What is the definition of an anaesthetic drug?
A drug that induces partial or total loss of sensation
What are the 2 main types of anaesthesia?
General anaesthesia:
- this involves total loss of sensation
Local anaesthesia:
- this involves partial loss of sensation
What are the 3 different types of local anaesthesia?
Regional anaesthesia:
- involves the loss of sensation to a region or part of the body
Local infiltration:
- Involves infiltration into cuts or skin incisions
- it is more confined to the area around the wound
Topical anaesthesia:
- this involves eye drops or topical skin creams
- it does NOT involve a needle
What are the 2 different methods of local anaesthesia?
Non-pharmacological:
- cold
- pressure
- hypoxia
Pharmacological:
- reversible - local anaesthetics
- irreversible - phenol, ethanol, radiofrequency, surgery
- involves complete destruction of the nerve carrying sensation from an area to the brain
What are the fundamental characteristics of a local anaesthetic agent?
It is a drug which:
- Reversibly prevents transmission of a nerve impulse
- In the region to which it is applied
- Without affecting consciousness
What are the different ways in which local anaesthetics can be administered?
- Can be applied topically - e.g. eye drops, on mouth ulcers or skin
- local infiltration around the skin edges of a wound
- nerve block
- epidural or spinal block
Which 2 major systems are affected in local anaesthetic toxicity?
What symptoms may result?
If you give someone too much local anaesthetic, it will work on the brain and the specialised conduction system within the heart
this results in neurological and cardiovascular symptoms
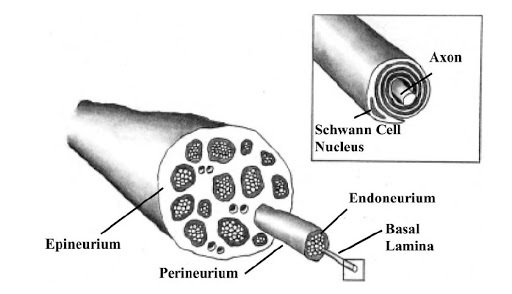
What are the 3 layers of a nerve?
Where does the local anaesthetic work?
The nerve is surrounded by the epineurium
Individual nerve bundles are surrounded by the perineurium
An individual nerve fibre is surrounded by the endoneurium
the LA is injected into the epineurium and takes time to diffuse into the nerve fibre
Why are local anaesthetics sometimes called “blocks”?
What is their general mechanism of action?
They block voltage gated sodium channels along the axon
this means that action potentials cannot be generated and passed on
they work on different domains of the sodium channel and prevent Na+ ions from moving into the cell
What are the characteristics of an ideal local anaesthetic?
- Reversible
- quick onset
- suitable duration
- no local irritation on repeated application
- no side effects
- no potential to induce allergy
- applicable by all routes
- cheap, stable and soluble
From which aspect do local anaesthetics block sodium channels?
What type of block does this provide?
LAs work by blocking sodium channel conduction
they block sodium channels from the inside
they provide reversible conduction block
What are the main local anaesthetic agents?
- Procaine
- Lidocaine
- Prilocaine
- Mepivacaine
- Bupivacaine
- Levo bupivacaine
- Ropivacaine
- Articaine
What is the structure of a local anaesthetic like?
All LAs have 2 components connected with an intermediate chain
they have a lipophilic part - an unsaturated benzene ring
and a hydrophilic part - tertiary amine
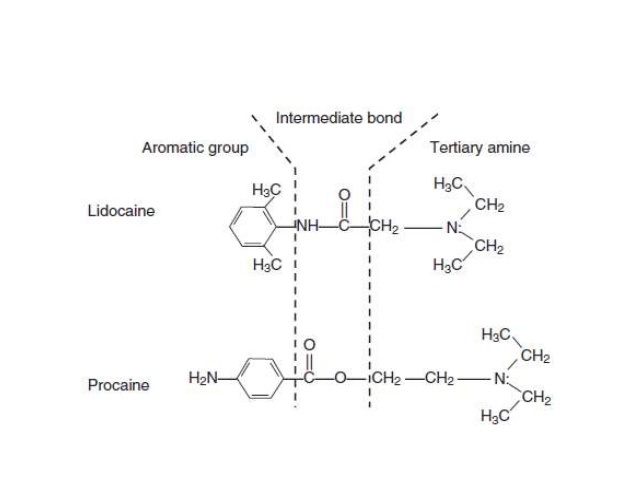
What structural component determines which type of local anaesthetic it is?
The link between the intermediate chain and the benzene ring determines the type of LA
it is either ester or amide
What do the names of all LAs end in?
How can you tell if they are ester or amide?
“Caine”
If there is an i before the Caine, they are amides
if there is NOT an i before the Caine, they are esters
What are examples of ester local anaesthetics?
- Benzocaine
- chloroprocaine
- cocaine
- procaine
- tetracaine
What are examples of amide local anaesthetics?
- Bupivacaine
- etidocaine
- levobupivacaine
- lidocaine
- mepivacaine
- prilocaine
- ropivacaine
What characteristic of local anaesthetics determines their onset of action?
The pKa value
LAs can exist in the ionised or unionised form
in order to get into the cell, they have to be in the unionised form
once they are within the cell, they have to become ionised in order to bind to the channel
What does the pKa value of a local anaesthetic tell you?
The pKa value shows that ionised and non-ionised forms of local anaesthetics are equal
if pKa > pH then unionised form > ionised form
if pKa < pH then ionised form > unionised form
What would the ratio be like if one local anaesthetic had a pKa of 10 and another had a pKa of 7?
The LA with a pKa value of 7 will have more unionised form and will work quicker
body pH is 7.4
the closer the pKa value of the local anaesthetic to 7.4, the faster it will work
What happens if body pH is lowered?
What does this mean about where local anaesthetic can be injected?
If the pH is lowered, there will be even less unionised form of LA and there is a greater difference between pH and pKa
if you inject LA around an abscess or inflamed tissue, it will not work due to local acidosis and lowered pH
What are the rules around ionised and non-ionised forms of local anaesthetic?
- Clinical onset is not the same for all local anaesthetics with the same pKa
- this may be due to the individual LAs ability to diffuse through connective tissue
- the closer the pKa to physiological pH, the faster the onset
What characteristic determines the duration of action of a local anaesthetic?
Protein binding
the more protein binding, the longer the duration of action
the drug is released from the protein over a longer period of time
the length of the intermediate chain joining aromatic and amide groups also has an influence
What is meant by potency?
What does it depend on?
The dose required to produce the desired effect
this depends on lipid solubility
a more lipid soluble drug will penetrate the cell membrane, meaning a smaller amount is required to produce a given effect
-
Arthritis58
-
A1 - Pectoral Girdle & Shoulder102
-
A2 - Upper Arm & Elbow94
-
Peripheral Nerve Lesions - Brachial Plexus Injuries34
-
Upper Limb Ultrasound17
-
A3 - Forearm92
-
A4 - Wrist & Hand82
-
L1 - Anatomy of the Vertebral Column94
-
Back Pain51
-
Hip Fracture43
-
L2 - Pelvis & Hip Joint76
-
Gluteal Region & Hip58
-
The Knee Joint72
-
The Thigh & Knee Anatomy68
-
Posterior Thigh & Knee74
-
Leg & Ankle58
-
Vessels of the Lower Limb49
-
The Leg & Ankle Anatomy74
-
The Foot60
-
Lower Limb Radiology36
-
LL Ultrasound and Cases25
-
Lower Limb Muscles100
-
Muscles of the Upper Limb69
-
SDL 1 - FRONT OF NECK67
-
Introduction to the Brain41
-
The Skull22
-
Blood Supply to Brain & Meninges74
-
SDL 2 - Face & Skull89
-
SDL 3 - Brain, Meninges & Blood Supply44
-
Front of Neck Surface Anatomy10
-
Brainstem & Cerebellum65
-
SDL 4 - Brainstem, Cerebellum & Cranial Nerves65
-
Cranial Nerves67
-
Forebrain & Ventricles56
-
Localisation60
-
SDL 5 - FOREBRAIN, VENTRICLES & CSF39
-
Local Anaesthetics43
-
Spinal Cord & Spinal Nerves66
-
Ascending Pathways68
-
Descending Motor Pathways53
-
Transient Ischaemic Attack (TIA)35
-
Stroke37
-
SDL - Vertebral Column & Spinal Cord70
-
SDL 7 - SPINAL CORD & SPINAL NERVES18
-
Parkinson’s Disease58
-
Basal Ganglia55
-
Somatosensory Physiology57
-
Patterns of Sensory Loss40
-
Skin Histology45
-
Epilepsy75
-
Headache - Diagnosis & Management72
-
Radiotherapy & Chemotherapy for CNS Tumours66
-
Dementia84
-
Multiple Sclerosis43
-
Pain 152
-
Clinical Aspects of Pain75
-
General Anaesthesia77
-
The Auditory Pathway48
-
The Visual Pathway55
-
Visual Defects72
-
Cerebellum50
-
The Auditory System78
-
Physiology of Vision54
-
Limbic System49
-
Balance, Posture & Vestibular System0
-
Upper & Lower Motor Neurone Disorders27
-
Gait and Posture41
-
Pharmacology of Movement37
-
Diagnosing Weakness23
