixed plexus
- Roots
- Trunks
- Divisions
- Cords
- Branches

how are brachial plexus lesions caused by downward traction, what is damaged and what is the effect?

- downward traction (eg. fall on side of neck)
- C5, 6 damage (deltoid & shoulder muscles, brachialis & biceps)
- arm “porter’s tip” (Erb-Duchenne paralysis)
Common in childbirth, and accidents - Pulling baby pulls on upper cords, C5 and C6

what is Arm “porters tip” (Erb-Cuchenne paralysis)?
Arm adducted as deltoid no longer works, elbow is extended because biceps not working, forearm pronated and wrist flexed
Right shows child developed it in childbirth, tends to rapidly resolve

what is erbs point?
“Erb’s point” is also a term used in head and neck surgery to describe the point on the posterior border of the sternocleidomastoid muscle where the four superficial branches of the cervical plexus—the greater auricular, lesser occipital, transverse cervical, and supraclavicular nerves—emerge from behind the muscle

how are brachial plexus lesions caused by upward traction, what is damaged and what is the effect?

- upward traction (eg. breech delivery)
- T1 damage (intrinsic muscles)
- hand “clawed” (Klumpke’s paralysis) – claw hand
Lower cords
This is upward traction instead of downward traction

In descriptive anatomy of forearm, wrist and hand, what words should be used?
- use “RADIAL” and “ULNAR” (rather than lateral and medial)
- use “VOLAR” or “PALMAR” and “DORSAL” (rather than anterior and posterior)
is the Axillary Nerve at risk and what may it be a complication of?
- at risk - wraps around surgical neck of humerus
- complication of - # humeral neck, shoulder dislocation, Saturday night palsy (pressure on post. cord of brachial plexus)
what make sup the axillary nerve and what does it supply?
C5, C6 - posterior cord
Supplies deltoid and teres minor
Supplies skin over lateral arm – regimental badge area
what motor and sensory loos would be seen in axillary nerve damage?
- motor deficit - loss of shoulder abduction (deltoid)
- sensory deficit - badge area
If they have reduced sensation then pretty sure axillary nerve has been injured and leads to deltoid atrophy, if identify at point of injury you can introduce physiotherapy to ensure

what are the roots of the radial nerve and where is it located?
- roots - C5, 6, 7, 8, T1, posterior cord
- in arm, closely associated with - profunda brachii artery
- enters forearm by passing between - brachioradialis & brachialis (and posterior interosseous branch of radial nerve passes between 2 planes of supinator)
Runs in radial groove of the humerus as it passes from medial to lateral
where is the radial nerve at risk?
at risk - spiral groove of humerus & lat. intermuscular septum (and posterior inter-osseous branch at radial neck)
raidal nevre damage may happen in what complication?
humeral shaft, Saturday night palsy (pressure on post. cord of brachial plexus), exposure of proximal radius
if the radial nerve is dmaaged, what motor or sensory deficit may be seen?

- motor deficit - wrist drop (extensors)
- sensory deficit - 1st web space dorsall
Radial nerve palsy symptoms depend on site of lesion:
Axilla = loss of elbow extension, wrist extension and sensory changes forearm and hand
Arm = loss of wrist extension and sensory loss
Forearm = loss of fingers extension (PIN)
Wrist = loss of sensation (SRN) e.g. handcuff

what makes up the median nerve?
roots - C7, 8, T1
Medial and lateral cord supply
where is the median nerve located?
- in arm, closely associated with - brachial artery
- enters forearm by passing between - two heads of pronator teres

what does the median nevre supply?
Supplies flexors forearm (apart from FCU an medial half of FDP), LOAF muscles
Supplies sensation to the radial 3.5 digits

where is the median nerve at risk and of what complication?
- at risk - volar aspect wrist (& cubital fossa)
- complication of - carpal tunnel syndrome, wrist lacerations (& supracondylar #’s, Struther’s ligament)
if the median nerve is damaged what is the motor and sensory loss?
- motor deficit - thenar wasting (monkey hand), pointing finger
- sensory deficit - volar aspect thumb
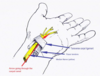
what makes up carpel tunnel?
Floor – carpal bones
Roof – flexor retinaculum
Contents – FDS x4, FDP x4, FPL and median nerve i.e. 9 tendons and a nerve