Cardio - Physiology - Hemodynamics; Local Vascular Control; Blood Pressure Control; Cardiac Output & Venous Return Flashcards
What is fluid velocity?
The speed of a particle of fluid (cm/sec)
What is fluid flow?
The amount of fluid traveling a distance per time
Q = velocity * area
If the cross sectional area (A) of an artery increases, what effect does this have on flow rate?
If the cross sectional area (A) of an artery increases, what effect does this have on velocity?
The flow rate will remain the same BECAUSE
–>
the velocity decreases
Q = vA
What two factors affect flow rate in the cardiovascular system?
Fluid velocity and vessel cross-sectional area
Q = vA
What are the two types of flow found in the cardiovascular system?
Turbulent (rough, damaging) and laminar (smooth, protective)

In simple terms, describe the effects of turbulent and laminar flows on cardiovascular vessels.
Laminar = efficient, protective
Turbulent = damaging, chaotic

In laminar flow through the arteries, where does the fluid flow quickest?
The central layers
(the outer layers interact with the sationary walls)

What does a high Reynold’s number (> 2000) indicate about the flow in the blood vessels?
What does a low Reynold’s number (< 2000) indicate about the flow in the blood vessels?
It is turbulent and noisy;
it is laminar and smooth

What three factors increase the Reynold’s number as they increase?
What factor decreases the Reynold’s number as it increases?
(Note: An increasing Reynold’s number = increasing blood turbulence)
Blood density,
*diameter of the blood vessel,
*blood velocity;
blood viscosity
(*vessel diameter and blood velocity are the two most important factors here)

Assuming flow rate has to remain constant, which will have a bigger effect on blood turbulence, changes in vessel diameter or changes in blood velocity?
Velocity
(diameter follows a linear change;
velocity will respond in a squared change)
v = Q / (πr2)
Is velocity higher in a narrow or wide vessel lumen?
Narrow
v = Q / (πr2)
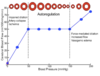
What term refers to the ability of a blood vessel to return to its normal, non-distended shape once an external force is removed?
What term refers to the ability of a blood vessel to deform (change shape) in response to a force?
What term refers to the ability of a blood vessel to change its volume in accordance with changes in internal pressure?
Elasticity;
distensibility;
compliance
Why are blood vessels in the elderly stiffer than those in younger populations?
Loss of elastin
(less elasticity)

Why are both blood vessel distensibility and elastance desirable?
The aorta (and other large vessels) distend with the increase in systolic pressure (this dampens pressures and decreases afterload).
The elastance means they (contracting) help distribute the fluid out into the capillaries continuously.
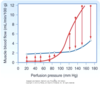
What controls the rate of blood flow?
I.e. what does the heart push against?
Peripheral resistance
Q = ΔP / R
Q = ΔP / R shows us that blood flow is impeded by resistance.
What equation shows us all the variables creating that resistance?
R = 8 * η * l / πr4
(8 * viscosity * length / πr4)
Changes in blood vessel diameter will have a bigger effect on which, blood velocity or the resistance to flow?
velocity = Q / πr2
Resistance to flow = 8ηl / πr4
50% narrowing of an artery will have what effect on the resistance in that artery?
A 16-fold increase
R = 8 * η * l / πr4
25% narrowing of an artery will have what effect on the resistance in that artery?
A 3.2-fold increase
R = 8 * η * l / πr4
Resistors in sequence are calculated as:
Resistors in parallel are calculated as:
R1 + R2 + R3 = RTotal
1/R1 + 1/R2 + 1/R3 = 1/RTotal
What effect does bifurcation of vessels off the aorta have on blood flow?
The resistance of all the vessels are now in parallel (and so, decreased);
this trades efficacy for function and reduced resistance –>
flow rates can now be different for different organs

Bifurcating the aorta into various blood vessels creates a system of reduced resistances (the resistance vessels are now in parallel).
What are the two major effects of this structure?
Differing blood flow through differing organs;
the heart pushes against less resistance
Increases in what two factors increase resistance to blood flow?
Increases in what single factor decrease resistance to blood flow?
Blood viscosity, vessel length
vessel lumen radius
R = 8 * η * l / πr4
An individual with diabetes can have an increased risk of a first heart attack high enough to be comparable to what other patient?
An individual that has already had a heart attack