HD2 Qs Flashcards
mBob, 70-years-old, presents to his General Practitioner (GP) complaining of frequent urination accompanied by a burning sensation and interrupted flow of urine that have been going on for about 4 months. Digital rectal examination reveals an enlarged, nodular prostate and his prostate- specific antigen (PSA) levels are very high. After his biopsy results come back, he is diagnosed with prostate cancer. Which prostatic zone typically enlarges with prostatic cancer?
Transitional zone
Periurethral gland region
Fibromuscular zone
Central zone
Peripheral zone
Bob, 70-years-old, presents to his General Practitioner (GP) complaining of frequent urination accompanied by a burning sensation and interrupted flow of urine that have been going on for about 4 months. Digital rectal examination reveals an enlarged, nodular prostate and his prostate- specific antigen (PSA) levels are very high. After his biopsy results come back, he is diagnosed with prostate cancer. Which prostatic zone typically enlarges with prostatic cancer?
Transitional zone
Periurethral gland region
Fibromuscular zone
Central zone
Peripheral zone
A 72-year-old man presents with symptoms and signs of benign prostatic hyperplasia. Which one of the following structures is most likely to be enlarged?
Posterior lobe of the prostate
Median lobe of the prostate
Right lateral lobe of the prostate
Left lateral lobe of the prostate
Anterior lobe of the prostate
A 72-year-old man presents with symptoms and signs of benign prostatic hyperplasia. Which one of the following structures is most likely to be enlarged?
Posterior lobe of the prostate
Median lobe of the prostate
Right lateral lobe of the prostate
Left lateral lobe of the prostate
Anterior lobe of the prostate
A 26-year-old man attends the GP with abdominal pain and diarrhoea. The GP suspects gastritis but checks his urine in case of a UTI. The results are as follows:
Blood Neg mmol/l
Protein Neg mmol/l
Leukocytes ++ mmol/l
Nitrites Neg mmol/l
Which of the following is an explanation for the abnormal urine dipstick result?
Benign prostatic hypertrophy (BPH)
Chlamydia
Ureteral stricture
Neurogenic bladder
Diarrhoea
A 26-year-old man attends the GP with abdominal pain and diarrhoea. The GP suspects gastritis but checks his urine in case of a UTI. The results are as follows:
Blood Neg mmol/l
Protein Neg mmol/l
Leukocytes ++ mmol/l
Nitrites Neg mmol/l
Which of the following is an explanation for the abnormal urine dipstick result?
Benign prostatic hypertrophy (BPH)
Chlamydia
Ureteral stricture
Neurogenic bladder
Diarrhoea
An 84-year-old man admitted to the neurology ward informs the nurse that he is unable to urinate. He appears significantly distressed and reports pain due to urinary retention. The nurse places him in a warm bath, where the patient is finally able to relax his sphincter and urinates.
Which of the following nervous structures was responsible for maintaining detrusor capacity and making it difficult for the patient to urinate?
Hypogastric plexuses
Inferior mesenteric plexus
Pelvic splanchnic nerves
Prostatic hyperplasia
Pudendal nerve
An 84-year-old man admitted to the neurology ward informs the nurse that he is unable to urinate. He appears significantly distressed and reports pain due to urinary retention. The nurse places him in a warm bath, where the patient is finally able to relax his sphincter and urinates.
Which of the following nervous structures was responsible for maintaining detrusor capacity and making it difficult for the patient to urinate?
Hypogastric plexuses
Inferior mesenteric plexus
Pelvic splanchnic nerves
Prostatic hyperplasia
Pudendal nerve
A neonate born with clubbed feet dies shortly after birth due to severe respiratory distress. His mother had not sought antenatal care. Post-mortem shows pulmonary hypoplasia.
Which of the following clinical features would most likely also be present?
Bilateral renal agenesis and oligohydramnios
Bilateral renal agenesis and polyhydramnios
Cleft palate
Oesophageal atresia and oligohydramnios
Oesophageal atresia and polyhydramnios
A neonate born with clubbed feet dies shortly after birth due to severe respiratory distress. His mother had not sought antenatal care. Post-mortem shows pulmonary hypoplasia.
Which of the following clinical features would most likely also be present?
Bilateral renal agenesis and oligohydramnios
Bilateral renal agenesis and polyhydramnios
Cleft palate
Oesophageal atresia and oligohydramnios
Oesophageal atresia and polyhydramnios
Which structure does the uterine artery pass over?
Round ligament
Ovarian ligament
Ureter
Ovary
Which structure does the uterine artery pass over?
Round ligament
Ovarian ligament
Ureter
Ovary
Complete the sentence: The ovarian ligament connects the ovary to the ______________.
Lateral surface of the uterus
Labia majora
Lateral abdominal wall
Pubic symphysis
Complete the sentence: The ovarian ligament connects the ovary to the ______________.
Lateral surface of the uterus
Labia majora
Lateral abdominal wall
Pubic symphysis
Label A-E of female anatomy [5]

A: bulb of the vestibule
B: levator ani
C: Obturator internus muscle
D: Left ureteric orifice
E: Muscular coat of urinary bladder

Label A-E

A: vagina
B: crus of clitoris
C: labia minoria
D: glands of clitoris
E: cervix

Label A

Vesico-uterine pouch
Label A-E

A: round ligament
B: broad ligament
C: suspensory ligament
D: uterine ligament
E: ovarian ligament
Label: 2, 3, 7, 8 and 10 [5]

2: uterine ligament
3: ovarian ligament
7: ureter
8: rectum
10: bladder
Which is the recto-uterine pouch? [1]

14

Label A-E

A: Clitoris
B: Labium minorum
C: bulb of vesitubule
D: ischiocavernous
E: Bartholin gland / greater vestibular gland

Label A-D

A: Perineal branches of pudendal nerve
B: Levator ani muscle
C: Inferior rectal nerves
D: Gluteus maximus muscle

Label the nerves of External female genital organs highlighted [4]

5:Dorsal nerve of clitoris
8 Perineal branches of pudendal nerve:
15: Pudendal nerve and internal pudendal artery
16: Inferior rectal nerves
Label A-F

A: ureter
B: uterine artery
C: levator ani muscle
D: vagina
E: round ligament
F: uterus
Which immunoglobins are produced when have antisperm antibodies? [3]
Develop antisperm antibodies (ASA): IgG, IgA and IgM
Which artery is 14? [1]

Internal iliac artery
label 1-9

1 Glans of clitoris
2 Labium majus
3 Vestibule of vagina
4 Hymen
5 Posterior labial commissure
6 Body of clitoris
7 Labium minus
8 External orifice of urethra
9 Vaginal orifice

Label 1-3 & 6-9

1 Body of clitoris
2 Crus of clitoris
3 Bulb of vestibule
4 Prepuce of clitoris
5 Glans of clitoris
6 Frenulum of clitoris
7 Labium minus
8 Vaginal orifice
9 Greater vestibular gland
Label the highlighted numbers [4]

11 Ilio-inguinal nerve
13 Superficial inguinal ring
14 Round ligament of uterus
16 Aponeurosis of external abdominal
oblique muscle
Label the highlighted guys [3]
24 Levator ani muscle
25 Pudendal nerve and
internal pudendal artery
26 Inferior rectal nerves

Label 1-14

1 Ilium
2 Rectum
3 Recto-uterine fold
4 Ovary
5 Uterine tube
6 Urinary bladder
7 Urethra
8 Labium minus
9 Recto-uterine pouch of
Douglas
10 Uterus (uterovesical
pouch)
11 Ligament of the head of
the femur
12 Head of femur
13 Vestibule of vagina
14 Labium majus
In the UK, what test is used to diagnose gestational diabetes?
HBA1c
Oral glucose tolerance test
Random plasma glucose
Capillary glucose
In the UK, what test is used to diagnose gestational diabetes?
HBA1c
Oral glucose tolerance test
Random plasma glucose
Capillary glucose
What is the standard initial treatment for gestational diabetes?
Insulin
Metformin
Glibenclamide
Exenatide
What is the standard initial treatment for gestational diabetes?
Insulin
Metformin
Glibenclamide
Exenatide
In a woman with drug-managed gestational diabetes, what are the recommendations for delivery?
Caesarian section at 35 weeks
Deliver at 37-38 weeks
Deliver at term
Allow the pregnancy to prolong as much as possible - do not induce.
In a woman with drug-managed gestational diabetes, what are the recommendations for delivery?
Caesarian section at 35 weeks
Deliver at 37-38 weeks
Deliver at term
Allow the pregnancy to prolong as much as possible - do not induce.
Women who have gestational diabetes should aim to deliver at 37-38 weeks if they are on pharmacological management. They would be advised to consider induction of labour or Caesarean section before 40+6 weeks if they are managing gestational diabetes with diet alone.
What score on oral glucose tolerance test would indicate GD fir fasting and at 2 hrs? [2]
Normal is:
Fasting: < 5.6 mmol/l
At 2 hours: < 7.8 mmol/l
cutoff for gestational diabetes as simply 5 – 6 – 7 – 8.
Which of the following is most problematic later in pregnancy / during birth?
Group B strep
Rubella
Toxoplasmosis gondii
CMV
Which of the following is most problematic later in pregnancy / during birth?
Group B strep
Rubella
Toxoplasmosis gondii
CMV
Others are all first trimester
Parovirus attacks which type of cells?
Neutrophils
Monocytes
Erythrocytes
B cells
Parovirus attacks which type of cells?
Neutrophils
Monocytes
Erythrocytes
B cells
During a routine appointment, a pregnant woman is found to have lower blood pressure than before she became pregnant. She is reassured that this is normal. Which substrate is responsible for this?
Angiotensin
Testosterone
Progesterone
Nitric oxide
Atrial natriuretic hormone
During a routine appointment, a pregnant woman is found to have lower blood pressure than before she became pregnant. She is reassured that this is normal. Which substrate is responsible for this?
Angiotensin
Testosterone
Progesterone
Nitric oxide
Atrial natriuretic hormone
During a routine appointment, a pregnant woman is found to have lower blood pressure than before she became pregnant. She is reassured that this is normal. Which substrate is responsible for this?
Angiotensin
Testosterone
Progesterone
Nitric oxide
Atrial natriuretic hormone
During a routine appointment, a pregnant woman is found to have lower blood pressure than before she became pregnant. She is reassured that this is normal. Which substrate is responsible for this?
Angiotensin
Testosterone
Progesterone
Nitric oxide
Atrial natriuretic hormone
What pathology does this depict? [1]

Placenta praevia
Fig 3 – Anterior placenta previa. The placenta (arrow) has covered the internal os completely (arrowhead).
A woman presents after difficulty conceiving for two years. A subsequent ultrasound reveals fibroids and the doctor explains that they are likely to be preventing embryo implantation. Where are they likely to be located?
Vagina
Uterus- submucosal
Uterus- intramural
Uterus- subserosal
Cervix
A woman presents after difficulty conceiving for two years. A subsequent ultrasound reveals fibroids and the doctor explains that they are likely to be preventing embryo implantation. Where are they likely to be located?
Vagina
Uterus- submucosal
Uterus- intramural
Uterus- subserosal
Cervix
A pregnant woman is counselled on the importance of screening of Rhesus incompatibility between her and her baby. Which combination of maternal and fetal Rh statuses would pose a risk of Rhesus disease?
There is a 15% risk regardless of Rh statuses
Rh-negative mother and Rh-positive baby
Rh-negative mother and Rh-negative baby
Rh-positive mother and Rh-negative baby
Rh-positive mother and Rh-positive baby
A pregnant woman is counselled on the importance of screening of Rhesus incompatibility between her and her baby. Which combination of maternal and fetal Rh statuses would pose a risk of Rhesus disease?
There is a 15% risk regardless of Rh statuses
Rh-negative mother and Rh-positive baby
Rh-negative mother and Rh-negative baby
Rh-positive mother and Rh-negative baby
Rh-positive mother and Rh-positive baby
A 22-year-old woman presents to the Emergency Department with vaginal bleeding and abdominal pain. She is 11 weeks pregnant. On examination, there is bleeding but the uterus is the size expected from the dates given and the cervical os is closed. Which of the following terms best describes this situation?
Complete miscarriage
Incomplete miscarriage
Inevitable miscarriage
Septic miscarriage
Threatened miscarriage
A 22-year-old woman presents to the Emergency Department with vaginal bleeding and abdominal pain. She is 11 weeks pregnant. On examination, there is bleeding but the uterus is the size expected from the dates given and the cervical os is closed. Which of the following terms best describes this situation?
Complete miscarriage
Incomplete miscarriage
Inevitable miscarriage
Septic miscarriage
Threatened miscarriage
Which of the following is a feature of the Leydig cells in the testes?
Elongated in shape
Secrete androgen-binding protein and tubular fluid
Produce testosterone
Support developing sperm during spermatogenesis
Form the blood-testes barrier
Which of the following is a feature of the Leydig cells in the testes?
Elongated in shape
Secrete androgen-binding protein and tubular fluid
Produce testosterone
Support developing sperm during spermatogenesis
Form the blood-testes barrier
A 52-year-old female presents to your clinic with chronic tiredness. She does not report any weight gain or cold intolerance. You perform an investigatory workup that demonstrates the following:
Haemoglobin A1c (HbA1c) 36 mmol/mol (< 42)
Ferritin 176 ng/mL (20 - 230)
Vitamin B12 897 ng/L (200 - 900)
Folate 0.2 nmol/L (> 3.0)
Thyroid Stimulating Hormone (TSH) 4.23 mU/L (0.45 - 5.0)
Which one of the following would be responsible for the deficiency seen in this patient?
Laxative abuse
Menopause
Phenytoin
Tobacco use
Vitamin B12 injections
**A 52-year-old female presents to your clinic with chronic tiredness. She does not report any weight gain or cold intolerance. You perform an investigatory workup that demonstrates the following:
Haemoglobin A1c (HbA1c) 36 mmol/mol (< 42)
Ferritin 176 ng/mL (20 - 230)
Vitamin B12 897 ng/L (200 - 900)
Folate 0.2 nmol/L (> 3.0)
Thyroid Stimulating Hormone (TSH) 4.23 mU/L (0.45 - 5.0)
Which one of the following would be responsible for the deficiency seen in this patient?
Laxative abuse
Menopause
Phenytoin
Tobacco use
Vitamin B12 injections
Phenytoin is a cause of folic acid deficiency
A 26-year-old G2P1 woman who is 7-weeks pregnant presents to the obstetric emergency department with severe vomiting and nausea. The patient explains that their symptoms started around 3 weeks ago, and are now vomiting up to 12 times a day.
Her weight is recorded by the doctor, which shows a decrease of 5.5% from her usual weight.
Investigations show the following results:
Na+ 131 mmol/L (135 - 145)
K+ 3.2 mmol/L (3.5 - 5.0)
Cl- 92 mmol/L (98-106)
Urea 4.5 mmol/L (2.0 - 7.0)
Creatinine 115 µmol/L (55 - 120)
Serum ketones 0.1 mmol/L (<0.6 mmol/L)
What would you expect on an arterial blood gas (ABG)?
Metabolic acidosis
Metabolic alkalosis
Mixed respiratory and metabolic acidosis
Respiratory acidosis
Respiratory alkalosis
A 26-year-old G2P1 woman who is 7-weeks pregnant presents to the obstetric emergency department with severe vomiting and nausea. The patient explains that their symptoms started around 3 weeks ago, and are now vomiting up to 12 times a day.
Her weight is recorded by the doctor, which shows a decrease of 5.5% from her usual weight.
Investigations show the following results:
Na+ 131 mmol/L (135 - 145)
K+ 3.2 mmol/L (3.5 - 5.0)
Cl- 92 mmol/L (98-106)
Urea 4.5 mmol/L (2.0 - 7.0)
Creatinine 115 µmol/L (55 - 120)
Serum ketones 0.1 mmol/L (<0.6 mmol/L)
What would you expect on an arterial blood gas (ABG)?
Metabolic acidosis
Metabolic alkalosis
Mixed respiratory and metabolic acidosis
Respiratory acidosis
Respiratory alkalosis
The electrolyte abnormalities seen in hyperemesis gravidarum include hyponatraemia, hypokalaemia, hypochloraemia and metabolic alkalosis
A 35-year-old women attends the emergency department with acute onset left-sided lower abdominal pain, small amounts of dark brown vaginal discharge and shoulder tip pain.
On further questioning, she has not had a period for around 8 weeks but normally has a regular 30 day cycle. She is currently sexually active with multiple partners, and doesn’t always use contraception. She has also been experiencing diarrhoea and episodes of dizziness for the past 2 days.
A transvaginal ultrasound scan is performed. This shows a gestational sac in the left Fallopian tube.
β-hCG >1500 IU (<5 IU)
Given the likely diagnosis, which of the following is the most likely underlying factor, increasing her risk for this pathology?
Combined oral contraceptive pill
Natural conception
Non-smoker
Pelvic inflammatory disease
Younger age
A 35-year-old women attends the emergency department with acute onset left-sided lower abdominal pain, small amounts of dark brown vaginal discharge and shoulder tip pain.
On further questioning, she has not had a period for around 8 weeks but normally has a regular 30 day cycle. She is currently sexually active with multiple partners, and doesn’t always use contraception. She has also been experiencing diarrhoea and episodes of dizziness for the past 2 days.
A transvaginal ultrasound scan is performed. This shows a gestational sac in the left Fallopian tube.
β-hCG >1500 IU (<5 IU)
Given the likely diagnosis, which of the following is the most likely underlying factor, increasing her risk for this pathology?
Combined oral contraceptive pill
Natural conception
Non-smoker
Pelvic inflammatory disease: increases the chance of an ectopic pregnancy
Younger age
A 23-year-old G1P0 woman, who defaulted all prior antenatal appointments, presents to the obstetrics clinic at 32 weeks’ gestation for her first antenatal visit. The mother appears to be in good health, with no significant past medical history. All her immunisations are up to date.
On examination, the symphyseal-fundal height is noted to be 28cm. An ultrasound scan is performed, which revealed that the fetus’ abdominal circumference is below the 3rd percentile for age, the femur length below the 3rd percentile, while the head circumference is noted to be along the 90th percentile. The baby’s weight is estimated to be below that of the 10th percentile.
Which of the following is the most likely cause for the abnormality noted in this fetus?
Maternal smoking
Singleton gestation
Maternal rubella infection
Maternal age
Early age of menarche
A 23-year-old G1P0 woman, who defaulted all prior antenatal appointments, presents to the obstetrics clinic at 32 weeks’ gestation for her first antenatal visit. The mother appears to be in good health, with no significant past medical history. All her immunisations are up to date.
On examination, the symphyseal-fundal height is noted to be 28cm. An ultrasound scan is performed, which revealed that the fetus’ abdominal circumference is below the 3rd percentile for age, the femur length below the 3rd percentile, while the head circumference is noted to be along the 90th percentile. The baby’s weight is estimated to be below that of the 10th percentile.
Which of the following is the most likely cause for the abnormality noted in this fetus?
Maternal smoking
Singleton gestation
Maternal rubella infection
Maternal age
Early age of menarche
The fetus has features suggestive of small for gestational age, as evidenced by the birth weight below the 10th percentile. Furthermore, fetal measurements is suggestive of a baby that is asymmetrical intrauterine growth restriction (IUGR), as the head circumference is on a significantly higher percentile than that of abdominal circumference and femur length.
A 28-year-old female presents to the GP having just taken a pregnancy test which was positive. As part of her pregnancy over the next 8 months, she has to have frequent blood tests due to the risk of haemolytic disease of the newborn. What is the underlying pathology of this condition?
Fetal production of IgG antibodies against maternal platelets
Fetal production of IgG antibodies against maternal red blood cells
Maternal production of IgG antibodies against fetal red blood cells
Maternal production of IgG antibodies against the fetal bone marrow
Maternal production of IgG antibodies against fetal platelets
A 28-year-old female presents to the GP having just taken a pregnancy test which was positive. As part of her pregnancy over the next 8 months, she has to have frequent blood tests due to the risk of haemolytic disease of the newborn. What is the underlying pathology of this condition?
Fetal production of IgG antibodies against maternal platelets
Fetal production of IgG antibodies against maternal red blood cells
Maternal production of IgG antibodies against fetal red blood cells
Maternal production of IgG antibodies against the fetal bone marrow
Maternal production of IgG antibodies against fetal platelets
During a routine abdominal CT scan for abdominal discomfort and weight loss, a 25-year-old gentleman is found to have enlarged para-aortic lymph nodes.
What area of the body should be checked in this gentleman for a potential malignancy, given the CT findings?
Bladder
Glans penis
Prostate
Rectum
Testes
During a routine abdominal CT scan for abdominal discomfort and weight loss, a 25-year-old gentleman is found to have enlarged para-aortic lymph nodes.
What area of the body should be checked in this gentleman for a potential malignancy, given the CT findings?
Bladder
Glans penis
Prostate
Rectum
Testes
What is the difference between placenta previa and placental abruption? [2]
Placenta previa is when the placenta implants itself very close or over the cervix.
Placental abruption is when the placenta detaches itself from the implantation.

What serum marker may help diagnose SIDS? [1]
Serum 5-HT is significantly elevated in SIDS (specifically intra-platelet)
Which structure forms the posterior border of the lesser sciatic foramen? [1]
Which structure forms the posterior border of the lesser sciatic foramen?
Sacrotuberous ligament
Which muscle divides the greater sciatic foramen into superior and inferior components?
Obturator internus
Adductor magnus
Piriformis
Gluteus minimus
Which muscle divides the greater sciatic foramen into superior and inferior components?
Obturator internus
Adductor magnus
Piriformis
Gluteus minimus
Q
Which muscle lies over sacral plexus?
levator ani
coccygeus
obturator internus
piriformis
Q
Which muscle lies over sacral plexus?
levator ani
coccygeus
obturator internus
piriformis
The [] is a fibromuscular mass which is the site of convergence of perineal and pelvic floor muscles
The perineal body is a fibromuscular mass which is the site of convergence of perineal and pelvic floor muscles
The [] is a fibromuscular mass which is the site of convergence of perineal and pelvic floor muscles
The perineal body is a fibromuscular mass which is the site of convergence of perineal and pelvic floor muscles
Label A-C

a iliococcygeus muscle
b pubococcygeus muscle
c puborectalis muscle
A 17-year-old male has a suspected testicular torsion and the scrotum is to be explored surgically. The surgeon incises the skin and then the dartos muscle. What is the next tissue layer that will be encountered during the dissection?
Visceral layer of the tunica vaginalis
Cremasteric fascia
Parietal layer of the tunica vaginalis
External spermatic fascia
Internal spermatic fascia
A 17-year-old male has a suspected testicular torsion and the scrotum is to be explored surgically. The surgeon incises the skin and then the dartos muscle. What is the next tissue layer that will be encountered during the dissection?
Visceral layer of the tunica vaginalis
Cremasteric fascia
Parietal layer of the tunica vaginalis
External spermatic fascia
Internal spermatic fascia
A 31-year-old woman attends for a routine antenatal clinic visit. She is in her first pregnancy, currently at 32 weeks gestation. She reports feeling quite breathless, and her observations show a heart rate of 90bpm, a blood pressure of 120/80mmHg, a temperature of 36.6ºC, a respiratory rate of 16/min and oxygen saturation of 97%.
An arterial blood gas is done to rule out any respiratory pathology and shows respiratory alkalosis.
What physiological change in pregnancy has occurred to result in this?
Decrease in tidal volume and increase in pulmonary ventilation
Increase in tidal volume and decrease in pulmonary ventilation
Increase in tidal volume and increase in pulmonary ventilation
No change in tidal volume and increase in pulmonary ventilation
No change in tidal volume or pulmonary ventilation
A 31-year-old woman attends for a routine antenatal clinic visit. She is in her first pregnancy, currently at 32 weeks gestation. She reports feeling quite breathless, and her observations show a heart rate of 90bpm, a blood pressure of 120/80mmHg, a temperature of 36.6ºC, a respiratory rate of 16/min and oxygen saturation of 97%.
An arterial blood gas is done to rule out any respiratory pathology and shows respiratory alkalosis.
What physiological change in pregnancy has occurred to result in this?
Decrease in tidal volume and increase in pulmonary ventilation
Increase in tidal volume and decrease in pulmonary ventilation
Increase in tidal volume and increase in pulmonary ventilation
No change in tidal volume and increase in pulmonary ventilation
No change in tidal volume or pulmonary ventilation
A 28-year-old woman delivered a healthy baby at 39+2 by vaginal delivery. There were no complications. Despite firmly wanting to breastfeed, she is having difficulty getting the baby to latch on. Which hormone is responsible for stimulating the production of milk by the alveolar epithelial cells of the breast?
Oxytocin
Prolactin
Oestrogen
Progesterone
Corticotropin-releasing hormone
A 28-year-old woman delivered a healthy baby at 39+2 by vaginal delivery. There were no complications. Despite firmly wanting to breastfeed, she is having difficulty getting the baby to latch on. Which hormone is responsible for stimulating the production of milk by the alveolar epithelial cells of the breast?
Oxytocin
Prolactin
Oestrogen
Progesterone
Corticotropin-releasing hormone
A 60-year-old gentleman presents to his GP with a nodule on his scrotum. A biopsy result shows it to be a squamous cell carcinoma of the scrotum.
Which set of regional lymph nodes are the primary site of lymphatic spread of this tumour?
External iliac
Inguinal
Internal iliac
Para-aortic
Sacral
A 60-year-old gentleman presents to his GP with a nodule on his scrotum. A biopsy result shows it to be a squamous cell carcinoma of the scrotum.
Which set of regional lymph nodes are the primary site of lymphatic spread of this tumour?
External iliac
Inguinal
Internal iliac
Para-aortic
Sacral
Which one of the following vessels provides the greatest contribution to the arterial supply of the breast?
External mammary artery
Thoracoacromial artery
Internal mammary artery
Lateral thoracic artery
Subclavian artery
Which one of the following vessels provides the greatest contribution to the arterial supply of the breast?
External mammary artery
Thoracoacromial artery
Internal mammary artery
Lateral thoracic artery
Subclavian artery
A couple comes in worried that they have been unable to conceive after 18 months of regular unprotected sex. Which of the following is a cause of hypergonadotropic hypogonadism?
Kallmann’s syndrome
Turner’s syndrome
Sheehan’s syndrome
Asherman’s syndrome
Anorexia nervosa
A couple comes in worried that they have been unable to conceive after 18 months of regular unprotected sex. Which of the following is a cause of hypergonadotropic hypogonadism?
Kallmann’s syndrome
Turner’s syndrome
Sheehan’s syndrome
Asherman’s syndrome
Anorexia nervosa
Hypergonadotropic hypogonadism is a failure of the gonads to respond to gonadotropins secreted by the anterior pituitary gland. This is the case in Turner’s syndrome
A 34-year-old woman presents with per vaginal bleeding, immediately after giving birth. Her estimated blood loss is 700ml. What is the most common cause of primary post-partum haemorrhage?
Atony of the uterus
Retained placenta
Clotting disorders
Lacerations to the vulva and/or vagina
Uterine rupture
A 34-year-old woman presents with per vaginal bleeding, immediately after giving birth. Her estimated blood loss is 700ml. What is the most common cause of primary post-partum haemorrhage?
Atony of the uterus
Retained placenta
Clotting disorders
Lacerations to the vulva and/or vagina
Uterine rupture
A gravida 2, para 0 (G2P0) woman at 9 weeks gestation presents to the emergency department with a 2-week history of vomiting. She reports that she has been unable to keep anything down for the last 3 days and now feels exhausted. She also reports 10kg of weight loss since the start of her pregnancy, stating that she now weighs 55kg.
On examination the patient’s eyes are sunken and her mucous membranes appear dry.
A urine dip shows marked ketosis, though is otherwise unremarkable.
What is a risk factor for the most likely diagnosis?
Age >35
Hypothyroidism
Pregnancy with a single foetus
Smoking tobacco
Trophoblastic disease
A gravida 2, para 0 (G2P0) woman at 9 weeks gestation presents to the emergency department with a 2-week history of vomiting. She reports that she has been unable to keep anything down for the last 3 days and now feels exhausted. She also reports 10kg of weight loss since the start of her pregnancy, stating that she now weighs 55kg.
On examination the patient’s eyes are sunken and her mucous membranes appear dry.
A urine dip shows marked ketosis, though is otherwise unremarkable.
What is a risk factor for the most likely diagnosis?
Age >35
Hypothyroidism
Pregnancy with a single foetus
Smoking tobacco
Trophoblastic disease risk factor for hyperemesis gravidarynn
A pregnant woman presents with chronic pelvic pain, deep dyspareunia, dysuria, and odorous green vaginal discharge. She also reports upper right quadrant pain. What is the most likely cause of this upper right quadrant pain?
Cholecystitis
Fitz-Hugh-Curtis syndrome
Pulmonary embolism
Pleurisy
Viral hepatitis
A pregnant woman presents with chronic pelvic pain, deep dyspareunia, dysuria, and odorous green vaginal discharge. She also reports upper right quadrant pain. What is the most likely cause of this upper right quadrant pain?
Cholecystitis
Fitz-Hugh-Curtis syndrome
Pulmonary embolism
Pleurisy
Viral hepatitis
All of the above options may cause upper right quadrant pain, but this woman has presented with pelvic inflammatory disease, and Fitz-Hugh-Curtis syndrome (adhesions of liver to peritoneum) is associated with this condition.
Cholecystitis, pulmonary embolisms, pleurisy and viral hepatitis would not present with dyspareunia, dysuria or vaginal discharge.
A 78-year-old man develops a carcinoma of the scrotum. To which of the following lymph node groups may the tumour initially metastasise?
Para aortic
Obturator
Inguinal
Meso rectal
None of the above
A 78-year-old man develops a carcinoma of the scrotum. To which of the following lymph node groups may the tumour initially metastasise?
Para aortic
Obturator
Inguinal
Meso rectal
None of the above
A 27-year-old new mother is breastfeeding her new baby. The midwife explains that during breastfeeding, the baby suckling on the nipple triggers the release of a compound into the blood that results in the contraction of cells in the mammary glands resulting in milk being pushed out of the nipple.
Which of the following compounds is responsible for this reflex?
Dopamine
Luteinising hormone
Oxytocin
Prolactin
Serotonin
A 27-year-old new mother is breastfeeding her new baby. The midwife explains that during breastfeeding, the baby suckling on the nipple triggers the release of a compound into the blood that results in the contraction of cells in the mammary glands resulting in milk being pushed out of the nipple.
Which of the following compounds is responsible for this reflex?
Dopamine
Luteinising hormone
Oxytocin
Prolactin
Serotonin
Whilst prolactin is important in lactation, it does not trigger milk ejection. It instead triggers production of milk.
A 39-year-old primigravid woman attends the antenatal clinic for her 12-week scan. She is told that the results of the combined test suggested she was at high risk of her fetus having Down’s syndrome.
What were the likely results of her combined test?
↑ HCG, ↑ PAPP-A, increased amount of nuchal fluid
↑ HCG, ↓ PAPP-A, increased amount of nuchal fluid
↑ HCG, ↓ PAPP-A, normal amount of nuchal fluid
↓ HCG, ↓ PAPP-A, decreased amount of nuchal fluid
↓HCG, ↑ PAPP-A, increased amount of nuchal fluid
A 39-year-old primigravid woman attends the antenatal clinic for her 12-week scan. She is told that the results of the combined test suggested she was at high risk of her fetus having Down’s syndrome.
What were the likely results of her combined test?
↑ HCG, ↑ PAPP-A, increased amount of nuchal fluid
↑ HCG, ↓ PAPP-A, increased amount of nuchal fluid
↑ HCG, ↓ PAPP-A, normal amount of nuchal fluid
↓ HCG, ↓ PAPP-A, decreased amount of nuchal fluid
↓HCG, ↑ PAPP-A, increased amount of nuchal fluid
A 35-year-old woman with a history of endometriosis undergoes elective adhesiolysis. The patient has been troubled by pain on micturition, defecation, and intercourse despite pharmacotherapy with the combined oral contraceptive pill.
The surgery is complicated due to widespread endometriotic adhesions. During the operation, the surgeon accidentally divides the ligament that attaches the cervix to the lateral pelvic wall.
What ligament has been injured?
Broad ligament
Cardinal ligament
Pubocervical ligament
Round ligament of the uterus
Uterosacral ligament
A 35-year-old woman with a history of endometriosis undergoes elective adhesiolysis. The patient has been troubled by pain on micturition, defecation, and intercourse despite pharmacotherapy with the combined oral contraceptive pill.
The surgery is complicated due to widespread endometriotic adhesions. During the operation, the surgeon accidentally divides the ligament that attaches the cervix to the lateral pelvic wall.
What ligament has been injured?
Broad ligament
Cardinal ligament - CARDINAL 4 CERVIX
Pubocervical ligament
Round ligament of the uterus - The round ligament of the uterus maintains the anteverted position of the uterus. Clinical significance of the round ligament of the uterus includes round ligament pain, which may present in pregnancy with stretching from a gravid uterus.
Uterosacral ligament
A newborn baby is found to have a brachial plexus injury upon examination. On the affected side, the baby is unable to move his arm properly, which is fixated medially. He is diagnosed with Erb’s palsy. Which of the following risk factors increases the risk of this?
Macrosomia
Low maternal BMI
Maternal diabetes insipidus
Polyhydramnios
Family history of preeclampsia
A newborn baby is found to have a brachial plexus injury upon examination. On the affected side, the baby is unable to move his arm properly, which is fixated medially. He is diagnosed with Erb’s palsy. Which of the following risk factors increases the risk of this?
Macrosomia
Low maternal BMI
Maternal diabetes insipidus
Polyhydramnios
Family history of preeclampsia
A 26-year-old lady, who is 10 weeks pregnant, presents to the Emergency Department with a history of excessive vomiting and feeling unwell. She has not had a booking scan yet. You arrange an ultrasound and notice that the uterus is large for dates. What is the most likely diagnosis?
Normal pregnancy
Ectopic pregnancy
Molar pregnancy
Endometriosis
Fibroids
A 26-year-old lady, who is 10 weeks pregnant, presents to the Emergency Department with a history of excessive vomiting and feeling unwell. She has not had a booking scan yet. You arrange an ultrasound and notice that the uterus is large for dates. What is the most likely diagnosis?
Normal pregnancy
Ectopic pregnancy
Molar pregnancy
Endometriosis
Fibroids
A woman presents with fresh vaginal bleeding immediately following the rupture of her membranes. Fetal heart abnormalities including bradycardias and decelerations are present. Transvaginal ultrasonography confirms that there are ruptured blood vessels which are fetal in origin, which overlie the cervix. What is the most likely cause of her bleeding?
Vasa praevia
Rhesus Disease
Placental abruption
Placental accreta
Cord prolapse
A woman presents with fresh vaginal bleeding immediately following the rupture of her membranes. Fetal heart abnormalities including bradycardias and decelerations are present. Transvaginal ultrasonography confirms that there are ruptured blood vessels which are fetal in origin, which overlie the cervix. What is the most likely cause of her bleeding?
Vasa praevia
Rhesus Disease
Placental abruption
Placental accreta
Cord prolapse
Vasa praevia presents with fresh PV bleeding immediately following membrane rupture, and fetal heart rate abnormalities. Although it does not pose a major risk to the mother it has significant fetal mortality
A young woman presents with pelvic pain occurring during her periods, with ‘deep’ pain during intercourse and pain on defecation during this time. She states that her periods are regular with little bleeding. What is the most likely diagnosis?
Pelvic inflammatory disease
Endometriosis
Fibroids
Adenomyosis
Premenstrual syndrome
A young woman presents with pelvic pain occurring during her periods, with ‘deep’ pain during intercourse and pain on defecation during this time. She states that her periods are regular with little bleeding. What is the most likely diagnosis?
Pelvic inflammatory disease
Endometriosis
Fibroids
Adenomyosis
Premenstrual syndrome
A 48-year-old female presents to the day surgery unit for a bilateral salpingo-oophorectomy. The surgeon explains the procedure to her.
Which of the following ligaments would the surgeon have to open to access the ovaries and the fallopian tubes?
Broad ligament
Cardinal ligament
Ovarian ligament
Round ligament
Uterosacral ligament
A 48-year-old female presents to the day surgery unit for a bilateral salpingo-oophorectomy. The surgeon explains the procedure to her.
Which of the following ligaments would the surgeon have to open to access the ovaries and the fallopian tubes?
Broad ligament
Cardinal ligament
Ovarian ligament
Round ligament
Uterosacral ligament
A 17-year-old girl has missed her period by 6 days, which is unusual given her regular 30-day cycle. She buys a pregnancy test and tests positive. On fertilisation of the egg, the sperm stimulates the release of which substance to prevent polyspermy?
Lysozymes
Sodium ions
Phosphate ions
Potassium ions
Calcium ions
A 17-year-old girl has missed her period by 6 days, which is unusual given her regular 30-day cycle. She buys a pregnancy test and tests positive. On fertilisation of the egg, the sperm stimulates the release of which substance to prevent polyspermy?
Lysozymes
Sodium ions
Phosphate ions
Potassium ions
Calcium ions
A 29-year-old woman, who is 10 weeks pregnant with twins, presents to the emergency department suffering from worsening nausea and vomiting over the last 3 weeks. This is her second pregnancy. Her first pregnancy had a number of complications. Her first baby was large for gestational age, and she suffered from hypertension of pregnancy. The doctor diagnoses her with hyperemesis gravidarum (HG).
What from this history is a key risk factor for developing HG?
Hypertension of pregnancy
Large for gestational age
Multiparity
Multiple pregnancy
Pre-eclampsia
A 29-year-old woman, who is 10 weeks pregnant with twins, presents to the emergency department suffering from worsening nausea and vomiting over the last 3 weeks. This is her second pregnancy. Her first pregnancy had a number of complications. Her first baby was large for gestational age, and she suffered from hypertension of pregnancy. The doctor diagnoses her with hyperemesis gravidarum (HG).
What from this history is a key risk factor for developing HG?
Hypertension of pregnancy
Large for gestational age
Multiparity
Multiple pregnancy
Risk factors for HG include trophoblastic disease, multiple pregnancies, molar pregnancy and previous hyperemesis.
Pre-eclampsia
A 29-year-old woman presents to the emergency department at her local hospital. She is 10 weeks pregnant and has been suffering from persistent nausea and vomiting. She is clinically dehydrated and admits to losing 8kg over the last month.
What condition is a risk factor for the most likely diagnosis?
Foetus small for gestational age
Gestational diabetes
Pre-eclampsia
Single pregnancies
Trophoblastic disease
A 29-year-old woman presents to the emergency department at her local hospital. She is 10 weeks pregnant and has been suffering from persistent nausea and vomiting. She is clinically dehydrated and admits to losing 8kg over the last month.
What condition is a risk factor for the most likely diagnosis?
Foetus small for gestational age
Gestational diabetes
Pre-eclampsia
Single pregnancies
Trophoblastic disease
A 30-year-old woman at 41 weeks gestation is in labour. The baby’s head is delivered but a minute of gentle traction has failed to deliver the shoulders. What is the first intervention that should be used to try and overcome shoulder dystocia once it has been identified?
Oxytocin administration
McRoberts manoeuvre
Urgent episiotomy
Symphysiotomy
Zavanelli manoeuvre
A 30-year-old woman at 41 weeks gestation is in labour. The baby’s head is delivered but a minute of gentle traction has failed to deliver the shoulders. What is the first intervention that should be used to try and overcome shoulder dystocia once it has been identified?
Oxytocin administration
McRoberts manoeuvre
Urgent episiotomy
Symphysiotomy
Zavanelli manoeuvre
Rose is a 34-year-old female who has been in a relationship for 4 years. Rose and her partner have been trying to conceive regularly for over a year without success. They have visited their GP to organise some investigations into a possible cause. Which hormone is released after ovulation occurs and can be used as a marker of fertility?
Luteinising hormone (LH)
Follicle stimulating hormone (FSH)
Oestrogen
Testosterone
Progesterone
Rose is a 34-year-old female who has been in a relationship for 4 years. Rose and her partner have been trying to conceive regularly for over a year without success. They have visited their GP to organise some investigations into a possible cause. Which hormone is released after ovulation occurs and can be used as a marker of fertility?
Luteinising hormone (LH)
Follicle stimulating hormone (FSH)
Oestrogen
Testosterone
Progesterone Day 21 progesterone, also known as mid-luteal cycle progesterone, is used to test for ovulation if the woman has a regular cycle. If irregular, then you need to test progesterone a week before predicted menstruation.
A 28-year-old woman who is 36 weeks into her first pregnancy is rushed to the hospital due to a blood pressure of 160/110mmHg. She is also found to have proteinuria and is complaining of a headache, blurred vision, and abdominal pain. What characteristic finding would be expected in this situation?
Tachycardia and hypotension
Bradycardia, hypertension and respiratory irregularity
Haemolysis, elevated liver enzymes and low platelets
Facial oedema, rash and stridor
Warm peripheries, rigors and bounding pulse
A 28-year-old woman who is 36 weeks into her first pregnancy is rushed to the hospital due to a blood pressure of 160/110mmHg. She is also found to have proteinuria and is complaining of a headache, blurred vision, and abdominal pain. What characteristic finding would be expected in this situation?
Tachycardia and hypotension
Bradycardia, hypertension and respiratory irregularity
Haemolysis, elevated liver enzymes and low platelets
Facial oedema, rash and stridor
Warm peripheries, rigors and bounding pulse
The history indicates pre-eclampsia. This is characterised by hypertension and proteinuria with onset after 20 weeks of pregnancy. Blood pressure should be managed with anti-hypertensives. Woman with this condition may develop the HELLP syndrome. This is characterised by haemolysis (raised LDH), elevated liver enzymes and low platelets.
What is the main mechanism of action of the combined oral contraceptive pill?
Causes fallopian tube dysfunction
Thickens cervical mucus
Thins endometrial lining
Prevents implantation
Inhibition of ovulation
What is the main mechanism of action of the combined oral contraceptive pill?
Causes fallopian tube dysfunction
Thickens cervical mucus
Thins endometrial lining
Prevents implantation
Inhibition of ovulation
A 20-year-old woman comes in requiring contraception and wants to find out more about the combined oral contraceptive pill. She has heard it can cause cancer and wants to find out more about its risks. Which of the following is the correct advice you can tell her?
There is no evidence that the combined oral contraceptive pill causes increased risk of cancer
The combined oral contraceptive pill increases the risk of breast and cervical cancer but is protective against ovarian and endometrial cancer
The combined oral contraceptive pill increases the risk of breast and ovarian cancer
The combined oral contraceptive pill decreases the risk of breast cancer but increases the risk of endometrial and ovarian cancer
Only after 10 years of use does the combined oral contraceptive pill increase the risk of breast cancer
A 20-year-old woman comes in requiring contraception and wants to find out more about the combined oral contraceptive pill. She has heard it can cause cancer and wants to find out more about its risks. Which of the following is the correct advice you can tell her?
There is no evidence that the combined oral contraceptive pill causes increased risk of cancer
The combined oral contraceptive pill increases the risk of breast and cervical cancer but is protective against ovarian and endometrial cancer
The combined oral contraceptive pill increases the risk of breast and ovarian cancer
The combined oral contraceptive pill decreases the risk of breast cancer but increases the risk of endometrial and ovarian cancer
Only after 10 years of use does the combined oral contraceptive pill increase the risk of breast cancer
A pregnant woman comes in to see the doctor as her husband is concerned about her breathing becoming deeper. Chest examination is unremarkable. Her respiratory rate is 16/min. Which explanation should be provided to this couple?
This is abnormal and requires referral for further assessment
This is normal and caused by progesterone
This is abnormal and should be monitored by her GP
This is normal and caused by testosterone
This is normal and caused by oestrogen
A pregnant woman comes in to see the doctor as her husband is concerned about her breathing becoming deeper. Chest examination is unremarkable. Her respiratory rate is 16/min. Which explanation should be provided to this couple?
This is abnormal and requires referral for further assessment
This is normal and caused by progesterone
This is abnormal and should be monitored by her GP
This is normal and caused by testosterone
This is normal and caused by oestrogen
If a women has endometriosis and pain when defecating, where are the locations that might get likely accumulation of blood from the extra-pelvic endometrial tissue? [2]
Pouch of Douglas
Bowel
A 24-year-old woman presents to the emergency department with severe left-sided pelvic pain. She also reports amenorrhoea. On clinical examination, the doctor elicits pelvic tenderness. A pregnancy test shows a positive result, and subsequently, a transvaginal ultrasound is performed. This identifies a tubal ectopic pregnancy, and a fetal heartbeat is detected. Therefore, a laparoscopic salpingectomy is performed.
Within what anatomical structure is this pathology most likely contained?
Broad ligament
Cardinal ligament
Ovarian ligament
Round ligament
Uterosacral ligament
A 24-year-old woman presents to the emergency department with severe left-sided pelvic pain. She also reports amenorrhoea. On clinical examination, the doctor elicits pelvic tenderness. A pregnancy test shows a positive result, and subsequently, a transvaginal ultrasound is performed. This identifies a tubal ectopic pregnancy, and a fetal heartbeat is detected. Therefore, a laparoscopic salpingectomy is performed.
Within what anatomical structure is this pathology most likely contained?
Broad ligament Broad ligament contains the Fallopian tubes
Cardinal ligament
Ovarian ligament
Round ligament
Uterosacral ligament
You are reviewing a 3-week old baby boy who is bought in by his mum. Percy was born vaginally at term at the local hospital. He became unwell straight after birth and was treated for neonatal sepsis in the neonatal intensive care unit. Fortunately, he recovered well and was discharged after 7 days.
What is the most common cause of sepsis in this age group?
Escherichia coli
Listeria monocytogenes
Streptococcus pneumoniae
Group B Streptococcus
Haemophilus influenza
You are reviewing a 3-week old baby boy who is bought in by his mum. Percy was born vaginally at term at the local hospital. He became unwell straight after birth and was treated for neonatal sepsis in the neonatal intensive care unit. Fortunately, he recovered well and was discharged after 7 days.
What is the most common cause of sepsis in this age group?
Escherichia coli
Listeria monocytogenes
Streptococcus pneumoniae
Group B Streptococcus
Haemophilus influenza
A 40-year-old lady with a background of endometriosis is undergoing a hysterectomy. The gynaecology registrar when undertaking the procedure notes the ureter’s position in relation to the uterus. What is the position of the ureter in relation to the surrounding blood vessels?
Ureter crosses pelvic brim at aortic bifurcation
Ureter passes above ovarian artery
Ureter passes above uterine artery
Ureter passes underneath ovarian artery
Ureter passes underneath uterine artery
A 40-year-old lady with a background of endometriosis is undergoing a hysterectomy. The gynaecology registrar when undertaking the procedure notes the ureter’s position in relation to the uterus. What is the position of the ureter in relation to the surrounding blood vessels?
Ureter crosses pelvic brim at aortic bifurcation
Ureter passes above ovarian artery
Ureter passes above uterine artery
Ureter passes underneath ovarian artery
Ureter passes underneath uterine artery
A 24-year-old woman presents to her GP, she is 11 weeks postpartum. She is complaining of pain in her left breast when breastfeeding and is worried about continuing to feed her baby.
On examination, there is a 2cm x 2cm erythematous lesion on the left breast. On palpation, it is tender and hot to touch. The right breast appears normal.
The patient has a temperature of 38.2ºC and so the GP decides to prescribe antibiotics. She also encourages the patient to continue breastfeeding.
What is the main site of lymphatic drainage for the area of infection?
Contralateral axillary nodes
Infraclavicular nodes
Ipsilateral axillary nodes
Parasternal nodes
Supraclavicular nodes
A 24-year-old woman presents to her GP, she is 11 weeks postpartum. She is complaining of pain in her left breast when breastfeeding and is worried about continuing to feed her baby.
On examination, there is a 2cm x 2cm erythematous lesion on the left breast. On palpation, it is tender and hot to touch. The right breast appears normal.
The patient has a temperature of 38.2ºC and so the GP decides to prescribe antibiotics. She also encourages the patient to continue breastfeeding.
What is the main site of lymphatic drainage for the area of infection?
Contralateral axillary nodes
Infraclavicular nodes
Ipsilateral axillary nodes Axillary nodes are the main site of lymphatic drainage for the breast
Parasternal nodes
Supraclavicular nodes
A 28-year-old primigravida woman who is in her third trimester presents for her antenatal check up.
An ultrasound scan reveals a smaller than normal fetal abdominal circumference. Fetal head circumference is normal and there are no congenital abnormalities detected. A diagnosis of asymmetrical intrauterine growth reduction is made.
Which of the following is the most likely cause of the condition in this scenario?
Down syndrome
Early intrauterine infection
Prolonged maternal malnutrition
Underlying maternal hypothyroidism
Placental insufficiency
A 28-year-old primigravida woman who is in her third trimester presents for her antenatal check up.
An ultrasound scan reveals a smaller than normal fetal abdominal circumference. Fetal head circumference is normal and there are no congenital abnormalities detected. A diagnosis of asymmetrical intrauterine growth reduction is made.
Which of the following is the most likely cause of the condition in this scenario?
Down syndrome
Early intrauterine infection
Prolonged maternal malnutrition
Underlying maternal hypothyroidism
Placental insufficiency
A young girl has the ovarian cycle explained to her by her GP, at a routine appointment. The GP explains that the theca of the pre-antral follicle contains hormone receptors which facilitate production of large amounts of hormones. Which type of receptor is found on the theca?
FSH receptors
LH receptors
Progesterone receptors
Testosterone receptors
Oestrogen receptors
A young girl has the ovarian cycle explained to her by her GP, at a routine appointment. The GP explains that the theca of the pre-antral follicle contains hormone receptors which facilitate production of large amounts of hormones. Which type of receptor is found on the theca?
FSH receptors
LH receptors LH interacts with thecal LH receptors to produce androstenedione, which is converted into oestradiol by aromatase in granulosa cells.
Progesterone receptors
Testosterone receptors
Oestrogen receptors
A young girl has the ovarian cycle explained to her by her GP, at a routine appointment. The GP explains that the follicle produces hormones which prepare the womb for embryo implantation. Which part of the follicle does this?
Granulosa cells
Zona pellucida
Theca
Antrum
Cumulus oophorus
A young girl has the ovarian cycle explained to her by her GP, at a routine appointment. The GP explains that the follicle produces hormones which prepare the womb for embryo implantation. Which part of the follicle does this?
Granulosa cells
Zona pellucida
Theca
Antrum
Cumulus oophorus
A 72-year-old man develops a hydrocele which is being surgically managed. As part of the procedure the surgeons divide the tunica vaginalis. From which of the following is this structure derived?
Peritoneum
External oblique aponeurosis
Internal oblique aponeurosis
Transversalis fascia
Rectus sheath
A 72-year-old man develops a hydrocele which is being surgically managed. As part of the procedure the surgeons divide the tunica vaginalis. From which of the following is this structure derived?
Peritoneum
External oblique aponeurosis
Internal oblique aponeurosis
Transversalis fascia
Rectus sheath
A 28-year-old primigravida is undergoing a routine physical examination and blood tests as part of her 12-week booking appointment. She has no relevant past medical or drug history. She is well and reports no symptoms associated with her pregnancy thus far. The physical examination is unremarkable but urinalysis reveals trace glycosuria.
What is the most likely diagnosis?
Gestational diabetes
Normal finding
Pre-diabetes
Pre-eclampsia
Type 2 diabetes
A 28-year-old primigravida is undergoing a routine physical examination and blood tests as part of her 12-week booking appointment. She has no relevant past medical or drug history. She is well and reports no symptoms associated with her pregnancy thus far. The physical examination is unremarkable but urinalysis reveals trace glycosuria.
What is the most likely diagnosis?
Gestational diabetes
Normal finding - Trace glycosuria is common in pregnancy due to the increased GFR and reduction in tubular reabsorption of filtered glucose
Pre-diabetes
Pre-eclampsia
Type 2 diabetes
Which of the following is a correct description of the proliferative phase of the menstrual cycle?
Oestrogen produced by the follicle results in the thickening of the endometrium and the formation of spiral arteries and glands
Progesterone from the corpus luteum acts upon the endometrium to stimulate the endometrial glands
Fall in progesterone and oestrogen results in the degeneration of the endometrium
Occurs between days 15-28
FSH and LH cause the follicle to grow and mature
Which of the following is a correct description of the proliferative phase of the menstrual cycle?
Oestrogen produced by the follicle results in the thickening of the endometrium and the formation of spiral arteries and glands
Progesterone from the corpus luteum acts upon the endometrium to stimulate the endometrial glands
Fall in progesterone and oestrogen results in the degeneration of the endometrium
Occurs between days 15-28
FSH and LH cause the follicle to grow and mature
A 29-year-old pregnant woman in her third trimester presents to her GP for the results of her routine blood tests:
Hb 102 g/L Female: (115 - 160)
Platelets 190 * 109/L (150 - 400)
WBC 9 * 109/L (4.0 - 11.0)
What is the most likely reason for this patient’s anaemia? [1]
Haemodilution
In pregnancy, maternal blood volume up 30% - red cells up 20% but plasma up 50% → Hb falling
A 22 year old lady presents with lump in the right breast. She reports it has been present for around 4 months but she has grown increasingly concerned as it has not gone away. On examination there is a 2cm smooth lump in the right breast. It is mobile and not fixed to the skin. There are no nipple or skin changes. What is the most likely diagnosis?
Breast cyst
Ductal carcinoma-in-situ
Fat necrosis
Fibroadenoma
Breast abscess
A 22 year old lady presents with lump in the right breast. She reports it has been present for around 4 months but she has grown increasingly concerned as it has not gone away. On examination there is a 2cm smooth lump in the right breast. It is mobile and not fixed to the skin. There are no nipple or skin changes. What is the most likely diagnosis?
Breast cyst
Ductal carcinoma-in-situ
Fat necrosis
Fibroadenoma
Breast abscess
Fibroadenomas are the most common breast lumps in women aged 15-25. They are typically less than 3cm in size, are firm and mobile. They are not concerning and tend to resolve over a few years.
Fat necrosis occurs after trauma to the breast e.g. from a sports injury or following procedures such as core needle biopsy. The area may be tender with visible bruising. It is usually self-resolving and unlikely to persist for this long
You are the junior doctor based in a reproductive medicine clinic. A patient asks you whether women have eggs in their ovaries when they are born and you give her a simple explanation of oogenesis. Up to what stage of oogenesis do cells develop in utero?
Metaphase II
Metaphase I
Prophase I
Prophase II
Anaphase II
You are the junior doctor based in a reproductive medicine clinic. A patient asks you whether women have eggs in their ovaries when they are born and you give her a simple explanation of oogenesis. Up to what stage of oogenesis do cells develop in utero?
Metaphase II
Metaphase I
Prophase I
Prophase II
Anaphase II
A 30-year-old woman, Gwen, presents to her GP for advice about conception. She wants to know how soon after having sex she can take a urine pregnancy test and get an accurate result.
Commercially available urine pregnancy tests detect hCG in the urine.
Why does the GP advise Gwen to wait to take the test until the first day of her missed menstrual period for the best chance of an accurate result?
HCG is secreted by the blastocyst after hatching from the zona pellucida
HCG is secreted by the corpus luteum after formation of the bilaminar disc
HCG is secreted by the syncytiotrophoblast after implantation
The ovary produces hCG immediately after fertilisation, but levels are not high enough to detect in the urine until after a few days
The zygote produces hCG immediately, but levels are not high enough to detect in the urine until after a few days
A 30-year-old woman, Gwen, presents to her GP for advice about conception. She wants to know how soon after having sex she can take a urine pregnancy test and get an accurate result.
Commercially available urine pregnancy tests detect hCG in the urine.
Why does the GP advise Gwen to wait to take the test until the first day of her missed menstrual period for the best chance of an accurate result?
HCG is secreted by the blastocyst after hatching from the zona pellucida
HCG is secreted by the corpus luteum after formation of the bilaminar disc
HCG is secreted by the syncytiotrophoblast after implantation
The ovary produces hCG immediately after fertilisation, but levels are not high enough to detect in the urine until after a few days
The zygote produces hCG immediately, but levels are not high enough to detect in the urine until after a few days
A 55-year-old postmenopausal lady is undergoing investigation for vaginal bleeding. The bleeding has been ongoing for the last 2 months, and there is no family history of malignancy. Her recent cervical smear reported no abnormalities. On transvaginal ultrasound, it is demonstrated that the endometrial thickness is 6 mm. What should be the next step?
Serum oestrogen & progestogen
Magnetic Resonance Imaging
Computed Tomography scan
Endometrial biopsy
Serum LH/FSH
A 55-year-old postmenopausal lady is undergoing investigation for vaginal bleeding. The bleeding has been ongoing for the last 2 months, and there is no family history of malignancy. Her recent cervical smear reported no abnormalities. On transvaginal ultrasound, it is demonstrated that the endometrial thickness is 6 mm. What should be the next step?
Serum oestrogen & progestogen
Magnetic Resonance Imaging
Computed Tomography scan
Endometrial biopsy - Postmenopausal bleeding should always alert a medical professional to the possibility of endometrial cancer. NICE guidelines (2015) recommend an urgent 2-week referral for women aged 55 or over with post-menopausal bleeding.
Serum LH/FSH
A 14-year-old boy is feeling self-conscious that he is the shortest in the class and his voice has not ‘broken’ yet. His mother attends the GP with him and a thorough history and examination are carried out. The doctor reassures him that he is developing within the normal range and explains that puberty occurs at different times for everyone. Which cells secrete testosterone in the testes?
Spermatogonia stem cells
Myoid cells
Leydig cells
Sertoli cells
Fibroblasts
A 14-year-old boy is feeling self-conscious that he is the shortest in the class and his voice has not ‘broken’ yet. His mother attends the GP with him and a thorough history and examination are carried out. The doctor reassures him that he is developing within the normal range and explains that puberty occurs at different times for everyone. Which cells secrete testosterone in the testes?
Spermatogonia stem cells
Myoid cells
Leydig cells
Sertoli cells
Fibroblasts
A midwife calls the obstetric Foundation Year 2 doctor to review her patient, a 33-year-old woman who had a spontaneous vaginal delivery one hour ago. The patient has ongoing vaginal bleeding and the midwife estimates that she has lost 600 millilitres of blood in total. What is the most common cause of primary postpartum haemorrhage?
Retained products of conception
Uterine rupture
Perineal trauma
Uterine inversion
Uterine atony
A midwife calls the obstetric Foundation Year 2 doctor to review her patient, a 33-year-old woman who had a spontaneous vaginal delivery one hour ago. The patient has ongoing vaginal bleeding and the midwife estimates that she has lost 600 millilitres of blood in total. What is the most common cause of primary postpartum haemorrhage?
Retained products of conception
Uterine rupture
Perineal trauma
Uterine inversion
Uterine atony
A worried parent brings their 16-year-old daughter to the general practice, concerned that she has not yet started her periods.
The 16-year-old has got breast bud development, although menstruation has not started. A pregnancy test is negative.
What is the most likely diagnosis?
Endometriosis
Normal variation
Obesity-induced amenorrhoea
Primary amenorrhoea
Secondary amenorrhoea
A worried parent brings their 16-year-old daughter to the general practice, concerned that she has not yet started her periods.
The 16-year-old has got breast bud development, although menstruation has not started. A pregnancy test is negative.
What is the most likely diagnosis?
Endometriosis
Normal variation
Obesity-induced amenorrhoea
Primary amenorrhoea Primary amenorrhoea is defined as the failure to establish menstruation by 15 years of age in girls with normal secondary sexual characteristics (such as breast development), or by 13 years of age in girls with no secondary sexual characteristics
Secondary amenorrhoea
What drug do you give to prevent develoment of pre-eclmapsia to eclampsia? [1]
MgS [1]
Which molecules from placenta causes the increase in oestrogen that causes hyperemesis gravidarum? [2]
GDF15 - interacts with NTS and makes GFRAL

Which type of pregnancy does twin-twin infusion occur in? [1]
Only affects mono-chorionic pregnancies
If a women has endometriosis and pain when defecating, where are the locations that might get likely accumulation of blood from the extra-pelvic endometrial tissue? [2]
Pouch of Douglas
Bowel
Intracranial atherosclerosis, Hydrocephalus & Chorioretinitis would inidcate which disease? [1]
**congenital toxoplasmosis **
Describe what the arrows are highlighting on this CTG? [1]

Variable decelerations
What are the arrows highlighting on this CTG? [1]

Late decelerations
Which of the following is the correct definition of decelerations on cardiotocography (CTG)?
Abrupt decrease in baseline heart rate of >20 bpm for >15 seconds
Abrupt decrease in baseline heart rate of >10 bpm for >10 seconds
Abrupt decrease in baseline heart rate of >20 bpm for >20 seconds
Abrupt decrease in baseline heart rate of >5 bpm for >10 seconds
Abrupt decrease in baseline heart rate of >15 bpm for >15 seconds
Which of the following is the correct definition of decelerations on cardiotocography (CTG)?
Abrupt decrease in baseline heart rate of >20 bpm for >15 seconds
Abrupt decrease in baseline heart rate of >10 bpm for >10 seconds
Abrupt decrease in baseline heart rate of >20 bpm for >20 seconds
Abrupt decrease in baseline heart rate of >5 bpm for >10 seconds
Abrupt decrease in baseline heart rate of >15 bpm for >15 seconds
Which of the following would be classed as a reassuring amount of variability on a CTG?
More than 25 bpm for more than 25 minutes
More than 25 bpm for 15-25 minutes
Less than 5 bpm for between 30-50 minutes
5–25 bpm for 30 minutes
Less than 5 bpm for more than 50 minutes
Which of the following would be classed as a reassuring amount of variability on a CTG?
More than 25 bpm for more than 25 minutes
More than 25 bpm for 15-25 minutes
Less than 5 bpm for between 30-50 minutes
5–25 bpm for 30 minutes
Less than 5 bpm for more than 50 minutes
What are the arrows highlighting on this CTG?
Late decelerations
Prolonged decelerations
Early decelerations
Sinusoidal pattern
Variable decelerations

What are the arrows highlighting on this CTG?
Late decelerations
Prolonged decelerations
Early decelerations
Sinusoidal pattern
Variable decelerations
Which of the following is the correct definition of an acceleration on a cardiotocogram (CTG)?
Abrupt increase in baseline heart rate of >15 bpm for >10 seconds
Abrupt increase in baseline heart rate of >5 bpm for >15 seconds
Abrupt increase in baseline heart rate of >5 bpm for >5 seconds
Abrupt increase in baseline heart rate of >10 bpm for >20 seconds
Abrupt increase in baseline heart rate of >15 bpm for >15 seconds
Which of the following is the correct definition of an acceleration on a cardiotocogram (CTG)?
Abrupt increase in baseline heart rate of >15 bpm for >10 seconds
Abrupt increase in baseline heart rate of >5 bpm for >15 seconds
Abrupt increase in baseline heart rate of >5 bpm for >5 seconds
Abrupt increase in baseline heart rate of >10 bpm for >20 seconds
Abrupt increase in baseline heart rate of >15 bpm for >15 seconds
Male infertility:
What % of all sperm needs to be normal for classification of all sperm? [1]
What % of all sperm needs to have progressive motility for normal classification of sperm? [1]
To be classified as normal:
Only 4% needs to be normal
Progresive motility needs to be 32%
What is labelled A
Chlamdyia infection
Endometriosis
Fibroids
Gonorrhea infection
Polycysitc ovary syndrome

What is labelled A
Chlamdyia infection
Endometriosis
Fibroids
Gonorrhea infection
Polycysitc ovary syndrome
What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18

Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18
What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18

What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18
What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18

What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18
What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18

What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18
What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18

What is this image
Herpes Simplex 1
Herpes Simplex 2
HPV 6
HPV 16
HPV 18
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis - penile chancre
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis - Congenital syphilis exhibiting classic skin rash
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis - Congenital syphilis - Hutchinson’s teeth
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia - LGV lymphadenopathy
Syphilis
HPV 16
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6
What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6

What is this image
Gonorrhoea
Herpes simplex 2
Chlamydia
Syphilis
HPV 6
What is this image depicted of the female reproductive tract [1]

Endometriosis
A cyanotic newborn is diagnosed with transposition of the great arteries. Which of the following medications should be administered, whilst awaiting surgical treatment, to maintain patency of the ductus arteriosus?
Indomethacin
Ibuprofen
Prostacyclin
Paracetamol
Alprostadil
A cyanotic newborn is diagnosed with transposition of the great arteries. Which of the following medications should be administered, whilst awaiting surgical treatment, to maintain patency of the ductus arteriosus?
Indomethacin
Ibuprofen
Prostacyclin
Paracetamol
Alprostadil Alprostadil
This is prostaglandin E1. Prostaglandins will prevent the ductus arteriosus from closing
A 3-year-old girl is brought to the general practitioner. She has been distressed with otalgia, pulling her left ear for 12 hours. Just before arriving at the practice, the mother notices a smelling fluid discharge from her daughter’s left ear. Since then, her otalgia has resolved.
What is the most likely diagnosis?
Otitis media with effusion
Cholesteatoma
Acute otitis media
Acute mastoiditis
Acute otitis externa
A 3-year-old girl is brought to the general practitioner. She has been distressed with otalgia, pulling her left ear for 12 hours. Just before arriving at the practice, the mother notices a smelling fluid discharge from her daughter’s left ear. Since then, her otalgia has resolved.
What is the most likely diagnosis?
Otitis media with effusion
Cholesteatoma
Acute otitis media
Acute mastoiditis
Acute otitis externa
A 5 year old boy presents to the GP with his father. He has had a fever, runny nose and cough over the last few days and has now developed a red rash all over his body. His father is uncertain about which immunisations the boy has received. On examination the boy has an erythematous, blanching maculopapular rash all over, with grey spots on his buccal mucosa.
Which of the following is the most likely cause of his symptoms?
Hand, foot and mouth disease
Bechet’s disease
Mumps
Scarlet fever
Measles
A 5 year old boy presents to the GP with his father. He has had a fever, runny nose and cough over the last few days and has now developed a red rash all over his body. His father is uncertain about which immunisations the boy has received. On examination the boy has an erythematous, blanching maculopapular rash all over, with grey spots on his buccal mucosa.
Which of the following is the most likely cause of his symptoms?
Hand, foot and mouth disease
Bechet’s disease
Mumps
Scarlet fever
Measles
A rash with fever in the context of an incomplete or uncertain immunisation history should be considered as measles. This boy also has Koplik’s spots on his buccal mucosa which supports the diagnosis
Which neurotransmitter does oestrogen cause an incease in? [1]
Serotonin
Which congenital heart defect can be identified in this image?
Patent foramen ovale
Atrial septal defect
Patent ductus arteriosus
Ventricular septal defect
Tetralogy of Fallot

Which congenital heart defect can be identified in this image?
Patent foramen ovale
Atrial septal defect
Patent ductus arteriosus
Ventricular septal defect
Tetralogy of Fallot
what is the cell indicated?
- mesothelial cell
- syncytiotrophoblast
- mesenchymal cell
- cytotrophoblast
- endothelial cell
- decidual cell

what is the cell indicated?
- mesothelial cell
2. syncytiotrophoblast - mesenchymal cell
- cytotrophoblast
- endothelial cell
6. decidual cell
which cells are indicated by the }
- pellucidal cells
- theca externa cells
- fibroblasts
- theca interna cells
- granulosa cells
- granulosa lutein cells 7. theca l

which cells are indicated by the }
- pellucidal cells
- theca externa cells
- fibroblasts
4. theca interna cells - granulosa cells
6. granulosa lutein cells - theca lutein cells
In the ovary, the first layer of stromal cells that organise around the growing follicle is called the Feedback: theca interna. These theca interna cells help to synthesise estrogens.
This is an organ of the male reproductive system. The structures cut in cross section here are lined by
acinar glandular epithelium
- germinal epithelium
- simple cuboidal epithelium
- stratified columnar epithelium
- stratified cuboidal epithelium
- pseudostratified columnar epithelium
- stratified squamous epithelium

This is an organ of the male reproductive system. The structures cut in cross section here are lined by
acinar glandular epithelium 2. germinal epithelium 3. simple cuboidal epithelium 4. stratified columnar epithelium 5. stratified cuboidal epithelium **6. pseudostratified columnar epithelium** 7. stratified squamous epithelium
This is a diagram of the mature placenta and associated maternal structures. What is indicated by A?
- chorion
- amnion
- stratum basalis of the endometrium
- decidua capsularis
- myometrium
- decidua basalis
This is a diagram of the mature placenta and associated maternal structures. What is indicated by A?
- chorion
- amnion
- stratum basalis of the endometrium
- decidua capsularis
- myometrium
* *6. decidua basalis
The decidua basalis is the maternal part of the placenta derived from the endometrial tissue where the embryo implanted.**

What is the name of the fetal shunt shown in the diagram?
- umbilical vein
- foramen ovale
- ductus venosus
- ductus ateriosus
- ligamentum teres

What is the name of the fetal shunt shown in the diagram?
- umbilical vein
2. foramen ovale - ductus venosus
- ductus ateriosus
5. ligamentum teres
what type of hernia is shown here?
Indirect inguinal hernia
- Direct inguinal hernia
- Femoral hernia
- Incisional hernia
- Congenital inguinal hernia

what type of hernia is shown here?
- Indirect inguinal hernia
2. Direct inguinal hernia - Femoral hernia
- Incisional hernia
5. Congenital inguinal hernia
In this sagittal section of the female pelvis, which of the labelled structures is mainly supplied by the gonadal artery?
C
D
E
F
H

In this sagittal section of the female pelvis, which of the labelled structures is mainly supplied by the gonadal artery?
C
D
E
F
H
**In this sagittal section of the female pelvis, the structure labelled F is an ovary and is mainly supplied by the gonadal artery.
The ovarian artery is the main arterial supply to the gonads in females.**

What is the structure labelled B?
Vas deferens
Prostate
Internal urethral orifice
Ureter
Seminal vesicle

What is the structure labelled B?
Vas deferens
Prostate
Internal urethral orifice
Ureter
Seminal vesicle
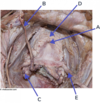
Which of the following relaxes pubic symphysis during labour?
Oxytocin
Oestrogen
Progesterone
Androstenedione
Vasopressin
Which of the following relaxes pubic symphysis during labour?
Oxytocin
Oestrogen
Progesterone
Androstenedione
Vasopressin
Venous blood from which structure is drained into A?
Right ovary
Right testicle
Left testicle
Right kidney
Spleen

Venous blood from which structure is drained into A?
Right ovary
Right testicle
Left testicle
Right kidney
Spleen
Venous blood from the left testicle is drained via the left testicular vein into the left renal vein.
However, the right testicular vein drains directly into the IVC, whereas the left testicular vein drains into the left renal vein, before the IVC is reached. Compression of the left renal vein can thus impede venous blood drainage from the left testicle, possibly resulting in a varicocoele.

In this prosection of a female in the lithotomy position, identify A
A. perineal body B. bulbospongiosus C. greater vestibular (Bartholin's) gland D. Cowper's gland E. crus of clitoris

A. perineal body B. bulbospongiosus **C. greater vestibular (Bartholin's) gland** D. Cowper's gland E. crus of clitoris
Ovary: What type of follicle is labelled A?
1. Secondary (antral) 2. Primordial 3. Growing 4. Atretic 5. Primary 6. Graafian

Ovary: What type of follicle is labelled A?
1. Secondary (antral) 2. Primordial **3. Growing** 4. Atretic 5. Primary 6. Graafian
Having several layers of granulosa cells, this is a growing follicle. There
is no antrum.
What is A?
A. vas deferens B. ejaculatory duct C. testicular artery D. spermatic cord E. ilioinguinal nerve F. genitofemoral nerve

What is A?
**A. vas deferens** B. ejaculatory duct C. testicular artery D. spermatic cord E. ilioinguinal nerve F. genitofemoral nerve
Identify A on this lateral view of the penis and testes
A. epididymis B. external spermatic fascia C. Buck's fascia D. tunica vaginalis E. pampiniform (venous) plexus

Identify A on this lateral view of the penis and testes
**A. epididymis** B. external spermatic fascia C. Buck's fascia D. tunica vaginalis E. pampiniform (venous) plexus
In this diagram of a growing placenta (~21 days), the large black arrow indicates the
- Extraembryonic mesoderm
- Stratum basalis of the endometrium
- Decidua basalis
- Syncytiotrophoblast
- Trophoblastic lacuna
- Cytotrophoblast shell

In this diagram of a growing placenta (~21 days), the large black arrow indicates the
- Extraembryonic mesoderm
- Stratum basalis of the endometrium
- Decidua basalis
- Syncytiotrophoblast
- Trophoblastic lacuna
* *6. Cytotrophoblast shell**
What type of cell is indicated in this growing placental villus?
- Simple cuboidal epithelial cell
- Syncytiotrophoblast
- Erythrocyte
- Mesenchymal cell
- Cytotrophoblast
- Decidual cell

What type of cell is indicated in this growing placental villus?
- Simple cuboidal epithelial cell
- Syncytiotrophoblast
- Erythrocyte
- Mesenchymal cell
* *5. Cytotrophoblast** - Decidual cell
Cytotrophoblast cells extend out of the villus to form branches in the
lacunae and also when invading into the endometrium. The
cytotrophoblast cells are stained brown in this preparation. If in contact
with maternal blood, the surface becomes covered by
syncytiotrophoblast.
Testis: What cell is indicated by the arrows?
- Spermatocyte
- Spermatid
(late) - Spermatid
(early) - Spermatogonia

Testis: What cell is indicated by the arrows?
1. Spermatocyte
2. Spermatid
(late)
3. Spermatid
(early)
4. Spermatogonia
Primary spermatocytes are cells with large nuclei fairly close to the
bottom of the seminiferous tubule but above the spermatogonia (which
have more condensed nuclei).
Identify A
A. rectovesical pouch B. seminal vesicles C. epididymis D. prostate gland E. Cowper's gland F. urethra

Identify A
A. rectovesical pouch **B. seminal vesicles** C. epididymis D. prostate gland E. Cowper's gland F. urethra
What is A?
- left testicular vein
- ureter
- left testicular artery
- inferior mesenteric artery
- inferior mesenteric vein

What is A? **1. left testicular vein** 2. ureter 3. left testicular artery 4. inferior mesenteric artery 5. inferior mesenteric vein
what is A?
- ureter
- ovarian artery
- ovarian vein
- inferior mesenteric artery
- renal artery

what is A?
- *1. ureter**
2. ovarian artery
3. ovarian vein
4. inferior mesenteric artery
5. renal artery
What is A?
- sphincter urethrae
- prostate gland
- internal urethral sphincter
- bulbosponiosus
- detruser muscle

What is A? **1. sphincter urethrae** 2. prostate gland 3. internal urethral sphincter 4. bulbosponiosus 5. detruser muscle
What is the structure labelled A?
External iliac artery Lateral sacral artery Superior gluteal artery Inferior gluteal artery Internal iliac artery

What is the structure labelled A?
External iliac artery Lateral sacral artery Superior gluteal artery **Inferior gluteal artery** Internal iliac artery
Other labelled structures (in this image): A → Superior gluteal artery B → External iliac artery C → Lateral sacral artery D → Inferior gluteal artery E → Internal iliac artery
Which of the following hormones is responsible for maintaining this morphology?
LH FSH Oestrogen Progesterone hCG
Which of the following hormones is responsible for maintaining this morphology?
LH FSH Oestrogen **Progesterone** hCG
At 28 weeks gestation where would you expect to feel the uterine fundus?
Xiphisternum
Umbilicus
Symphysis pubis
Halfway between xiphisternum and umbilicus
At 28 weeks gestation where would you expect to feel the uterine fundus?
Xiphisternum
Umbilicus
Symphysis pubis
Halfway between xiphisternum and umbilicus
At 12 weeks gestation where would you expect to feel the uterine fundus?
A
Xiphisternum
B
Umbilicus
C
Halfway between umbilicus and xiphisternum
D
Symphysis pubis
At 12 weeks gestation where would you expect to feel the uterine fundus?
A
Xiphisternum
B
Umbilicus
C
Halfway between umbilicus and xiphisternum
D
Symphysis pubis
Which of the following are recognised causes of intrauterine growth restriction (IUGR)?
Hypercholesterolaemia
Hypertension
Pre-eclampsia
Diabetes
Alcohol
Smoking
Which of the following are recognised causes of intrauterine growth restriction (IUGR)?
Hypercholesterolaemia
Hypertension
Pre-eclampsia
Diabetes
Alcohol
Smoking
Which of the following are accounts for 30-40% of intrauterine growth restriction (IUGR) cases?
Hypercholesterolaemia
Hypertension
Pre-eclampsia
Diabetes
Alcohol
Smoking
Which of the following are accounts for 30-40% of intrauterine growth restriction (IUGR) cases?
Hypercholesterolaemia
Hypertension
Pre-eclampsia
Diabetes
Alcohol
Smoking
Which of the following is thought to be a cause of hyperemesis gravidarum?
Over eating
Psychological issues
High levels of circulating HCG
Underlying infection
Which of the following is thought to be a cause of hyperemesis gravidarum?
Over eating
Psychological issues
High levels of circulating HCG
Underlying infection
Which of the following methods is the correct way to calculate the estimated date of delivery (EDD)?
Last day of LMP + 8 months and 1 week
First day of last menstrual period (LMP) + 8 months and 1 week
First day of LMP + 9 months
First day of LMP + 9 months and 1 week
Which of the following methods is the correct way to calculate the estimated date of delivery (EDD)?
Last day of LMP + 8 months and 1 week
First day of last menstrual period (LMP) + 8 months and 1 week
First day of LMP + 9 months
First day of LMP + 9 months and 1 week
Which period of gestation does the 2nd trimester represent?
A
14-29 weeks
B
15-30 weeks
C
10-20 weeks
D
13-28 weeks
Which period of gestation does the 2nd trimester represent?
A
14-29 weeks
B
15-30 weeks
C
10-20 weeks
D
13-28 weeks
What is the most common cause of postpartum haemorrhage?
Vulval or vaginal lacerations
Uterine atony
Uterine rupture
Retained placenta
What is the most common cause of postpartum haemorrhage?
Vulval or vaginal lacerations
Uterine atony
Uterine rupture
Retained placenta
Which causative agent most likely caused this pneumonia? [1]
Cytomegalovirus
Parainfluenza virus
Respiratory syncytial virus
Adenovirus

Which causative agent most likely caused this pneumonia? [1]
Cytomegalovirus
Parainfluenza virus
Respiratory syncytial virus - Multinucleated giant cells can be seen within the bronchial epithelium and neighboring alveoli.
Adenovirus
At 22 weeks gestation where would you expect to find the uterine fundus?
[1]
Umbilicus
A 40 year-old man presents to his GP with a new left testicular mass. Blood tests are requested which demonstrate raised LDH and alpha fetoprotein (AFP).
What type of testicular cancer can be excluded?
Seminoma
Embryonal
Teratoma
Trophoblastic
Yolk-sac
A 40 year-old man presents to his GP with a new left testicular mass. Blood tests are requested which demonstrate raised LDH and alpha fetoprotein (AFP).
What type of testicular cancer can be excluded?
Seminoma However, alpha fetoprotein is never produced with a seminoma.
Embryonal
Teratoma
Trophoblastic
Yolk-sac
A 22-year-old woman who is 9 weeks pregnant (G1P0) attends the gynaecological assessment unit with vaginal bleeding. A transvaginal ultrasound scan confirms an intrauterine pregnancy with a dilated cervical os and she is diagnosed with inevitable miscarriage. Following counselling about her options she declines expectant management and chooses to have her miscarriage managed medically.
Which of the following medications should she be given?
Vaginal misoprostol
Intramuscular (IM) methotrexate
Oral misoprostol
Intravenous (IV) magnesium sulphate
Oral mifepristone
A 22-year-old woman who is 9 weeks pregnant (G1P0) attends the gynaecological assessment unit with vaginal bleeding. A transvaginal ultrasound scan confirms an intrauterine pregnancy with a dilated cervical os and she is diagnosed with inevitable miscarriage. Following counselling about her options she declines expectant management and chooses to have her miscarriage managed medically.
Which of the following medications should she be given?
Vaginal misoprostol is the sole agent used in the UK for medical management of miscarriage. It is a prostaglandin analogue that binds to myometrial cells, causing contractions that lead to expulsion of tissue.
Intramuscular (IM) methotrexate
Oral misoprostol
Intravenous (IV) magnesium sulphate
Oral mifepristone
A 1-day-old baby is transferred to the neonatal intensive care unit (NICU) following the onset of grunting, fever, tachycardia, and episodes of apnoea. They are started on intravenous (IV) benzylpenicillin and gentamicin. They were born at term and were a normal birth weight. The mother tells you that she had a normal pregnancy and labour.
Which of the following is the most likely causative organism?
Staphylococcus epidermis
Listeria monocytogenes
Candida albicans
Escherichia coli
Streptococcus agalactiae
A 1-day-old baby is transferred to the neonatal intensive care unit (NICU) following the onset of grunting, fever, tachycardia, and episodes of apnoea. They are started on intravenous (IV) benzylpenicillin and gentamicin. They were born at term and were a normal birth weight. The mother tells you that she had a normal pregnancy and labour.
Which of the following is the most likely causative organism?
Staphylococcus epidermis
Listeria monocytogenes
Candida albicans
Escherichia coli
Streptococcus agalactiae This neonate is suffering from early-onset neonatal sepsis. The most common causative organism of this is Streptococcus agalactiae - also known as Group B Streptococcus (GBS).
Which of the following is the correct definition of fetal bradycardia according to NICE guidelines?
Baseline heart rate less than 80 bpm
Baseline heart rate less than 60 bpm
Baseline heart rate less than 110 bpm
Baseline heart rate less than 120 bpm
Which of the following is the correct definition of fetal bradycardia according to NICE guidelines?
Baseline heart rate less than 80 bpm
Baseline heart rate less than 60 bpm
Baseline heart rate less than 110 bpm
Baseline heart rate less than 120 bpm
Name a risk factor for germ cell tumours [1]
Cryptochordism
Endometrial cancer is caused by excess:
Progesterone
LH
FSH
Oestrogen
testosterone
Endometrial cancer is caused by excess:
Progesterone
LH
FSH
Oestrogen
testosterone
Leiomyomas are caused by an excess of:
Progesterone
LH
FSH
Oestrogen
testosterone
Leiomyomas are caused by an excess of:
Progesterone
LH
FSH
Oestrogen
testosterone
Which pathology is depicted in this histological slide? [1]

Hyaline membrane disease・Neonatal respiratory distress syndrome
What % and L of oxygen would you give a pregnany mother to decrease the chance of IGUR mortality? [1]
55% O2 at 8L/min round the clock decreases perinatal mortality rate
What position should mothers lie at during pregnancy if at risk of IUGR? [1]
Bed rest in left lateral position increases uteroplacental blood flow
Which nutritional things would you screen for in pre-term babies? [2]
Hyperglycemia (poorly developed pancreas; immature insulin secretion)
Osteopenia (limited Ca & P in parentral nutrition)
What type of virus caused this lung infection? [1]

RSV
. Multinucleated giant cell (MNGC) of respiratory syncytial virus infection
demonstrating a large intracytoplasmic inclusion (arrow); (H&E, 1000 ). MNGCs
are more commonly seen within alveoli than within bronchioles.
Which three viruses are most likely to cause this disease? [3]

Enterovirus 71 Virus
Coxsackie virus
Kawasaki virus
Which of the following is the most common cause for hand fott and mouth disease [1]
What is the causative agent of this CSF infection? [1]

Group B streptococcus
What is the most likely cause of this neonatal pathology? [1]

Osteogenesis imperfecta
A child presents to A&E and becomes siginifcantly unwell and dies. The biopsy reveals viral antigens.
What is the most likely cause of their death? [1]
A histological biopsy from their lung is shown below.

RSV - most likely cause of viral pneumonia in neonates
Which SIDS pathology is depicted in this histopathological slide? [1]

Persistent haemopoiesis in the liver
What is likely to be the cause of death from this infant? [1]

Unknown - lung petechiae are suggestive of SIDS
A 64-year-old lady with a BMI of 37 presents to you complaining of incontinence. She has previously had two children, both were delivered vaginally and the first required forceps due to slow progression of the second stage of labour. She takes no regular medication and has no other significant past medical history.
Given her risk factors, which type of urinary incontinence is she most likely to suffer from?
Overflow incontinence
Mixed inctontinence
Urge incontinence
Stress incontinence
A 64-year-old lady with a BMI of 37 presents to you complaining of incontinence. She has previously had two children, both were delivered vaginally and the first required forceps due to slow progression of the second stage of labour. She takes no regular medication and has no other significant past medical history.
Given her risk factors, which type of urinary incontinence is she most likely to suffer from?
Overflow incontinence
Mixed inctontinence
Urge incontinence
Stress incontinence - forceps delivery increase liklihhod of stress incont.
What is the most common type of breast cancer? [1]
Invasive ductal carcinoma

Desribe pathophysiology of invasive ductal carcinoma [1]
when BM breached and malignant cells try to create small ducts - get sheets of cells penetrating the SMC & stroma

Describe the pathology of invasive lobular carcinoma [1]
get sheets of cells penetrating the SMC & stroma
Malignant cells form single file lines or single cells
Often show vacuoles within cytoplasm

What is the structure highlighted? [1]
Describe the cells surrounding it [2]

Lactiferous Duct - each lobe is drained by a single lactiferous duct that opens into the nipple. It is lined by a double layer of cuboidal or columnar cells surrounded by a sheath of connective tissue with myoid cells.
Difference between lactating and non-lactating mammory glands histoligically
R: Lactating

What type of breast cancer is depicted? [1]

classic invasive lobular carcinoma
What type of breast cancer is depicted? [1]

ductal carcinoma in situ (DCIS)
What type of breast cancer is depicted? [1]

DCIS
What alteration to the breast tissue has occured? [1]

Figure 2 – Histology showing ductal carcinoma in-situ (DCIS), demonstrating the malignant cells confined to the mammary ducts
What type of pathology is depicted in this breast tissue?
Invasive ductal carcinoma
DCIS
Invasive lobular carnicoma

What type of pathology is depicted in this breast tissue?
Invasive ductal carcinoma
DCIS
Invasive lobular carnicoma
What type of pathology is depicted in this breast tissue?
Invasive ductal carcinoma
DCIS
Invasive lobular carnicoma

What type of pathology is depicted in this breast tissue?
Invasive ductal carcinoma
DCIS
Invasive lobular carnicoma
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia

Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia
Apocrine metaplasia with eosinophilic cytoplasm and apical snouts involving dilated cysts. Notice the transition from single to multiple layered epithelium to true papillary configuration in the same cystic space.
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia

Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia - abundant eosinophilic granular cytoplasm, prominent nucleolus and apocrine snouts.
What change to breast tissue is depicted here? [1]

Microcalcifications tend to be less common in fibrocystic change than in carcinoma. They tend to be coarse and irregular.
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia

Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia
Some of the larger cysts in fibrocystic change may have a bluish appearance from outside (blue-domed cysts). The cyst lining is flattened or absent in some cases. In the center of this image, cysts are lined by apocrine epithelium. Note the focus of adenosis above it.
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia

Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia
Sclerosing adenosis is a benign hyperplastic process that may be mistaken for carcinoma. The average age at presentation is about 30 yrs. The lesion retains is lobular configuration and is more cellular centrally.
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia

Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia
The proliferating tubules may be elongated and have attenuated lumens. There is preferential preservation of myoepithelial cells in the tubules and epithelial cells are less conspicuous. Some degree of lobular fibrosis is usually present.
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia

Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
The tubules and glands in a fibroadenoma are lined by cuboidal or low columnar epithelium with uniform nuclei and surrounded by a myoepithelial layer. The stroma is made up of loose connective tissue. If the stroma is hypercellular, the diagnosis of phyllodes tumor should be excluded.
Sclerosing adenosis
Apocrine metaplasia
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia
Which change to breast tissue is depicted here
Cysts
DCIS
Fibroadenoma
Sclerosing adenosis
Apocrine metaplasia
Higher magnification view of intracanalicular pattern in a fibroadenoma. The stromal connective tissue invaginates into the glandular epithelium and appears to be contained within it.
Which breast pathology is depicted here? [1]

Lobular carcinoma-in-situ (LCIS) is a non-palpable lesion which is usually an incidental finding in breasts removed for other reasons. It is multicentric in 70% of cases and bilateral in 30% to 40% of cases. The lobules are distended with uniform round or oval, medium sized cells. The nuclei are uniform and normochromatic. This image shows LCIS involving several lobules. A few uninvolved lobules can be seen on the right.
What is this breast pathology depicted? [1]

Ductal carcinoma in situ
The tumor cells with high nuclear grade nearly fill the lumen in this example of DCIS. The cytoplasmic borders are sharply demarcated.
What breast pathology is depicted here [1]

High power view of cribriform DCIS showing microcalcifications.
What breast pathology is depicted here? [1]

This case of high-grade invasive ductal carcinoma was composed mostly of solid areas, showed no evidence of tubule formation and was assigned score of 3 for tubule formation.
Which of the these photos is invasive ductal or invasive lobular breast cancer? [2]

L: invasive ductal carcinoma showed tubule formation
R: Invasive lobular carcinoma The tumor cells are arranged in slender linear strands one to two cells across
Which of the these photos is invasive ductal or invasive lobular breast cancer? [2]

R: invasive ductal carcinoma showed tubule formation
L: Invasive lobular carcinoma
Which pathogen causes “Pneumococcus”? [1]
Streptococcus pneumoniae
Which of the following is anaerobic?
Bacillus
Listeria
Clostridium
Corynebacterium
Which of the following is anaerobic?
Bacillus
Listeria
Clostridium
Corynebacterium
Corynebacterium, Listeria, Bacillus & Clostridium are all what type of bacteria? [1]
Gram positive bacillius
Name the two vaccinations for Streptococcus pneumoniae [2] and how many serotypes they protect agaisnt [2]
Pneumococcal polysaccharide vaccine (PPV): Penuomax - covers 23 serotypes
Pneumococcal conjugate vaccine (PCV): Prevenar protects against 13 serotypes
Which pathogen causes A? [1]

Corynebacterium dipetheria
Which pathogen cauese this symptom? [1]

Neisseria meningitidis - septic patient
What is the most common cause of lobal pneumonia?
Streptococcus pneumoniae
What is the most common organism responsible for infective endocarditis?
Streptococcus bovis
Staphylococcus epidermis
Staphylococcus aureus
Streptococcus viridans
What is the most common organism responsible for infective endocarditis?
Streptococcus bovis
Staphylococcus epidermis
Staphylococcus aureus
Streptococcus viridans
Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever

Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever
Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever

Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever
Which pathogens cause A & B? [2]

A: measles
B: scarlet fever
Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever

Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever
Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever

Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever Scarlet fever: white strawberry tongue (left) and red strawberry tongue (right)
What type of virus is enterovirus, Hep A & rotavirus?
Enveloped RNA
Envelopoed DNA
Non-enveloped RNA
Non-enveloped DNA
What type of virus is enterovirus, Hep A & rotavirus?
Enveloped RNA
Envelopoed DNA
Non-enveloped RNA
Non-enveloped DNA
What type of virus are Papillomavirus, Adenovirus & Parvovirus (ssDNA)
Enveloped RNA
Envelopoed DNA
Non-enveloped RNA
Non-enveloped DNA
What type of virus are Papillomavirus, Adenovirus & Parvovirus (ssDNA)
Enveloped RNA
Envelopoed DNA
Non-enveloped RNA
Non-enveloped DNA
Measles, mumps, rubella (MMR)
RSV, influenza, parainfluenza
SARS-CoV-2
Hepatitis C
HIV
Measles, mumps, rubella (MMR)
RSV, influenza, parainfluenza
SARS-CoV-2
Hepatitis C
HIV
Name this symptom [1]
What causative agent is most likely to have caused this infection?

Herpetic whitlow
Caused by HSV-1 (60% of cases, HSV-2 in 40%)
What causative agent is most likely to have caused this? [1]

Congenital CMV infection
Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
VZV
Measles
Scarlet Fever

Which pathogen is most likely to have caused this symptom?
Diphtheria
Mumps
VZV
Measles
Scarlet Fever
What is this infection? [1]
Name the two most likely causative agents? [1]

Impetigo
Agents: group A Streptococcus and Staphylococcus aureus.
Label the causative agents of A-C

A: VZV
B: Scarlet Fever
C: Measles
Name the most likely causative agent of this symptom [1]

Epstein-Barr Virus - causing infectious mononucleosis (glandular fever)
Name the most likely causative agent of this symptom [1]

Epstein-Barr Virus - causing infectious mononucleosis (glandular fever)
Describe this syndrome depicted [1]
Name two diseases that a patient might suffer from if they have this syndrome [2]

Madelung deformity [1]
Idiopathic short stature [1]
leri-weill dyschondrosteosi s [1]
Which pathology is associated with a molar pregnancy? [1]
Hyperemesis gravidarum [1]
What does this surgical treatment treat? [1]

Cervical incompetence (image is a transvaginal cerclage)
What is does the US show? [1]

Cervical incompetence
Listeria is a gram [] bacteria.
Listeria is [] shaped
Listeria is a gram positive bacteria.
Listeria is rod shaped

Listeria is a gram [] bacteria.
Listeria is [] shaped
Listeria is a gram positive bacteria.
Listeria is rod shaped

What does the US depict? [1]

placental abruption
Name this feature of late congential syphilis [1]

Clutton joints
A painless joint effusion in a child, usually in the knee, caused by inflammation of the synovial membranes due to congenital syphilis
Name this feature of late congenital syphilis [1]

Hutchinson teeth
is a sign of congenital syphilis, which occurs when a pregnant mother transmits syphilis to her child in utero or at birth. The condition is noticeable when a child’s permanent teeth come in. The incisors and molars take on a triangular or peglike appearance.
Name this feature of late congenital syphilis [1]

Saber shins
What is the arrow pointing to? [1]

velamentous insertion of umbilical cord into placenta
What is the pathology depicted here? [1]

velamentous insertion of umbilical cord into placenta

Name this early stage congenital syphilis symptom

Pemphigus syphiliticus.
Name this early stage congenital syphilis symptom

Pemphigus syphiliticus.
In cases where a mother has potentially come into contact with parvovirus B19, viral serology can be performed:
Parvovirus specific [] antibodies indicate recent infection
Parvovirus specific [] antibodies indicate past infection and therefore immunity.
In cases where a mother has potentially come into contact with parvovirus B19, viral serology can be performed:
Parvovirus specific IgM antibodies indicate recent infection
Parvovirus specific IgG antibodies indicate past infection and therefore immunity.
The main risk of fetal parvovirus infection is []
The main risk of fetal parvovirus infection is fetal hydrops – the abnormal accumulation of fluid in two or more fetal compartments.

There is a classic triad of features in congenital toxoplasmosis. What are they? [3]
There is a classic triad of features in congenital toxoplasmosis:
Intracranial calcification
Hydrocephalus
Chorioretinitis (inflammation of the choroid and retina in the eye)
What pathology is 4-6 x higher of occuring in childhood because of IUGR? [1]
Cerebral palsy
What does Intraventricular hemorrhage / periventricular leukomalacia look like on ultrasound? [1]
Honeycombed

Explain pathophysiology of necrotising enterocolitis [2]
How serious? [1]
Part of the bowel becomes necrotic due to bacterial invasion of ischaemic bowell wall:
Causes large amount of gas in bowel: can cause perforation of bowel: leads to peritonitis & sepsis
It is a life threatening emergency

Label A-D of this Doppler ultrasound of an artery [4]

A: Systole
B: Average
C: Diastole
D: Diastolic notch

Compare the flow between A & C of this doppler ultrasound.

A: showing normal flow
C: severely reduced flow with severe notch (see arrows).
How does the A-wave in a ductus venosus doppler ultrasound present in a normal and IUGR fetus? [2]
Normally ductus venosus shows positive A wave.
Reversal of the A wave may be seen in severe intrauterine growth restriction as well as in tricuspid regurgitation.

Explain subset of SIDS infants related to serum platelet anomolies
Subset of SIDS infants have elevated serum serotonin platelets carry >98% of 5HT in blood:
Causes constriction of damaged blood vessels and enhances platelet aggregation
Which causative agent most likely caused this pneumonia? [1]
Cytomegalovirus
Parainfluenza virus
Respiratory syncytial virus
Adenovirus

Which causative agent most likely caused this pneumonia? [1]
Cytomegalovirus
Parainfluenza virus
Respiratory syncytial virus - Multinucleated giant cells can be seen within the bronchial epithelium and neighboring alveoli.
Adenovirus
What type of virus caused this lung infection? [1]

RSV
. Multinucleated giant cell (MNGC) of respiratory syncytial virus infection
demonstrating a large intracytoplasmic inclusion (arrow); (H&E, 1000 ). MNGCs
are more commonly seen within alveoli than within bronchioles.
What is the most common bacterial [1] and viral [1] cause of pneumonia in neonates? [2]
Respiratory syncytial virus (RSV)
streptococcus pneumoniae
What is the causative agent of this CSF infection? [1]

Group B streptococcus
What is the most likely cause of this neonatal pathology? [1]

Osteogenesis imperfecta
A child presents to A&E and becomes siginifcantly unwell and dies. The biopsy reveals viral antigens.
What is the most likely cause of their death? [1]
A histological biopsy from their lung is shown below.

RSV - most likely cause of viral pneumonia in neonates
Which SIDS pathology is depicted in this histopathological slide? [1]

Persistent haemopoiesis in the liver
What is likely to be the cause of death from this infant? [1]

Unknown - lung petechiae are suggestive of SIDS
What should normal symphysio-fundal height correspond to? [1]
In a normally growing fetus, the SFH measurement in centimetres it taken as corresponding to the gestation in weeks
IUGR is associated with which congenital heart defect in neonates? [1]
Patent ductus ateriosus - causes hypoxia
Which gram +ve bactria is indicated in this slide? [1]

Streptococcus pneumoniae
A deficiency in which the following would predispose an individual to a pneuomococcal infection?
IgA
IgM
IgE
IgG
IgD
A deficiency in which the following would predispose an individual to a pneuomococcal infection?
IgA
IgM
IgE
IgG Hypogammaglobulinaemia
IgD
A 6-year-old child presents to your clinic unwell with a fever and sore throat. Upon further history taking you discover he has not had any vaccinations. On examination, there is a grey-white coloured membrane covering his tonsils.
What is the most likely diagnosis?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever
A 6-year-old child presents to your clinic unwell with a fever and sore throat. Upon further history taking you discover he has not had any vaccinations. On examination, there is a grey-white coloured membrane covering his tonsils.
What is the most likely diagnosis?
Diphtheria
Mumps
Rubella
Measles
Scarlet Fever
Whats the difference between gastroschisis & exomphalos? [2]

This is a photograph of the lower back of a one day old baby who is still in hospital. What is the most likely cause of this lesion?
- Child abuse
- Blood coagulation defect
- Meningicoccal septicaemia
- Strawberry haemangioma
- Mongolian blue spot

This is a photograph of the lower back of a one day old baby who is still in hospital. What is the most likely cause of this lesion?
- Child abuse
- Blood coagulation defect
- Meningicoccal septicaemia
- Strawberry haemangioma
5. Mongolian blue spot
Dermal melanocytosis is the name of a kind of birthmark that is flat, blue, or blue-gray. They appear at birth or in the first few weeks of life. Dermal melanocytosis was formerly called Mongolian blue spots
This centile chart shows the weight of a newborn baby plotted against gestation. The baby is
- extremely low birthweight
- small for gestational age
- normal birthweight
- low birthweight
- very low birthweight

This centile chart shows the weight of a newborn baby plotted against gestation. The baby is
- extremely low birthweight
- small for gestational age
- normal birthweight
4. low birthweight - very low birthweight
a. greater vestibular (Bartholin’s) gland
b. perineal body
c. Cowper’s gland
d. crus of clitoris
e. bulbospongiosus

a. greater vestibular (Bartholin’s) gland
b. perineal body
c. Cowper’s gland
d. crus of clitoris
e. bulbospongiosus
This photograph is of a new born with hydrocele. This occurs as a result of
a. patent processus vaginalis
b. cryptorchidism
c. androgen insufficiency
d. ectopic testes
e. patent ductus arteriosus

This photograph is of a new born with hydrocele. This occurs as a result of
a. patent processus vaginalis
b. cryptorchidism
c. androgen insufficiency
d. ectopic testes
e. patent ductus arteriosus
This girl had difficulty swallowing. The arrow indicates a/an
- inflamed palatine tonsil
- inflamed adenoid
- normal adenoid
- normal palatine tonsil
- inflamed uvula
- normal uvula
- inflamed appendix

This girl had difficulty swallowing. The arrow indicates a/an
1. inflamed palatine tonsil
2. inflamed adenoid
3. normal adenoid
4. normal palatine tonsil
5. inflamed uvula
6. normal uvula
7. inflamed appendix
What is structure Z?
a. yolk sac
b. polar body
c. extraembryonic mesoderm
d. amnion
e. chorionic villi

What is structure Z?
a. yolk sac
b. polar body
c. extraembryonic mesoderm
d. amnion
e. chorionic villi
This diagram is the anterior view of the cervix and uterus. The supports of the cervix indicated are
- cardinal ligaments
- levator ani muscle
- round ligaments
- ovarian ligaments

This diagram is the anterior view of the cervix and uterus. The supports of the cervix indicated are
1. cardinal ligaments
2. levator ani muscle
3. round ligaments
4. ovarian ligaments
A baby was born at 27/40. She was given three doses of surfactant and ventilated. On day 4, a chest x-ray showed ‘solid’ lungs. The photomicrograph shows
- hyaline membrane disease
- normal lung for this age
- pneumonia
- pneumothorax
- pneumopericardium
- intraventricular haemmorhage

A baby was born at 27/40. She was given three doses of surfactant and ventilated. On day 4, a chest x-ray showed ‘solid’ lungs. The photomicrograph shows
1. hyaline membrane disease
2. normal lung for this age
3. pneumonia
4. pneumothorax
5. pneumopericardium
6. intraventricular haemmorhage
This diagram shows the inguinal canal of a 3-week old baby. What abnormality is shown?
- Hydrocoele
- Complete inguinal hernia
- Ectopic testis
- Intra-abdominal testis
- Teratoma

This diagram shows the inguinal canal of a 3-week old baby. What abnormality is shown?
- Hydrocoele
2. Complete inguinal hernia - Ectopic testis
- Intra-abdominal testis
- Teratoma
A 2-year-old girl is vomiting, refuses to eat and has a fever. She has a non-blanching haemorhagic rash. She is up to date with all her vaccinations. Which infective agent is
most likely to be associated with her condition?
- Haemophilus influenza
- Herpes simplex virus
- Mycobacterium tuberculosis
- Neisseria meningitides
- Streptococcus pyogenes

A 2-year-old girl is vomiting, refuses to eat and has a fever. She has a non-blanching haemorhagic rash. She is up to date with all her vaccinations. Which infective agent is
most likely to be associated with her condition?
- Haemophilus influenza
- Herpes simplex virus
- Mycobacterium tuberculosis
4. Neisseria meningitides - Streptococcus pyogenes
The photo shows
- syringomyelia
- exomphalos
- Meckel-Gruber syndrome
- sirenomelia
- amniotic band disruption
- gastroschisis

The photo shows
- syringomyelia
2. exomphalos - Meckel-Gruber syndrome
- sirenomelia
- amniotic band disruption
- gastroschisis
The photo shows
- syringomyelia
- exomphalos
- Meckel-Gruber syndrome
- sirenomelia
- amniotic band disruption
- gastroschisis

The photo shows
- syringomyelia
- exomphalos
- Meckel-Gruber syndrome
- sirenomelia
- amniotic band disruption
6. gastroschisis
The photomicrograph shows
- normal prostate
- prostatic adenocarcinoma
- normal testis
- papillary serous tumour of the testis
- transitional cell carcinoma

The photomicrograph shows
1. normal prostate
2. prostatic adenocarcinoma
3. normal testis
4. papillary serous tumour of the testis
5. transitional cell carcinoma
A 24 year old man presented to his GP complaining of a lump in the right testis. The patient was referred to his local urology department and underwent a right orchidectomy. In
this histopathology specimen of the tissue, the arrow indicates
- seminomatous tumour cells
- non-seminomatous tumour cells
- lymphocytes
- papillary serous carcinoma
- Sertoli cell tumour cells

A 24 year old man presented to his GP complaining of a lump in the right testis. The patient was referred to his local urology department and underwent a right orchidectomy. In
this histopathology specimen of the tissue, the arrow indicates
1. seminomatous tumour cells
2. non-seminomatous tumour cells
3. lymphocytes
4. papillary serous carcinoma
5. Sertoli cell tumour cells
State each type of testicular cancer shown [3]

The large images show a general histology pattern of a seminoma (upper panel)
**undifferentiated embryonal carcinoma (middle panel) **
teratoma: a tumor displaying differentiation into various somatic tissues (bottom panel).
This ovarian tumour is a/an
- adenocarcinoma
- teratoma
- dysgerminoma
- granulosa cell tumour
- choriocarcinoma
- seminoma

This ovarian tumour is a/an
- adenocarcinoma
- teratoma
- dysgerminoma
- granulosa cell tumour
- choriocarcinoma
- seminoma
- Human papilloma virus
- Herpes simplex virus
- Tricomonas vaginalis
- Neisseria gonorrhoea
- Chlamydia trachomatis

1. Human papilloma virus
2. Herpes simplex virus
3. Tricomonas vaginalis
4. Neisseria gonorrhoea
5. Chlamydia trachomatis
A caudal epidural would
1. anaesthetise the lower pelvic viscera, but would leave the legs unaffected.
2. anaesthetise the lower pelvic viscera and the legs.
3. anaesthetise the pudendal nerve.
4. anaesthetise just the perineum and the lower quarter of the vagina.
5. anaesthetise the area below the waist

A caudal epidural would
1. anaesthetise the lower pelvic viscera, but would leave the legs unaffected.
2. anaesthetise the lower pelvic viscera and the legs.
3. anaesthetise the pudendal nerve.
4. anaesthetise just the perineum and the lower quarter of the vagina.
5. anaesthetise the area below the waist
A 3-year-old boy presents with a mass in his abdomen. There is no significant history. Physical examination findings include a firm, non-pulsatile abdominal mass in the left abdomen which does not cross the midline. Tenderness is elicited on deep palpation. A urine dipstick is positive for a trace amount of blood. Which of the following is the most appropriate management for this patient?
A. Chemotherapy alone
B. Nephrectomy alone
C. Nephrectomy followed by chemotherapy
D. Nephrectomy followed by radiotherapy
A 3-year-old boy presents with a mass in his abdomen. There is no significant history. Physical examination findings include a firm, non-pulsatile abdominal mass in the left abdomen which does not cross the midline. Tenderness is elicited on deep palpation. A urine dipstick is positive for a trace amount of blood. Which of the following is the most appropriate management for this patient?
A. Chemotherapy alone
B. Nephrectomy alone
C. Nephrectomy followed by chemotherapy
D. Nephrectomy followed by radiotherapy
Treatment of Wilms tumor is usually nephrectomy followed by systemic chemotherapy.
A 2-year-old male is brought by his mother with complaints of fever, hematuria, and a left abdominal mass. The child appears to be weak and lethargic. The biopsy of the mass is done, which reveals stroma with bone, cartilage, fat, smooth and striated muscle, and areas of necrosis. What chromosome carries this disease?
A. Chromosome 5
B. Chromosome 11
C. Chromosome 17
D. Chromosome 22
A 2-year-old male is brought by his mother with complaints of fever, hematuria, and a left abdominal mass. The child appears to be weak and lethargic. The biopsy of the mass is done, which reveals stroma with bone, cartilage, fat, smooth and striated muscle, and areas of necrosis. What chromosome carries this disease?
A. Chromosome 5
B. Chromosome 11 Wilms tumor suppressor gene and is found on chromosome 11.
C. Chromosome 17
D. Chromosome 22
Which cell types are effected in this pathology? [1]

Precursor cone cells
A 6-month-old boy is brought to the clinic by his parents for a whitish appearance of the right pupil and squinting of the right eye. Physical examination shows a clear lens with a mass lesion at the posterior segment in the right eye. Ultrasound of the right eye shows a mass with hyperechoic areas showing acoustic shadow. A mutation in which of the following chromosomes is most likely responsible for this patient’s condition?
A. X
B. 7
C. 9
D. 13
A 6-month-old boy is brought to the clinic by his parents for a whitish appearance of the right pupil and squinting of the right eye. Physical examination shows a clear lens with a mass lesion at the posterior segment in the right eye. Ultrasound of the right eye shows a mass with hyperechoic areas showing acoustic shadow. A mutation in which of the following chromosomes is most likely responsible for this patient’s condition?
A. X
B. 7
C. 9
D. 13
Which gene is predominately mutated to cause Wilms tumour in this process? [1]

WT-1
Which of the following are impacted by retinoblastoma?
A
B

Which of the following are impacted by retinoblastoma?
A - cone cells
B
Which of the following are impacted by retinoblastoma?
Top
Bottom

Which of the following are impacted by retinoblastoma?
Top
Bottom - cone
Retinoblastoma
MDM2 or MDM4 over-expression or amplification - leads to inactivation of which gene?
MDM2 or MDM4 over-expression or amplification - leads to inactivation of TP53
A 1-year-old male is brought to the clinic by his parents, who are concerned about his intermittent fever for the past month. He has had no cough, vomiting, or diarrhea. He was born healthy and is at the 60th percentile for both height and weight. Temperature is 37.5 C (99.5 F), blood pressure is 80/50 mmHg, pulse is 102 beats per minute, and respirations are 22breaths per minute. On examination, the patient is lethargic and pale. The left upper eyelid is drooping, and the left pupil is constricted. Only the right side of the face appears flushed when he cries. There is mild hepatomegaly. Muscle strength is normal. Magnetic resonance imaging (MRI) reveals a paravertebral cervical mass. Which of the following protooncogenes is the pathology related to?
A. N-myc
B. TGF-alpha
C. Bcl-2
D. c-KIT
A 1-year-old male is brought to the clinic by his parents, who are concerned about his intermittent fever for the past month. He has had no cough, vomiting, or diarrhea. He was born healthy and is at the 60th percentile for both height and weight. Temperature is 37.5 C (99.5 F), blood pressure is 80/50 mmHg, pulse is 102 beats per minute, and respirations are 22breaths per minute. On examination, the patient is lethargic and pale. The left upper eyelid is drooping, and the left pupil is constricted. Only the right side of the face appears flushed when he cries. There is mild hepatomegaly. Muscle strength is normal. Magnetic resonance imaging (MRI) reveals a paravertebral cervical mass. Which of the following protooncogenes is the pathology related to?
A. N-myc
B. TGF-alpha
C. Bcl-2
D. c-KIT
Neuroblastomas are the most common extracranial tumors of childhood in patients younger than two years of age
A 1-year-old male is brought to the clinic by his parents, who are concerned about his intermittent fever for the past month. He has had no cough, vomiting, or diarrhea. He was born healthy and is at the 60th percentile for both height and weight. Temperature is 37.5 C (99.5 F), blood pressure is 80/50 mmHg, pulse is 102 beats per minute, and respirations are 22breaths per minute. On examination, the patient is lethargic and pale. The left upper eyelid is drooping, and the left pupil is constricted. Only the right side of the face appears flushed when he cries. There is mild hepatomegaly. Muscle strength is normal. Magnetic resonance imaging (MRI) reveals a paravertebral cervical mass. Which of the following protooncogenes is the pathology related to?
A. N-myc
B. TGF-alpha
C. Bcl-2
D. c-KIT
A 1-year-old male is brought to the clinic by his parents, who are concerned about his intermittent fever for the past month. He has had no cough, vomiting, or diarrhea. He was born healthy and is at the 60th percentile for both height and weight. Temperature is 37.5 C (99.5 F), blood pressure is 80/50 mmHg, pulse is 102 beats per minute, and respirations are 22breaths per minute. On examination, the patient is lethargic and pale. The left upper eyelid is drooping, and the left pupil is constricted. Only the right side of the face appears flushed when he cries. There is mild hepatomegaly. Muscle strength is normal. Magnetic resonance imaging (MRI) reveals a paravertebral cervical mass. Which of the following protooncogenes is the pathology related to?
A. N-myc
B. TGF-alpha
C. Bcl-2
D. c-KIT
Neuroblastomas are the most common extracranial tumors of childhood in patients younger than two years of age
This symptom would suggest which paediatric cancer?
Neuroblastoma
Rb
Wilms tumour
ALL

This symptom would suggest which paediatric cancer?
Neuroblastoma
Rb
Wilms tumour
ALL
ALL
Pro-B (CD19+, CD10-) always have translocation of [] gene
Pre-B always have translocation of chromosomes [] & []
Pro-B (CD19+, CD10-) always have translocation of MLL gene
Pre-B always have translocation of chromosomes 12 & 22
A 4 year old boy is brought to the physician by his mother due to a 5 week history of lethargy, a progressively enlarging left sided neck mass and a 5 day onset of unexplainable bilateral diffuse lower leg petechial hemorrhage. On exam, the left posterior cervical lymph node is enlarged and nontender to palpation. A lymph node biopsy shows a predominance of interfollicular infiltrate containing numerous blast cells and focal necrosis. Immunohistochemistry is positive for PAX5, CD10 and TdT. Upon further workup, which of the following translocations would be associated with a good prognosis?
t(12;21)
t(14;18)
t(8;14)
t(9;22)

A 4 year old boy is brought to the physician by his mother due to a 5 week history of lethargy, a progressively enlarging left sided neck mass and a 5 day onset of unexplainable bilateral diffuse lower leg petechial hemorrhage. On exam, the left posterior cervical lymph node is enlarged and nontender to palpation. A lymph node biopsy shows a predominance of interfollicular infiltrate containing numerous blast cells and focal necrosis. Immunohistochemistry is positive for PAX5, CD10 and TdT. Upon further workup, which of the following translocations would be associated with a good prognosis?
t(12;21) - pre B ALL
t(14;18)
t(8;14)
t(9;22)
‘Strep throat’ is predominately caused by:
Group A Streptococcus (Streptococcus pyogenes)
Streptococcus bovis
Streptococcus mutans
Group B Streptococcus (Streptococcus agalactiae)
Streptococcus pneumoniae

‘Strep throat’ is predominately caused by:
Group A Streptococcus (Streptococcus pyogenes)
Streptococcus bovis
Streptococcus mutans
Group B Streptococcus (Streptococcus agalactiae)
Streptococcus pneumoniae
This symptom is caused by
Group A Streptococcus (Streptococcus pyogenes)
Streptococcus bovis
Streptococcus mutans
Group B Streptococcus (Streptococcus agalactiae)
Streptococcus pneumoniae

This symptom is caused by (impetigo)
Group A Streptococcus (Streptococcus pyogenes)
Streptococcus bovis
Streptococcus mutans
Group B Streptococcus (Streptococcus agalactiae)
Streptococcus pneumoniae
Which the following is most likely to colonize the female genital tract?
Group A Streptococcus (Streptococcus pyogenes)
Streptococcus bovis
Streptococcus mutans
Group B Streptococcus (Streptococcus agalactiae)
Streptococcus pneumoniae
Which the following is most likely to colonize the female genital tract?
Group A Streptococcus (Streptococcus pyogenes)
Streptococcus bovis
Streptococcus mutans
Group B Streptococcus (Streptococcus agalactiae)
Streptococcus pneumoniae
Which bacteria is group A strep? [1]
Streptococcus pyogenes
Which hormone triggers the change from A to B?
LH
Oestrogen
FSH
Progesterone

Which hormone triggers the change from A to B?
LH
Oestrogen
FSH
Progesterone
Which of the following is oestrogen produced in?
A
B
C
D
E

Which of the following is oestrogen produced in?
A
B - granulosa cells
C
D
E
Which hormone falling triggers the creation of atretic follicles?
LH
Oestrogen
FSH
Progesterone
Which hormone falling triggers the creation of atretic follicles?
LH
Oestrogen
FSH
Progesterone
Endometrial cancer is caused by excess of which hormone
LH
Oestrogen
FSH
Progesterone
Endometrial cancer is caused by excess of which hormone
LH
Oestrogen
FSH
Progesterone
The endometrial lesion in the image above is most likely associated with which of the following ovarian tumors?
Fibroma
Granulosa cell tumor
Immature teratoma
Sertoli-Leydig cell tumor
Yolk sac tumor

The endometrial lesion in the image above is most likely associated with which of the following ovarian tumors?
Fibroma
Granulosa cell tumor
Immature teratoma
Sertoli-Leydig cell tumor
Yolk sac tumor
What type of cancer is depicted in this histopathological slide?
Ovarian
Cervical
Endometrial
Vesical

What type of cancer is depicted in this histopathological slide?
Ovarian
Cervical
**Endometrial **
Vesical

A 28-year-old female, gravida 0, presents to a reproductive endocrinologist’s office desiring fertility. She was recently diagnosed with polycystic ovarian syndrome (PCOS) based on chronic anovulation, signs of hirsutism (facial hair), and an ultrasound that was significant for multiple follicles (>10mm) in each ovary. At her initial visit, her body mass index (BMI) was noted to be 38 kg/m2, and her heart rate was 120 beats per minute. All of her other vital signs were within normal limits. Her past medical history is significant for diabetes mellitus type 2 which is controlled with metformin 500 mg twice daily. She denies any past surgical history. Family history is significant for obesity, hypertension, and dyslipidemia in her mother and father, and PCOS in her older sister. Upon questioning, she received all childhood vaccinations, including the HPV series as a teenager. What type of cancer is she at the most significant risk for developing in her lifetime?
A. Ovarian
B. Cervical
C. Endometrial
D. Anal
A 28-year-old female, gravida 0, presents to a reproductive endocrinologist’s office desiring fertility. She was recently diagnosed with polycystic ovarian syndrome (PCOS) based on chronic anovulation, signs of hirsutism (facial hair), and an ultrasound that was significant for multiple follicles (>10mm) in each ovary. At her initial visit, her body mass index (BMI) was noted to be 38 kg/m2, and her heart rate was 120 beats per minute. All of her other vital signs were within normal limits. Her past medical history is significant for diabetes mellitus type 2 which is controlled with metformin 500 mg twice daily. She denies any past surgical history. Family history is significant for obesity, hypertension, and dyslipidemia in her mother and father, and PCOS in her older sister. Upon questioning, she received all childhood vaccinations, including the HPV series as a teenager. What type of cancer is she at the most significant risk for developing in her lifetime?
A. Ovarian
B. Cervical
C. Endometrial
D. Anal
A nulliparous 36-year-old woman presents for an annual wellness visit. She is sexually active and takes an oral contraceptive pill regularly. She does not smoke tobacco, drink alcohol, or use illicit drugs. Her body mass index (BMI) is 35 kg/m2. Which patient factor most increases her risk for developing ovarian cancer?
A. BMI of 35 kg/m2
B. Age
C. Oral contraceptive use
D. Sexual activity
A nulliparous 36-year-old woman presents for an annual wellness visit. She is sexually active and takes an oral contraceptive pill regularly. She does not smoke tobacco, drink alcohol, or use illicit drugs. Her body mass index (BMI) is 35 kg/m2. Which patient factor most increases her risk for developing ovarian cancer?
A. BMI of 35 kg/m2
B. Age
C. Oral contraceptive use
D. Sexual activity
Why does breastfeeding & pregnancy protect agaisnt ovarian cancer? [1]
Breastfeeding and pregnancy protect against ovarian cancer as it reduces ovulatory cycles.
Which genes increase the liklihood of ovarian cancer? [2]
RCA1 and BRCA2 gene mutations are likely causes of ovarian and breast cancer. 10 to 15% of ovarian cancers have a genetic predisposition listed as the main risk factor.
Why does taking oral contraceptive pills cause a protective effect for ovarian cancer? [1]
Suppresses ovulation
What is the most likely syndrome that this baby has?
A. Amniotic band syndrome
B. Angelman syndrome
C. Down syndrome
D.Edwards syndrome
E. Prader-Willi syndrome

What is the most likely syndrome that this baby has?
A. Amniotic band syndrome
B. Angelman syndrome
C. Down syndrome
D.Edwards syndrome
E. Prader-Willi syndrome
What structure is A pointing to in this photomicrograph of an ovary?
A Corpus albicans
B. Corpus luteum
C. Primordial follicle
D. Primary follicle
E. Oocyte

What structure is A pointing to in this photomicrograph of an ovary?
A Corpus albicans
B. Corpus luteum
C. Primordial follicle
D. Primary follicle
E. Oocyte
What is the blue arrow pointing at?
A. posterior vaginal fornix
B. broad ligament
C. rectouterine pouch (of Douglas)
D. rectovesical pouch
E. vesicouterine

What is the blue arrow pointing at?
A. posterior vaginal fornix
B. broad ligament
C. rectouterine pouch (of Douglas)
D. rectovesical pouch
E. vesicouterine
The arrow is pointing to what structure in the breast?
A Lactiferous sinus
B. Lactiferous duct
C. Areola
D. Smooth muscle cells
E. Suspensory ligament

The arrow is pointing to what structure in the breast?
A Lactiferous sinus
B. Lactiferous duct
C. Areola
D. Smooth muscle cells
E. Suspensory ligament
This diagram shows the changes that occur after fertilisation and before implantation.
Name structure (e).
A. zygote
B. morula
C.blastocyst
D. embryo
E. fetus
This diagram shows the changes that occur after fertilisation and before implantation.
Name structure (e).
A. zygote
B. morula
C.blastocyst
D. embryo
E. fetus
A baby who is described as small for gestational age is one whose weight at birth
falls below which centile for their gestational age?
A. 3rd centile
B. 15th centile
C. 10th centile
D. 5th centile
E. 20th centile
A baby who is described as small for gestational age is one whose weight at birth
falls below which centile for their gestational age?
A. 3rd centile
B. 15th centile
C. 10th centile
D. 5th centile
E. 20th centile
What structure is labelled A in this photomicrograph of seminiferous tubules?
A. Primary
spermatocytes
B. Secondary
spermatocytes
C. Spermatogonia
D. Spermatids
E. Spermatozoa

What structure is labelled A in this photomicrograph of seminiferous tubules?
A. Primary
spermatocytes
B. Secondary
spermatocytes
C. Spermatogonia
D. Spermatids
E. Spermatozoa
What cells do you see in this photomicrograph of a cervical smear?
A. Chondrocytes
B. Epithelial cells
C. Fibroblasts
D. Lymphocytes
E. Myocytes

What cells do you see in this photomicrograph of a cervical smear?
A. Chondrocytes
B. Epithelial cells
C. Fibroblasts
D. Lymphocytes
E. Myocytes
What hormone is responsible for stimulating uterine contractions, production of
placental prostaglandin
A. Gonadotrophin-releasing hormone
B. Luteinising hormone
C.Oxytocin
D. Prolactin
E. Progesterone
What hormone is responsible for stimulating uterine contractions, production of
placental prostaglandin
A. Gonadotrophin-releasing hormone
B. Luteinising hormone
C.Oxytocin
D. Prolactin
E. Progesterone
What is structure X?
A. Corpus luteum
B. Primary oocyte
C. Secondary oocyte
D.Graafian follicle
E. Corpus albicans

What is structure X?
A. Corpus luteum
B. Primary oocyte
C. Secondary oocyte
D.Graafian follicle
E. Corpus albicans
What is the most likely syndrome that images in this photograph suggest?
A. Amniotic band syndrome
B. Angelman syndrome
C. Down syndrome
D. Edwards syndrome
E. Prader- Willi syndrome

What is the most likely syndrome that images in this photograph suggest?
A. Amniotic band syndrome
B. Angelman syndrome
C. Down syndrome
D. Edwards syndrome
E. Prader- Willi syndrome
What is the congenital heart defect shown in this diagram?
A. Critical pulmonary stenosis
B. Coarctation of the aorta
C. Pulmonary valve atresia
D. Ventricular septal defect
E. Tetralogy of Fallot

What is the congenital heart defect shown in this diagram?
A. Critical pulmonary stenosis
B. Coarctation of the aorta
C. Pulmonary valve atresia
D. Ventricular septal defect
E. Tetralogy of Fallot
Identify this neural tube defect.
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

Identify this neural tube defect.
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly
Identify this neural tube defect.
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

Identify this neural tube defect.
A. Encephalocoele
**B. Meningocoele **
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

Identify this neural tube defect.
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

Identify this neural tube defect.
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly
In this photograph of a baby with meningococcus septicaemia what is the most likely
cause?
A. Haemophilus influenzae
B.Neisseria meningitidis
C. Pseudomonas sp.
D. Staphylococcus sp.
E. Streptococcus pneumoniae

In this photograph of a baby with meningococcus septicaemia what is the most likely
cause?
A. Haemophilus influenzae
B.Neisseria meningitidis
C. Pseudomonas sp.
D. Staphylococcus sp.
E. Streptococcus pneumoniae
The diagram shows a sagital section of an embryo at about day 16. Idnetify A
A. definative yolk sac
B. extraembryonic mesoderm
C. chorionic cavity
D. hypobalst 0%
E. amniotic cavity

The diagram shows a sagital section of an embryo at about day 16. Idnetify A
A. definative yolk sac
B. extraembryonic mesoderm
C. chorionic cavity
D. hypobalst 0%
E. amniotic cavity
What type of follicle is labelled A in this photomicrograph of an ovary?
A. Antral
B. Graafian
C. Primary
D. Primordial
E. Secondary
(Growing)

What type of follicle is labelled A in this photomicrograph of an ovary?
A. Antral
B. Graafian
C. Primary
**D. Primordial **
E. Secondary
(Growing)
What structure in this photomicrograph of the male reproductive system is labelled
A?
A. Ductus (vas) deferens
B. Epididymis
C. Penis
D. Prostate gland
E. Seminiferous tubules

A. Ductus (vas) deferens
B. Epididymis
C. Penis
D. Prostate gland
E. Seminiferous tubules
These graphs show hormonal changes throughout the menstrual cycle. In pregnancy,
which hormone maintains the corpus luteum and the production of hormone A until
the placenta produces hormone A.
A. Oestradiol
B. Human chorionic gonadotrophin
C. Progesterone
D. Insulin-like growth factor
E. Gonadotrophin-
releasing hormone

These graphs show hormonal changes throughout the menstrual cycle. In pregnancy,
which hormone maintains the corpus luteum and the production of hormone A until
the placenta produces hormone A.
A. Oestradiol
B. Human chorionic gonadotrophin
C. Progesterone
D. Insulin-like growth factor
E. Gonadotrophin-
releasing hormone
This picture shows brain calcification in an infant. What is the most likely condition?
A. Chronic renal failure
B. Toxoplasmosis
C. Congenital cytomegalovirus
D. Intracerebral haemorrhage
E. Cavernous angioma

A. Chronic renal failure
B. Toxoplasmosis
C. Congenital cytomegalovirus
D. Intracerebral haemorrhage
E. Cavernous angioma
From what cells of the ovary did this tumour originate?
A. Epithelial cells
B. Germ cells
C. Sex cord stromal cells
D. Smooth muscle cells
E. Mixture of A, B and C

From what cells of the ovary did this tumour originate?
A. Epithelial cells
B. Germ cells
C. Sex cord stromal cells
D. Smooth muscle cells
E. Mixture of A, B and C
This graph shows hormonal changes throughout pregnancy. Hormone C is measured
as part of the 1st and 2nd trimester screening tests for Down’s syndrome. What is
hormone C?
gonadotrophin-
releasing hormone
Insulin-like
growth factor
Progesterone
human
chorionic
gonadotrophin
Oestradiol

This graph shows hormonal changes throughout pregnancy. Hormone C is measured
as part of the 1st and 2nd trimester screening tests for Down’s syndrome. What is
hormone C?
gonadotrophin-
releasing hormone
Insulin-like
growth factor
Progesterone
human
chorionic
gonadotrophin
Oestradiol
On the diagram of the female perineum, identify A
A. Cowper’s
gland
B. perineal
body
C. crura of
clitoris
D.
Bartholin’s
gland
E. bulb of
vestibule
Name this collection of symptoms [1]

Madelung deformity
A 7-year-old presents with difficulty with left forearm movement. Examination demonstrates a prominent distal ulna and decreased pronation and supination of the left forearm. Dorsiflexion and ulnar deviation of the left wrist is decreased compared to the right wrist. The distal neurovascular exam is normal. A representative radiograph is shown. What is the most likely diagnosis?
A. Radial club hand
B. Madelung deformity
C. Radioulnar synostosis
D. Ulnar club hand
A 7-year-old presents with difficulty with left forearm movement. Examination demonstrates a prominent distal ulna and decreased pronation and supination of the left forearm. Dorsiflexion and ulnar deviation of the left wrist is decreased compared to the right wrist. The distal neurovascular exam is normal. A representative radiograph is shown. What is the most likely diagnosis?
A. Radial club hand
B. Madelung deformity
C. Radioulnar synostosis
D. Ulnar club hand
A 2-year-old boy is brought to the clinic by his mother. He has a history of familial short stature (both parents are short but otherwise healthy). During this visit, his pediatrician asks the nurse to measure the child’s height on a stadiometer in addition to the length on a measuring board. He also suggests height be measured henceforth during all clinic visits instead of the length. The nurse measures the average of 3 readings with the shoes removed and reports the height 1 cm lesser than the length. The child’s mother is perplexed. What is the best explanation that should be given to the child’s mother regarding this discrepancy?
A. This is a feature of constitutional delay of growth and puberty
B. This is a feature of combined familial short stature and constitutional delay of growth and puberty
C. This is a normal finding and no cause for alarm
D. This is a feature of disproportionate short stature
A 2-year-old boy is brought to the clinic by his mother. He has a history of familial short stature (both parents are short but otherwise healthy). During this visit, his pediatrician asks the nurse to measure the child’s height on a stadiometer in addition to the length on a measuring board. He also suggests height be measured henceforth during all clinic visits instead of the length. The nurse measures the average of 3 readings with the shoes removed and reports the height 1 cm lesser than the length. The child’s mother is perplexed. What is the best explanation that should be given to the child’s mother regarding this discrepancy?
A. This is a feature of constitutional delay of growth and puberty
B. This is a feature of combined familial short stature and constitutional delay of growth and puberty
C. This is a normal finding and no cause for alarm
D. This is a feature of disproportionate short stature
The height readings are lesser than the length by up to 1 cm. This is a physiological variation and there is no cause for alarm.
When the child stands the spine is compressed a bit compared to the lying down position and is the reason for the discrepancy.
A 15-year-old male is arrested after shooting the owner of a house he broke into with the intent to steal. The patient has been arrested for various other crimes, including trespassing, vandalism, and drug possession. On examination, he is irritable and unconcerned about his future. He does not show any remorse for shooting someone. What is the minimum duration of symptoms required to make the most likely diagnosis?
A. Three months
B. Six months
C. One year
D. Two years
A 15-year-old male is arrested after shooting the owner of a house he broke into with the intent to steal. The patient has been arrested for various other crimes, including trespassing, vandalism, and drug possession. On examination, he is irritable and unconcerned about his future. He does not show any remorse for shooting someone. What is the minimum duration of symptoms required to make the most likely diagnosis?
A. Three months
B. Six months
C. One year
The minimum duration of symptoms required for the diagnosis of conduct disorder is one year, with at least one of the symptoms present within the past six months.
D. Two years
Which type of attachment disorder matches these symptoms?

Reactive attchement disorder
Methylphenidate has been ordered for a 10-year-old male in the inpatient child and adolescent psychiatry unit for attention deficit-hyperactivity/disorder. Methylphenidate blocks the reuptake of which neurotransmitter?
A. Acetylcholine
B. Dopamine
C. Gamma-aminobutyric acid (GABA)
D. Serotonin
Methylphenidate has been ordered for a 10-year-old male in the inpatient child and adolescent psychiatry unit for attention deficit-hyperactivity/disorder. Methylphenidate blocks the reuptake of which neurotransmitter?
A. Acetylcholine
B. Dopamine
C. Gamma-aminobutyric acid (GABA)
D. Serotonin
Which type of attachment disorder matches these symptoms?

Disinhibited attachment disorder
Fibromyalgia is partly due to a fall in which of the following?
A. Acetylcholine
B. Dopamine
C. Gamma-aminobutyric acid (GABA)
D. Serotonin
Fibromyalgia is partly due to a fall in which of the following?
A. Acetylcholine
B. Dopamine
C. Gamma-aminobutyric acid (GABA)
D. Serotonin
Methlyphenidate treats which of the following
Anxiety
Conduct disorders
Depression
ADHD
Methlyphenidate treats which of the following
Anxiety
Conduct disorders
Depression
ADHD
Increased age causes a production of which pro-inflammatory molecule from macrophages?
CD14+
CD15+
CD16+
CD17+
Increased age causes a production of which pro-inflammatory molecule from macrophages?
CD14+
CD15+
CD16+
CD17+
With increased agaeing, dendritic cells pridce less of which interleukin?
IL-6
IL-8
IL-10
IL-12
IL-15

With increased agaeing, dendritic cells pridce less of which interleukin?
IL-6
IL-8
IL-10
IL-12
IL-15
Dendritic cells produce less of which toll like receptors (TLR) due to increased age? [2]
TLR 7 & 9
Natural killer cells have a preserved function of which of the following with age?
IFN-ϒ
TNF-a
TNF-b
IL-12
Natural killer cells have a preserved function of which of the following with age?
IFN-ϒ
TNF-a
TNF-b
IL-12
An 8-year-old female is brought to the clinic by her mother for an annual examination. The mother inquires as to when her daughter will likely begin puberty. Which of the following is the most notable and reliable first sign of puberty in girls?
A. Menarche
B. Thelarche
C. Pubarche
D. Linear growth
An 8-year-old female is brought to the clinic by her mother for an annual examination. The mother inquires as to when her daughter will likely begin puberty. Which of the following is the most notable and reliable first sign of puberty in girls?
A. Menarche
B. Thelarche - breast development
C. Pubarche
D. Linear growth
Which of the following statements correctly describes the apex of the bladder?
Internal triangular area with smooth walls
Connected to umbilicus by the median umbilical ligament
Where the bladder is continuous with the urethra
Triangular in shape and directed posteriorly
Which of the following statements correctly describes the apex of the bladder?
Internal triangular area with smooth walls
Connected to umbilicus by the median umbilical ligament
Where the bladder is continuous with the urethra
Triangular in shape and directed posteriorly
A 66-year-old woman is diagnosed with anal cancer. The tumour is located above the pectinate line.
This cancer is most likely to spread to which group of lymph nodes?
Superficial inguinal nodes
Internal iliac nodes
Para-aortic nodes
A 66-year-old woman is diagnosed with anal cancer. The tumour is located above the pectinate line.
This cancer is most likely to spread to which group of lymph nodes?
Superficial inguinal nodes
Internal iliac nodes
Para-aortic nodes
A woman in labour is due to undergo an episiotomy. Which of these is the most appropriate choice of anaesthetic for this procedure?
Spinal block
Caudal epidural
Pudendal nerve block
General anaesthetic
A woman in labour is due to undergo an episiotomy. Which of these is the most appropriate choice of anaesthetic for this procedure?
Spinal block
Caudal epidural
Pudendal nerve block
General anaesthetic
Which is the main muscle involved in helping to maintain erection? [1]
EXAM Q
Acceptable responses: bulbosongiosus, bulbospongiosus
Atherosclerosis of which artery is most likely to cause erectile dysfunction?
Superior gluteal artery
Inferior gluteal artery
Inferior rectal artery
Internal iliac artery
Perineal artery
Atherosclerosis of which artery is most likely to cause erectile dysfunction?
Superior gluteal artery
Inferior gluteal artery
Inferior rectal artery
Internal iliac artery
Perineal artery
The penile artery arises from the internal pudendal artery, which. arises from the internal iliac artery.
What is the cell lining of the majority of male urethra?
Transitional
Stratified squamous
Pseudostratified
Simple columnar
What is the cell lining of the majority of male urethra?
Transitional
Stratified squamous
Pseudostratified
Simple columnar
Which part of the testis changes during testicular cancer and how does it present?
Seminal vesicle
Prostate
Vas deferens
Epididymus
Seminiferous tubule
Which part of the testis changes during testicular cancer and how does it present?
Seminal vesicle
Prostate
Vas deferens
Epididymus
Seminiferous tubule: proliferating spermatogonia
The definition of antepartum haemorrhage is?
- significant bleeding from the
birth canal after the 24th week
of pregnancy - significant bleeding from the
birth canal after 32nd week of
pregnancy - significant bleeding from the
birth canal before the 24th
week of pregnancy
The definition of antepartum haemorrhage is?
1. significant bleeding from the
birth canal after the 24th week
of pregnancy
- significant bleeding from the
birth canal after 32nd week of
pregnancy - significant bleeding from the
birth canal before the 24th
week of pregnancy
Which of the following is not a pre-requisite for the
use of these obstetric instruments?
- The greatest diameter of the fetal
head must have passed the
pelvic brim - The cervix must be fully dilated
- The membranes must have
ruptured - The bladder must be empty
- The patient must have adequate
analgesia - The pregnancy must be 37+
weeks

Which of the following is not a pre-requisite for the
use of these obstetric instruments?
- The greatest diameter of the fetal
head must have passed the
pelvic brim - The cervix must be fully dilated
- The membranes must have
ruptured - The bladder must be empty
- The patient must have adequate
analgesia
6. The pregnancy must be 37+
weeks
Which of the following is not a risk factor for
intrauterine growth retardation?
- Pre-eclampsia
- Congenital
abnormalities - Infections
- Placental
insufficiency - First pregnancy
Which of the following is not a risk factor for
intrauterine growth retardation?
- Pre-eclampsia
- Congenital
abnormalities - Infections
- Placental
insufficiency
5. First pregnancy
Dizygotic twinning is more likely to occur…….
- in younger women
- as a result of fertility
treatments - parity <5
- by chance
Dizygotic twinning is more likely to occur…….
- in younger women
2. as a result of fertility
treatments - parity <5
- by chance
The puerperium is the period which……
- Begins with the
delivery of the baby
and ends 6 weeks later - Begins with the
delivery of the placenta
and ends 6 weeks later - Begins with the
delivery of the baby
and ends 6 months
later
The puerperium is the period which……
- Begins with the
delivery of the baby
and ends 6 weeks later
2. Begins with the
delivery of the placenta
and ends 6 weeks later - Begins with the
delivery of the baby
and ends 6 months
later
This is not a cause of recurrent
miscarriage………..
- autoimmune disease
- chromosomal
abnormalities - endometriosis
- cervical incompetence
- infection
- hormonal disturbances
This is not a cause of recurrent
miscarriage………..
- autoimmune disease
- chromosomal
abnormalities
3. endometriosis - cervical incompetence
- infection
- hormonal disturbances
Light & painless PV bleeding with a closed cervical os
& the uterus is size expected from dates is termed…..
- A threatened
miscarriage - A complete
miscarriage - A missed miscarriage
- Ongoing miscarriage
Light & painless PV bleeding with a closed cervical os
& the uterus is size expected from dates is termed…..
- A threatened
miscarriage - A complete
miscarriage - A missed miscarriage
- Ongoing miscarriage
What is the potential impact on the unborn
fetus of Toxoplasma gondii?
- Stillbirth
- Premature delivery
- physical damage,eg
eye disorders - Neurological disorders
leading to learning
difficulties - None of the above
- All of the above
6. All of the above
Administration of live vaccines (such as MMR) is often delayed until
after one year of age. Which of the following factors may interfere
with live vaccines in babies under 6 months of age?
- Lactoferrin in breastmilk
- Immunoglobulin G
acquired before birth - Neutrophil immaturity
- Absence of an adjuvant in
the vaccine - Immunological naivety
Administration of live vaccines (such as MMR) is often delayed until
after one year of age. Which of the following factors may interfere
with live vaccines in babies under 6 months of age?
- Lactoferrin in breastmilk
2. Immunoglobulin G
acquired before birth
- Neutrophil immaturity
- Absence of an adjuvant in
the vaccine - Immunological naivety
Which of the following factors are most important in
preventing collapse of aerated alveoli in the newborn baby?
- The first gasp
- Hepatic glycogen
- Pulmonary surfactant
- Closure of the ductus
arteriosus - Bradykinin
Which of the following factors are most important in
preventing collapse of aerated alveoli in the newborn baby?
- The first gasp
- Hepatic glycogen
3. Pulmonary surfactant
- Closure of the ductus
arteriosus - Bradykinin
The 5 components of the Apgar score are:
- Colour, respiratory
effort, muscle tone,
reflex irritability, heart
rate - Appearance, breathing
rate, grimace, pulse,
activity - complexion,
respiration, floppiness,
cry, pulse rate
The 5 components of the Apgar score are:
1. Colour, respiratory
effort, muscle tone,
reflex irritability, heart
rate
2. Appearance, breathing
rate, grimace, pulse,
activity
3. complexion,
respiration, floppiness,
cry, pulse rate
Common neonatal problems:
Which of the following is a cause of jaundice in the
first 24 hours of life?
- Hepatitis B
- Biliary atresia
- Physiological
jaundice - ABO immune
haemolysis - Breastmilk jaundice
4. ABO immune
haemolysis
Problems of prematurity: Respiratory Distress
Syndrome (RDS) is caused by:
- Lack of brown fat
- Surfactant deficiency
- Lack of alveolar
development - Pulmonary hypoplasia
- High surface area-to-
volume ratio
Problems of prematurity: Respiratory Distress
Syndrome (RDS) is caused by:
- Lack of brown fat
2. Surfactant deficiency - Lack of alveolar
development - Pulmonary hypoplasia
- High surface area-to-
volume ratio
This lesion, found on the lower
back of a newborn baby, arises from abnormal
development of which embryonic structure(s)?
- Frontonasal process
- Endoderm
- Angiogenic cells
- Yolk sac
- Neural folds

This lesion, found on the lower
back of a newborn baby, arises from abnormal
development of which embryonic structure(s)?
- Frontonasal process
- Endoderm
- Angiogenic cells
- Yolk sac
5. Neural folds
Congenital Heart Disease: Which of the
following is not a feature of Tetralogy of Fallot?
- Atrial septal defect
- Pulmonary stenosis
- Right ventricular
hypertrophy - Ventricular septal
defect - Over-riding aorta
Congenital Heart Disease: Which of the
following is not a feature of Tetralogy of Fallot?
1. Atrial septal defect
2. Pulmonary stenosis
3. Right ventricular
hypertrophy
4. Ventricular septal
defect
5. Over-riding aorta
Select the statement below which best describes
Low Birth Weight (LBW) babies
- All premature babies are LBW
- Conditions related to immaturity are
the leading cause of neonatal death
in the UK - 8% of births in Yemen are Low Birth
Weight - In the UK, LBW babies have the same
survival as normal birth weight
babies - If a baby is small-for-gestational age
they will also be LBW
- All premature babies are LBW
2. Conditions related to immaturity are
the leading cause of neonatal death
in the UK - 8% of births in Yemen are Low Birth
Weight - In the UK, LBW babies have the same
survival as normal birth weight
babies - If a baby is small-for-gestational age
they will also be LBW
Which congenital infection causes fetal anaemia,
heart failure and hydrops fetalis?
- Rubella
- Cytomegalovirus
- Toxoplasmosis
- Parvovirus B19
- Varicella
Which congenital infection causes fetal anaemia,
heart failure and hydrops fetalis?
- Rubella
- Cytomegalovirus
- Toxoplasmosis
4. Parvovirus B19 - Varicella
Genetic disease in childhood:
A polymorphic genetic marker is:
- Responsible for a number of
different inherited diseases - Gives rise to several
alternative phenotypes - Present at a frequency of >1%
in the normal population - A series of linked alleles
- A genetic tag that is unique to
a particular person
Genetic disease in childhood:
A polymorphic genetic marker is:
- Responsible for a number of
different inherited diseases - Gives rise to several
alternative phenotypes
Present at a frequency of >1%
in the normal population - A series of linked alleles
- A genetic tag that is unique to
a particular person
Developmental delay and disability: Which of the
following will be most helpful for a pre-school child
with uncomplicated learning disabilities?
- Physiotherapy
- Portage service
- Acute Paediatrician
- Intensive care unit
- The AA
Developmental delay and disability: Which of the
following will be most helpful for a pre-school child
with uncomplicated learning disabilities?
- Physiotherapy
2. Portage service - Acute Paediatrician
- Intensive care unit
- The AA
Which of the following statements about wheezing
in infancy is incorrect?
- It is mainly triggered by viral
infections - The wheeze occurs in the expiratory
phase of respiration - Most children with wheezing in
infancy will develop allergic asthma
in later life - Maternal smoking is a risk factor for
wheezing in infancy - The airways tend to narrow during
the expiratory phase of respiration
Which of the following statements about wheezing
in infancy is incorrect?
- It is mainly triggered by viral
infections - The wheeze occurs in the expiratory
phase of respiration
3. Most children with wheezing in
infancy will develop allergic asthma
in later life - Maternal smoking is a risk factor for
wheezing in infancy - The airways tend to narrow during
the expiratory phase of respiration
Child Psychiatry: which of the following
is a feature of autism?
- Impaired
communication - Bed wetting
- Criminal behaviour
- Hallucinations
- Truancy
Child Psychiatry: which of the following
is a feature of autism?
1. Impaired
communication
2. Bed wetting
3. Criminal behaviour
4. Hallucinations
5. Truancy
Childhood infections: This 4-year
old boy has a fever and a
vesicular rash. What is the most
likely cause?
- Smallpox
- Measles
- Meningococcal disease
- Tuberculosis
- Chickenpox

Childhood infections: This 4-year
old boy has a fever and a
vesicular rash. What is the most
likely cause?
- Smallpox
- Measles
- Meningococcal disease
- Tuberculosis
5. Chickenpox
Malignant disease in children: Which of the
following malignancies is not seen in childhood:
- Retinoblastoma
- Teratoma
- Wilm’s tumour
- Bronchial
carcinoma - Acute leukemia
Malignant disease in children: Which of the
following malignancies is not seen in childhood:
- Retinoblastoma
- Teratoma
- Wilm’s tumour
4. Bronchial
carcinoma - Acute leukemia
The majority of patients referred with short
stature have the following…..
- Constitutional
growth delay - Endocrine disorders
- Chronic diseases
- Psychosocial
deprivation - Dysmorphic
syndromes - Variation of normal
growth
The majority of patients referred with short
stature have the following…..
- Constitutional
growth delay - Endocrine disorders
- Chronic diseases
- Psychosocial
deprivation - Dysmorphic
syndromes
6. Variation of normal
growth
Red circle is
- pterion
- inion
- asterion
- nasion
- glabella

pterion
A indicates
- transition zone of the prostate gland
- peripheral zone of the prostate gland
- central zone of the prostate gland
- seminal vescicle
- bladder

A indicates
- transition zone of the prostate gland
2. peripheral zone of the prostate gland - central zone of the prostate gland
- seminal vescicle
- bladder
A baby was born at 27/40. She was given three doses doses of surfactant and ventilated.
On day 4, a chest x-ray showed ‘solid’ lungs. The photomicrograph shows
- hyaline membrane disease
- normal lung for this age
- pneumonia
- pneumothorax
- pneumopericardium
- intraventricular haemmorhage

1. hyaline membrane disease
Characteristics depicted suggest
- Kleinfelter syndrome
- Cushing syndrome
- Turner syndrome
- Acromegaly
- Congenital adrenal hyperplasia

Characteristics depicted suggest
1. Kleinfelter syndrome
2. Cushing syndrome
3. Turner syndrome
4. Acromegaly
5. Congenital adrenal hyperplasia
This diagram shows the inguinal canal of a 3-week old baby. What abnormality is shown?
- Hydrocoele
- Complete inguinal hernia
- Ectopic testis
- Intra-abdominal testis
- Teratoma

- Complete inguinal hernia
A 2-year-old girl is vomiting, refuses to eat and has a fever. She has a non-blanching haemorhagic rash. She is up to date with all her vaccinations. Which infective agent is
most likely to be associated with her condition?
- Haemophilus influenza
- Herpes simplex virus
- Mycobacterium tuberculosis
- Neisseria meningitides
- Streptococcus pyogenes
A 2-year-old girl is vomiting, refuses to eat and has a fever. She has a non-blanching haemorhagic rash. She is up to date with all her vaccinations. Which infective agent is
most likely to be associated with her condition?
- Haemophilus influenza
- Herpes simplex virus
- Mycobacterium tuberculosis
4. Neisseria meningitides - Streptococcus pyogenes
This is the nose of a newborn baby. This appearance is characteristic of:
- staphylococcal infection
- acne
- eczema
- milia
- erythema toxicum
- milia
The photo shows
- syringomyelia
- exomphalos
- Meckel-Gruber syndrome
- sirenomelia
- amniotic band disruption
- gastroschisis

The photo shows
- syringomyelia
2. exomphalos - Meckel-Gruber syndrome
- sirenomelia
- amniotic band disruption
- gastroschisis
A 24 year old man presented to his GP complaining of a lump in the right testis. The patient was referred to his local urology department and underwent a right orchidectomy. In
this histopathology specimen of the tissue, the arrow indicates
- seminomatous tumour cells
- non-seminomatous tumour cells
- lymphocytes
- papillary serous carcinoma
- Sertoli cell tumour cells

A 24 year old man presented to his GP complaining of a lump in the right testis. The patient was referred to his local urology department and underwent a right orchidectomy. In
this histopathology specimen of the tissue, the arrow indicates
1. seminomatous tumour cells
2. non-seminomatous tumour cells
3. lymphocytes
4. papillary serous carcinoma
5. Sertoli cell tumour cells
A represents
a. ischial tuberosity
b. ischial spine
c. ramus of ischium
d. pubic tubercle
e. pubis

A represents
a. ischial tuberosity
b. ischial spine
c. ramus of ischium
d. pubic tubercle
e. pubis
What is the most likely syndrome that this baby has?
A. Amniotic
band
syndrome
B. Angelman
syndrome
C. Down
syndrome
D. Edwards
syndrome
E. Prader-
Willi
syndrome

What is the most likely syndrome that this baby has?
A. Amniotic
band
syndrome
B. Angelman
syndrome
C. Down
syndrome
D. Edwards
syndrome
E. Prader-
Willi
syndrome
A. Corpus
albicans
B. Corpus
luteum
C. Primordial
follicle
D. Primary
follicle
E. Oocyte

A. Corpus
albicans
A. posterior
vaginal
fornix
B. broad
ligament
C.
rectouterine
pouch (of
Douglas)
D. rectovesical
pouch
E. vesicouterine

C.
rectouterine
pouch (of
Douglas)
Name structure (e).
A. zygote
B. morula
C. blastocyst
D. embryo
E. fetus

C. blastocyst
A. bladder
B. posterior fornix
C. vaginal canal
D. cervix
E. fundus ofuterus

A. bladder
B. posterior fornix
C. vaginal canal
D. cervix
E. fundus ofuterus
What structure is labelled A in this photomicrograph of seminiferous tubules?
A. Primary
spermatocytes
B. Secondary
spermatocytes
C. Spermatogonia
D. Spermatids
E. Spermatozoa

What structure is labelled A in this photomicrograph of seminiferous tubules?
A. Primary
spermatocytes
B. Secondary
spermatocytes
C. Spermatogonia
D. Spermatids
E. Spermatozoa
What hormone is responsible for stimulating uterine contractions, production of
placental prostaglandin and is missing in this diagram?
A. Gonadotrophin-releasing hormone
B. Luteinising hormone
C. Oxytocin
D. Prolactin
E. Progesterone

What hormone is responsible for stimulating uterine contractions, production of
placental prostaglandin and is missing in this diagram?
A. Gonadotrophin-releasing hormone
B. Luteinising hormone
C. Oxytocin
D. Prolactin
E. Progesterone
A. Corpus
luteum
B. Primary
oocyte
C. Secondary
oocyte
D.
Graafian
follicle
E. Corpus
albicans

A. Corpus
luteum
B. Primary
oocyte
C. Secondary
oocyte
D.
Graafian
follicle
E. Corpus
albicans
A. Amniotic
band
syndrome
B.
Angelman
syndrome
C. Down
syndrome
D. Edwards
syndrome
E. Prader-
Willi syndrome

A. Amniotic
band
syndrome
B.
Angelman
syndrome
C. Down
syndrome
D. Edwards
syndrome
E. Prader-
Willi syndrome
A. obturator internus
B. coccygeus
C. levator ani
D. piriformis
E. illiacus

A. obturator internus
B. coccygeus
C. levator ani
D. piriformis
E. illiacus
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly
A. definative yolk sac
B. extraembryonic mesoderm
C. chorionic cavity
D. hypobalst
E. amniotic cavity

A. definative yolk sac
B. extraembryonic mesoderm
C. chorionic cavity
D. hypobalst
E. amniotic cavity
These graphs show hormonal changes throughout the menstrual cycle. In pregnancy,
which hormone maintains the corpus luteum and the production of hormone A until
the placenta produces hormone A.
A. Oestradiol
B. Human chorionic gonadotrophin
C. Progesterone
D. Insulin-like growth factor
E. Gonadotrophin-releasing hormone

These graphs show hormonal changes throughout the menstrual cycle. In pregnancy,
which hormone maintains the corpus luteum and the production of hormone A until
the placenta produces hormone A.
A. Oestradiol
B. Human chorionic gonadotrophin
C. Progesterone
D. Insulin-like growth factor
E. Gonadotrophin-releasing hormone
This picture shows brain calcification in an infant. What is the most likely condition?
A. Chronic renal failure
B. Toxoplasmosis
C.Congenital cytomegalovirus
D. Intracerebral haemorrhage
E. Cavernous angioma

This picture shows brain calcification in an infant. What is the most likely condition?
A. Chronic renal failure
B. Toxoplasmosis
C.Congenital cytomegalovirus
D. Intracerebral haemorrhage
E. Cavernous angioma
This graph shows hormonal changes throughout pregnancy. Hormone C is measured
as part of the 1st and 2nd trimester screening tests for Down’s syndrome. What is
hormone C?
A. Oestradiol
B. Human chorionic gonadotrophin
C. Progesterone
D. Insulin-like growth factor
E. Gonadotrophin-releasing hormone

This graph shows hormonal changes throughout pregnancy. Hormone C is measured
as part of the 1st and 2nd trimester screening tests for Down’s syndrome. What is
hormone C?
A. Oestradiol
B. Human chorionic gonadotrophin
C. Progesterone
D. Insulin-like growth factor
E. Gonadotrophin-releasing hormone
This picture shows one of the major causes of death in a pre-term baby. What is this
condition?
Waterhouse-Friderichsen syndrome
Meningitis
Periventricular haemorrhage
Hyaline membrane disease
Neonatal sepsis

This picture shows one of the major causes of death in a pre-term baby. What is this
condition?
Waterhouse-Friderichsen syndrome
Meningitis
Periventricular haemorrhage
Hyaline membrane disease
Neonatal sepsis
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

E. Anencephaly
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly
A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly

A. Encephalocoele
B. Meningocoele
C. Spina bifida occulta
D. Myelomeningocoele
E. Anencephaly



BR; invasive ductal
BL: dcis
TR: invasive lobular
TL: insitu loblar
Which of the following best describes the slide
Stromal fibrosis
Cysts
Adenosis
Apocrine metaplasia

Cysts
(apocrine are more eosinophilic)

Which of the following best describes the slide
Stromal fibrosis
Cysts
Adenosis
Apocrine metaplasia

Apocrine metaplasia
Label the folllowing with
Stromal fibrosis
Cysts
Adenosis
Apocrine metaplasia


A 44-year-old woman who has just discovered that she is pregnant comes to see you about her hypertension. She reports that she has suffered from chronic hypertension for the past year and is currently taking ramipril. She does not suffer from any other medical problems. Her blood pressure today is 160/90mmHg. She would like your advice of hypertensive treatment in pregnancy.
Which one of the following should you advise?
Continue ramipril and start propranolol
Discontinue ramipril and start labetalol
Discontinue ramipril and start methyldopa
Continue ramipril
Continue ramipril and start labetalol
A 44-year-old woman who has just discovered that she is pregnant comes to see you about her hypertension. She reports that she has suffered from chronic hypertension for the past year and is currently taking ramipril. She does not suffer from any other medical problems. Her blood pressure today is 160/90mmHg. She would like your advice of hypertensive treatment in pregnancy.
Which one of the following should you advise?
Continue ramipril and start propranolol
Discontinue ramipril and start labetalol
Discontinue ramipril and start methyldopa
Continue ramipril
Continue ramipril and start labetalol
Tocolysis drugs:
which of the following is an inhibitor of prostaglandin synthesis?
nifedipine
atosiban
indomethacine
nitroglycerine NO donor
Betamimetics (sympathetic beta agonsists)
magnesium sulphate
Tocolysis drugs:
which of the following is an inhibitor of prostaglandin synthesis?
nifedipine
atosiban
indomethacine
nitroglycerine NO donor
Betamimetics (sympathetic beta agonsists)
magnesium sulphate
Tocolysis drugs:
which of the following is an oxytocin inhibitor?
nifedipine
atosiban
indomethacine
nitroglycerine NO donor
Betamimetics (sympathetic beta agonsists)
magnesium sulphate
Tocolysis drugs:
which of the following is an oxytocin inhibitor?
nifedipine
atosiban
indomethacine
nitroglycerine NO donor
Betamimetics (sympathetic beta agonsists)
magnesium sulphate
Tocolytic drugs:
which of the following is a myosin light chain inhibitor
nifedipine
atosiban
indomethacine
nitroglycerine NO donor
Betamimetics (sympathetic beta agonsists)
magnesium sulphate
Tocolytic drugs:
which of the following is a myosin light chain inhibitor
nifedipine
atosiban
indomethacine
nitroglycerine NO donor
Betamimetics (sympathetic beta agonsists)
magnesium sulphate
Which of the following is an SNRI?
fluoxetine
sertraline
citalopram
nortriptyline
duloxetine
Which of the following is an SNRI?
fluoxetine
sertraline
citalopram
nortriptyline
duloxetine
Which of the following is an TCA?
fluoxetine
sertraline
citalopram
nortriptyline
duloxetine
Which of the following is an TCA?
fluoxetine
sertraline
citalopram
nortriptyline
duloxetine
Which of the following has a possible risk of tachycardia and urinary retention in neonate and fetus?
fluoxetine
sertraline
citalopram
nortriptyline
duloxetine
Which of the following has a possible risk of tachycardia and urinary retention in neonate and fetus?
fluoxetine
sertraline
citalopram
nortriptyline
duloxetine
Which of the following is anti-cholinergic?
Oxybutynin
Tamsulosin
Prazosin
Bethanecol
Which of the following is anti-cholinergic?
Oxybutynin
Tamsulosin
Prazosin
Bethanecol
Which of the following is pro-cholinergic?
Oxybutynin
Tamsulosin
Prazosin
Bethanecol
Which of the following is pro-cholinergic?
Oxybutynin
Tamsulosin
Prazosin
Bethanecol
Which of the following are α-adrenergic antagonists?
Oxybutynin
Tamsulosin
Prazosin
Bethanecol
Which of the following are α-adrenergic antagonists?
Oxybutynin
Tamsulosin
Prazosin
Bethanecol
Which of the following drug induces labour by causing the myometrium to contract?
Oxytocin
Misoprostol
Carboprost
Mifepristone
Which of the following drug induces labour by causing the myometrium to contract?
Oxytocin
Misoprostol
Carboprost
Mifepristone
Which of the following drug induces labour by causing the cervix to contract?
Oxytocin
Misoprostol
Carboprost
Mifepristone
Which of the following drug induces labour by causing the cervix to contract?
Oxytocin
Misoprostol
Carboprost
Mifepristone
Which of the following drug induces labour by causing the uterus to contract?
Oxytocin
Misoprostol
Carboprost
Mifepristone
Which of the following drug induces labour by causing the uterus to contract?
Oxytocin
Misoprostol
Carboprost
Mifepristone
Which antibiotic inhibits bacterial wall synthesis, which prevents peptidoglycan cross linking?
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic inhibits bacterial wall synthesis, which prevents peptidoglycan cross linking?
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin (type of beta lactam drug)
Which antibiotic inhibits inhibit cell wall formation, D-ala bond formation & thus transglycosylation which prevents peptidoglycan cross linking to treat chlamydia
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic inhibits inhibit cell wall formation, D-ala bond formation & thus transglycosylation which prevents peptidoglycan cross linking to treat chlamydia
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic inhibits bacterial growth to treat chlamydia
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic inhibits bacterial growth to treat chlamydia
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic can be used to treat malaria?
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic can be used to treat malaria?
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic can be used to treat N. Gonnorrhoea
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
Which antibiotic can be used to treat N. Gonnorrhoea
Azithromycin
Doxycycline
Ceftriaxone
Benzylpenicillin
What role does alpha 1 action have on the IUS in the bladder? [1]
What effect do alpha 1 blockers have on IUS? [1]
It also induces contraction of the internal urethral sphincter of the urinary bladderInhibition causes it to relax and urine to escape
A 30 year old women is pregnant with her 3rd baby. She is now 31+2 weeks. She was concerned that the fetus seemed to have decreased movement and was referred for a umbilical cord and MCA Doppler. (she had an umbilical cord and MCA Doppler at the same stage of gestation for one of her previous pregnancies the normal umbilical cord Doppler is shown at the top). Her present umbilical cord Doppler is shown at the bottom.
What is the pattern shown in the present Doppler and what could be the consequence of this flow pattern? [2]

Absent flow throughout the diastole phase; blood is only flowing through systole
IUGR
A 30 year old women is pregnant with her 3rd baby. She is now 31+2 weeks. She was concerned that the fetus seemed to have decreased movement and was referred for a umbilical cord and MCA Doppler. (she had an umbilical cord and MCA Doppler at the same stage of gestation for one of her previous pregnancies the normal umbilical cord Doppler is shown at the top). Her present umbilical cord Doppler is shown at the bottom.
Explain the blood flow pattern seen in the normal ultrasound

At the end of the diastolic filling of the atria, there is still flow going through the umbilical cord; so there is still depth to it.
Flow never stops flowing all the way through even if the fetal heart stops beating !
A 30 year old women is pregnant with her 3rd baby. She is now 31+2 weeks. She was concerned that the fetus seemed to have decreased movement and was referred for a umbilical cord and MCA Doppler. (she had an umbilical cord and MCA Doppler at the same stage of gestation for one of her previous pregnancies the normal umbilical cord Doppler is shown at the top). Her present umbilical cord Doppler is shown at the bottom.
Explain why the pattern shown in the present Doppler is occurring [2]
(Absent flow in diastole) as blood is bein diverted to the MCA; vasoconstriction of the umbilical cord vessels is occuring
A 30 year old women is pregnant with her 3rd baby. She is now 31+2 weeks. She was concerned that the fetus seemed to have decreased movement and was referred for a umbilical cord and MCA Doppler. (she had an umbilical cord and MCA Doppler at the same stage of gestation for one of her previous pregnancies the normal MCA Doppler is shown at the top). Her present MCA is shown at the bottom.
What specific type of IUGR is shown here if you compare the umbilical cord and the MCA?
Explain how you can tell form the diagram

Asymmetric IUGR with brain sparing
There is no low point in the diastole phase in the MCA (due to vasodilation)
A baby is born by spontaneous vaginal delivery at 34 weeks to a mother who had tested positive for Covid-19. The baby boy weighed 2,065g. The neonate was admitted to the NICU, he was breathing room air without tachypnea and was started on feeds of expressed milk supplemented with formulae when breast milk was not available. 15 hrs after delivery they developed tachypnea and at 20 hrs they developed a fever, at 25 hrs they developed feed intolerance. An x-ray was taken at 30 hrs and repeated at 36 hrs. They tested positive for Covid-19 at 48 hrs after delivery.
What is the most likely diagnosis?

Necrotizing enterocolitis
Necrotising fasciitis in children may follow [] infection
Varicella-zoster infection
Herpes simplex virus
Cytomegalovirus
T. gondii
HIV
Necrotising fasciitis in children may follow [] infection
Varicella-zoster infection
Herpes simplex virus
Cytomegalovirus
T. gondii
HIV
Necrotising fasciitis in children may be caused by infection from which pathogen, aftern an initial infection from VZV? [1]
Group A streptococcus (GAS): e.g. Streptococcus pyogenes
This picture is from an autopsy. What is the pathology?
exomphalos
omphalocele
necrotising enterocolitis
peritonitits

This picture is from an autopsy. What is the pathology?
exomphalos
omphalocele
necrotising enterocolitis
peritonitits
An 8 year old child presents to her local A&E department with a 5 day history of progressively worsening fever, cough, nasal congestion and conjunctivitis. A rash started to appear on their face the day before. On examination of the oral mucosa small white spots are observed opposite the 1st and 2nd molars. Their vaccination status is unknown.
What is the most likely diagnosis?
Covid 19
Measles
Mumps
Rubella
Streptococcal scarlet fever

An 8 year old child presents to her local A&E department with a 5 day history of progressively worsening fever, cough, nasal congestion and conjunctivitis. A rash started to appear on their face the day before. On examination of the oral mucosa small white spots are observed opposite the 1st and 2nd molars. Their vaccination status is unknown.
What is the most likely diagnosis?
Covid 19
Measles
Mumps
Rubella
Streptococcal scarlet fever
An 7 year old boy is referred to an educational psychologist by the school because of concerns over their impaired communication development. During the assessment this behaviour is noted
What is the most likely diagnosis?
Attention deficit hyperactivity disorder
Autistic spectrum disorder
Conduct disorder
Obsessive compulsive disorder
Schizophrenia

Autistic spectrum disorder:
Not playing ‘pretend’ games (e.g. feeding a doll with play food)
Not smiling back when you smile at them
Not playing social games like ‘peek-a-boo’
Being over-sensitive or reacting strangely to some tastes, smells or sounds
Not pointing at interesting objects or looking when you point
Being very late starting to ‘babble’ and talk, not talking as much as other children or being able to say fewer than ten words at age 2 years old
Repetitive movements, for example rocking their body, flicking their fingers or hand-flapping
Repeating the same phrases over and over.
An individual is diagnosed with attention deficit hyperactivity disorder. When reviewing the mothers antenatal history what would be the most likely behaviour or condition that the mother had during her pregnancy?
Continued to drink alcohol
Continued to smoke
Had gestational diabetes
Had pre-eclampsia
Was obese
An individual is diagnosed with attention deficit hyperactivity disorder. When reviewing the mothers antenatal history what would be the most likely behaviour or condition that the mother had during her pregnancy?
Continued to drink alcohol
Continued to smoke
Had gestational diabetes
Had pre-eclampsia
Was obese
A female child was diagnosed with Turner syndrome at age of 4 years. She was given oxandrolone and her height was within target height. She was referred for further assessment at 7 year 10 months because of vaginal bleeding. On assessment she was assessed as Tanner stage 3.
How would this be best managed?
Counselling
Do nothing
Give GnRH analogues
Give growth hormone
Stop oxandrolone
A female child was diagnosed with Turner syndrome at age of 4 years. She was given oxandrolone and her height was within target height. She was referred for further assessment at 7 year 10 months because of vaginal bleeding. On assessment she was assessed as Tanner stage 3.
How would this be best managed?
Counselling
Do nothing
Give GnRH analogues - can’t do this because stage 3.
Give growth hormone
Stop oxandrolone
A baby is born at 36 weeks
Their length and weight are assessed at 8 weeks when they have their 1st set of vaccinations.
What is their gestationally corrected age?
40 weeks - 36 weeks = 4 weeks preterm
Start the plot at plotted at 4 week not 8 weeks
A 75 year old man has an open prostatectomy because of longstanding urinary problems that have not been managed by medication.
What is the most likely diagnosis?
Benign prostate hyperplasia
Embryonal carcinoma
Prostate cancer
Prostatis
Testicular cancer

A 75 year old man has an open prostatectomy because of longstanding urinary problems that have not been managed by medication.
What is the most likely diagnosis?
Benign prostate hyperplasia
Embryonal carcinoma
Prostate cancer
Prostatis
Testicular cancer
A 75 year old man has an open prostatectomy because of longstanding urinary problems that have not been managed by medication.
What is the most likely diagnosis?
Benign prostate hyperplasia
Embryonal carcinoma
Prostate cancer
Prostatis
Testicular cancer

A 75 year old man has an open prostatectomy because of longstanding urinary problems that have not been managed by medication.
What is the most likely diagnosis?
Benign prostate hyperplasia
Embryonal carcinoma
Prostate cancer
Prostatis
Testicular cancer
A 20 year old male goes to their GP concerned that their left testis / scrotum looks like a bag of worms. What anatomical issue means that the left side is predominately at risk?
There are no valves on the left side
The pampiniformplexus is more complex on the left
The left testicular vein is longer and drains to left renal vein at a right angle
The left testicular vein is shorter and drains into the IVC
Left renal has a longer course to reach the IVC

A 20 year old male goes to their GP concerned that their left testis / scrotum looks like a bag of worms. What anatomical issue means that the left side is predominately at risk?
There are no valves on the left side
The pampiniformplexus is more complex on the left
The left testicular vein is longer and drains to left renal vein at a right angle
The left testicular vein is shorter and drains into the IVC
Left renal has a longer course to reach the IVC
This 30 year old male has both a direct and indirect inguinal hernia. What structure is the yellow arrow pointing to?
Superficial ring
Deep ring
Hesselbach’s triangle
Linea alba
Aponeurosis of internal, external oblique and transversus abdominis muscles

This 30 year old male has both a direct and indirect inguinal hernia. What structure is the yellow arrow pointing to?
Superficial ring
Deep ring
Hesselbach’s triangle
Linea alba
Aponeurosis of internal, external oblique and transversus abdominis muscles
Which structure in this image helps you determine if a hernia is direct or indirect? [1]

Inferior epigastric vessels

Label A-C

A: Vas deferens
B: IEV
C: gonadal vessels
Is the hernia labelled at A a direct or indirect hernia?

Indirect
Which of the following is the vas deferens?
A
B
C
D
E

Which of the following is the vas deferens?
A
B
C
D
E
Which of the following is the inferior epigastric vessels?
A
B
C
D
E

Which of the following is the inferior epigastric vessels?
A
B
C
D
E
Which of the following is the gonadal vessels?
A
B
C
D
E

Which of the following is the gonodal vessels?
A
B
C
D
E
Is this a direct or indirect hernia?

Indirect
A 30 year old woman has a routine PAP smear and on investigation the pathologist notes these large glassy inclusions. What infectious pathogen is most likely to have caused these?
Chlamydiatrachomatis
Neisseriagonorrhoeae
Herpes simplex virus type I
Human papilloma virus type 16
Treponema pallidum

Chlamydiatrachomatis
Which of the following is leiomyoma, leiomyosarcoma and normal?

A: normal
B: fibroids
C: a malignant leiomyosarcoma is hypercellular and less fascicular, and consists of atypical smooth-muscle cells with hyperchromatic, enlarged nuclei. Increased mitotic figures and necrosis are frequent histological findings in leiomyosarcomas
A 30 year old woman has a routine PAP smear and on investigation the pathologist notes these abnormalities. What infectious pathogen is most likely to have caused these?
Chlamydiatrachomatis
Neisseriagonorrhoeae
Herpes simplex virus type I
Human papilloma virus type 16
Treponema pallidum

A 30 year old woman has a routine PAP smear and on investigation the pathologist notes these abnormalities. What infectious pathogen is most likely to have caused these?
Chlamydiatrachomatis
Neisseriagonorrhoeae
Herpes simplex virus type I
Human papilloma virus type 16
Treponema pallidum
A 30 year old woman has a routine PAP smear and on investigation the pathologist isolates the pathogen. What is the most likely pathogen? [1]

A 30 year old woman has a routine PAP smear and on investigation the pathologist isolates the pathogen. What is the most likely pathogen?
syphilis
During a routine ultrasound the image below was generated the largest depth of amniotic fluid was measured at 10 cm? What is this condition called?
Oligohydramnios
Normal amniotic volume
Polyhydramnios
During a routine ultrasound the image below was generated the largest depth of amniotic fluid was measured at 10 cm? What is this condition called?
Oligohydramnios
Normal amniotic volume
Polyhydramnios
A mother gives birth to a baby with chorioretintitis, hydrocephalus and intracranial atherosclerosis. A biopsy of the mothers muscle is shown below. What is the causative pathogen?
Toxoplasma gondii
Treponema pallidum
Parvovirus B19
Chlamydiatrachomatis
Neisseriagonorrhoeae

A mother gives birth to a baby with chorioretintitis, hydrocephalus and intracranial atherosclerosis. A biopsy of the mothers muscle is shown below. What is the causative pathogen?
Toxoplasma gondii
Treponema pallidum
Parvovirus B19
Chlamydiatrachomatis
Neisseriagonorrhoeae
A mother gives birth to a baby who lafter a couple of weeks looks like this. What is he infected with?
Toxoplasma gondii
Treponema pallidum
Parvovirus B19
Chlamydiatrachomatis
Neisseriagonorrhoeae

Parvovirus B19: slapped cheeks
At the routine 24 week antenatal visit the BP is measured at 142/92mmHg for the second time after the 1st reading was also 145/95mmHg 4 hrs previously. There is protein detected in her urine as well. What is the most likely diagnosis?
Gestational diabetes
Placental abruption
Placental praevia
Pre-eclampsia
Chronic hypertension of pregnancy
At the routine 24 week antenatal visit the BP is measured at 142/92mmHg for the second time after the 1st reading was also 145/95mmHg 4 hrs previously. There is protein detected in her urine as well. What is the most likely diagnosis?
Gestational diabetes
Placental abruption
Placental praevia
Pre-eclampsia
Chronic hypertension of pregnancy
At the routine 18 week antenatal visit the BP is measured at 142/92mmHg for the second time after the 1st reading was also 145/95mmHg 4 hrs previously. There is protein detected in her urine as well. What is the most likely diagnosis?
Gestational diabetes
Placental abruption
Placental praevia
Pre-eclampsia
Chronic hypertension of pregnancy
At the routine 18 week antenatal visit the BP is measured at 142/92mmHg for the second time after the 1st reading was also 145/95mmHg 4 hrs previously. There is protein detected in her urine as well. What is the most likely diagnosis?
Gestational diabetes
Placental abruption
Placental praevia
Pre-eclampsia
Chronic hypertension of pregnancy: up to week 20
An ultrasound is taken at 28 weeks showing the head (H) of the fetus is engaged with the internal os (white arrow). The red Doppler shows the umbilical vessels. What is the name of this issue?
Placenta previa
Placental abruption
Vasa previa
Placenta increta
Placenta accreta

Vasa previa - umbilical vessels connecting the placenta to the baby are covering the internal os
A 27 year old in her 3rd pregnancy is having a routine ultrasound which is shown below. The uterus is to the left hand side of the image and the bladder is at the bottom of the image. What is the problem shown?
Complete molar pregnancy
Incompetent cervix
Placental abruption
Placenta previa
Vasa praevia

Placenta previa: The US shows that the placenta is covering the OS opening completely
This is an ultrasound from a 16 week pregnant woman with heavy vaginal bleeding on examination the cervical os is dilated. The arrows are indicating the significant detachment of the placenta with hemorrahge. What is the type of miscarriage shown?
Complete
Incomplete
Inevitable
Missed
Threatened

Inevitable
The arrows are pointing to bleeding between the sac and the uterine wall. From the symptoms reported this would be inevitable miscarriage. The difference to a threatened miscarriage is that the cervical os is open compared to closed in a threatened
What is the aroow pointing at
urethra
vagina
rectum
ureter
anal canal

urethra
These images show a childhood respiratory condition. They show
congenital lobar emphysema
a bronchogenic cyst
asthma
pneumonia
tuberculosis

congenital lobar emphysema

Corpus luteum
what is the principal venous drainage of the anal cancl above the line indicated here?
superior rectal vein to internal iliac vein
middle rectal vein to inferior mesenteric vein
middle rectal ven to internal iliac vein
superior rectal vein to inferior mesenteric vein
inferior rectal vein to inferior mesenteric vein

superior rectal vein to inferior mesenteric vein
Which nerve loops around the ligament highlight here? [1]

pudendal nerve
The inguinal ligament runs from the ASIS to the pubic tubercle. What structure is located at its mid-point? [1]

femoral artery
The structure highlighted in this cross section of the prostate gland serves what function?
passage of ejaculant from seminal vesciles and vas deferens
entrance of prostatic fluid into urethra
vestigal / remnant uterus
prevent retrograde ejaculation
opening of bulbourethral glands

The structure highlighted in this cross section of the prostate gland serves what function?
passage of ejaculant from seminal vesciles and vas deferens
entrance of prostatic fluid into urethra
vestigal / remnant uterus
prevent retrograde ejaculation
opening of bulbourethral glands
A collection of striated muscle fibres are highlighted in this picture of the testes and spermatic cord. From which abdominal layer are these fibres derived?
external obliique
internal oblique
transversalis fascia
transversalis abdominus
parietal peritoneum

A collection of striated muscle fibres are highlighted in this picture of the testes and spermatic cord. From which abdominal layer are these fibres derived?
external obliique
internal oblique
transversalis fascia
transversalis abdominus
parietal peritoneum
The left testicular artery is hihglighted here. From where is this vessel derived
abdominal aorta T12
external iliac
internal iliac
abdominal aorta L2
pudendal artery

The left testicular artery is hihglighted here. From where is this vessel derived
abdominal aorta T12
external iliac
internal iliac
abdominal aorta L2
pudendal artery
what is A? [1]

obturator artery
What is A
iliacus
obturator internus
obturator externus
leavtor ani
coccygeus

What is A
iliacus
obturator internus
obturator externus
leavtor ani
coccygeus
A nine month old girl died after a sudden illness. Her adrenal gland is shown in her photograph. What most likekly caused her illness?
reye’s syndrome
meningoccocal septicaemia
neonate herpes virus infection
congenital adrenal hyperplasia

A nine month old girl died after a sudden illness. Her adrenal gland is shown in her photograph. What most likekly caused her illness?
reye’s syndrome
meningoccocal septicaemia
neonate herpes virus infection
congenital adrenal hyperplasia
The prostate gland has zones that are associated with higher prevalence of different conditions. Choose the option for the zone indicated by the arrow the condition most commonly associated with this zone
transitional zone - benign prostatc hyperplasia
peripheral zone - prostate cancer
transitional zone - prostate cancer
peripheral zone - benign prostatc hyperplasia

The prostate gland has zones that are associated with higher prevalence of different conditions. Choose the option for the zone indicated by the arrow the condition most commonly associated with this zone
transitional zone - benign prostatc hyperplasia
peripheral zone - prostate cancer
transitional zone - prostate cancer
peripheral zone - benign prostatc hyperplasia
The prostate gland has zones that are associated with higher prevalence of different conditions. Choose the option for the zone indicated by the arrow the condition most commonly associated with this zone
transitional zone - benign prostatc hyperplasia
peripheral zone - prostate cancer
transitional zone - prostate cancer
peripheral zone - benign prostatc hyperplasia

The prostate gland has zones that are associated with higher prevalence of different conditions. Choose the option for the zone indicated by the arrow the condition most commonly associated with this zone
transitional zone - benign prostatc hyperplasia
peripheral zone - prostate cancer
transitional zone - prostate cancer
peripheral zone - benign prostatc hyperplasia
adenocarcinoma of the prostate, Gleeson Grade 5
adenocarcinoma of the prostate, Gleeson Grade 1
transitional cell carcinoma
BPE
stratified squamous carcinoma

adenocarcinoma of the prostate, Gleeson Grade 5
dysgerminoma
serous adenocarcinoma
mucinous adenocarcnoma
teratoma
granulosa cell tumour

dysgerminoma
serous adenocarcinoma
mucinous adenocarcnoma
teratoma
granulosa cell tumour
leimyosarcoma
leimyoma
fibroadenoma
adenocarcinoma of the breast
normal breast tissue
fibrosarcoma

leimyosarcoma
leimyoma
fibroadenoma
adenocarcinoma of the breast
normal breast tissue
fibrosarcoma
This is a section from the breast. What does the image show?
Invasive carcinoma of no special type.
Benign breast terminal duct lobular unit
Ductal carcinoma-in-situ.
Lobular carcinoma-in-situ.

This is a section from the breast. What does the image show?
Benign breast terminal duct lobular unit
