Renal Pathology Flashcards
What is the most common cause of tubulointerstitial nephritis (TIN)?
Acute pyelonephritis
What changes can occur in the kidney if bacterial pyelonephritis is left untreated?
It will progress to chronic pyelonephritis, characterized by scarring and fibrosis –> thyroidization, and tubular atrophy. These changes lead to hypertension and renal failure.
What is this process called and what is it a result of?

Thyroidization of the kidney due to chronic pyelonephritis.
What the hell is the difference between tubulointerstitial nephritis (TIN) and acute interstitial nephritis/interstitial nephritis (AIN/IN)?
TIN is a general term for inflammation of the tubules or interstitium. AIN/IN is inflammation not caused by bacteria; usually caused by a hypersensitivity reaction to drugs.
Name the drugs that have the potential to cause what is seen in the photo. What is this disease called?
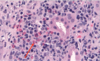
Intersitial nephritis - caused by penicillins (esp. methicillin), NSAIDs, sulfonamides
What is the cause of analgesic nephropathy? Briefly describe the pathogenesis of the disease and the morphological changes that occur in the kidney as a result.
Due to chronic use of acetaminophen + aspirin for >3 years.
Pathogenesis: NSAIDs inhibit COX, so there is no PGE2 synthesis by macula densa cells –> no vasodilation of the afferent arteriole to increase GFR.
Reduced blood flow due to an inability to make PGE2 and vasodilate ultimately leads to papillary necrosis.

Name four substances that have the potential to cause acute tubular necrosis (ATN).
Aminoglycosides, heavy metals, contrast dyes, myoglobin (from rhadbomyolysis)
Your patient has a slightly reduced GFR and they got a radiocontrast CT to evaluate renal function. They develop acute kidney failure. Biopsy shows the following. What is your Dx?
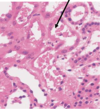
Acute tubular necrosis (ATN)
Can severe hypotension cause acute tubular necrosis?
Yeah
You have been managing a patient with resistant hypertension and note an increase in their serum creatinine. Check the pic. What is that called?

Hyalinosis
Describe two vascular changes in the kidneys that can occur in the setting of malignant hypertension (>180/120).
Fibrinoid necrosis (plasma proteins getting squeezed out of the arteriole) and onion skin lesions (intimal thickening and smooth m. and collagen proliferation).

Name the mutated genes and their corresponding chromosomes involved in autosomal dominant polycystic kidney disease (ADPKD).
PKD1 on chromosome 16
PKD2 on chromosome 4
Describe the morphological changes that occur in the kidneys of a patient with ADPKD.
Both kidneys become enlarged, with cysts that destroy the renal parenchyma

Name two major comorbidities associated with ADPKD.
- Berry aneurysms
- Polycystic liver disease
Is ADPKD common?
Yeah!
What is the genetic mutation involved in autosomal recessive polycystic kidney disease (ARPKD)? What is the typical outcome from this disorder?
PKHD1 fibrocystin gene mutation
Non-functioning kidneys in the fetus –> oligohydramnios –> lung hypoplasia and death
If fetus survives to birth, there is usually also congenital hepatic fibrosis needing a transplant.
Can patients with ESRD on prolonged dialysis develop a cystic kidney disease?
Yeah

Very simply, what is nephrotic syndrome?
Podocyte damage –> lots of proteins leak into the filtrate
Name four clinical findings suggestive of nephrotic syndrome.
1) Proteinuria –> 2) Hypoalbuminuria leading to 3) Edema
4) Hyperlipidemia cuz the liver thinks that will make up for the loss of protein
Name five differential diagnoses for nephrotic syndrome.
Glomerular-specific diseases:
- Minimal change disease
- Focal segmental glomerular sclerosis
- Membranous glomerulopathy
Systemic diseases:
- Diabetic nephropathy
- Lupus
Which glomerular disease is the most common cause of nephrotic syndrome in kids? How is it treated and what is usually the outcome?
Minimal change disease. Treat w/ steroids, typically resolves completely.
Describe the microscopic pathological changes of minimal change disease that can be seen on microscopy.
On light microscopy, shit looks normal.
On EM, you can see podocyte foot effacement (the feet look like they have coalesced).

Focal segmental glomerular sclerosis (FSGS) causes ________ syndrome clinically and is seen predominantly what patient population?
FSGS causes nephrotic syndrome and is seen mostly in black older teens and young adults
Describe the cellular pathological changes that occur in FSGS.
Podocytes get injured
Some podocytes die, exposing the underlying basement membrane.
Parietal epithelial cells reach out and attach to the exposed basement membrane.
Fibrosis ensues in these areas.







