ECG Theory Notes Flashcards
At normal paper speed of 25mm/s, how can we calculate the BPM if we know that 21 small squares are found between each QRS complex?
1 min = 1500 small squares
HR= 1500 /21 = 71 BPM
At normal paper speed of 25mm/s, how can we calculate the BPM if we know that 4 large squares are found between each QRS complex?
1 min = 300 Large squares
HR= 300/4 = 75 BPM
How can we calculate the BPM if we know that there are 19 QRS Complexes in 50 large squares? (paper speed 25mm/s)
50 Large squares = 10 s
19 x 6 = 114BPM
This is the clinical way of measuring HR.
How do we call a Patient with HR above 100 BPM?
Patient with Tachycardia
How do we call a Patient with HR below 60 BPM?
Patient with Bradycardia
What are the Adverse features of Bradycardia?
Shock
Syncope
Myocardial Ischemia
Heart Failure
What are the basic 6 problems related to Bradycardia?
1) Sinus Bradycardia
2) Sick sinus syndrome
3) AV Block
4) Escape Rhythms
5) AV Junctinal escape Rhythm
6) Asystole
What are the cardiac events that the PR interval connects between?
Start of Atrial Depolarization to the Start of Ventricular Depolarization
What are the risk factors of Asystole to be considered in Bradycardia?
Recent Asystole
Mobitz II AV block
Complete heart block with broad QRS
Ventricular pause > 3s
What is a general basic response in light of Adverse Bradycardia features?
500 mcg IV of Atropine
What is the cardiac event corresponding to the P wave?
Atrial Depolarization
What is the Cardiac event corresponding to the QRS Complex?
Ventricular Depolarizarion
What is the cardiac event related to the T wave?
Ventricular Repolarization
What is the corresponding cardiac event to the ST segment?
Pause in ventricular electrical activity before repolarization
What is the time period related to the QT Interval?
Total time taken by ventricular Depolarization and Repolarization
What is the U wave?
“Uncertain” - Interventricular Septal repolariztion or slow ventricular repolarization

19 QRS Complexes in 50 large squares (10 sec) means 114 Beats per minute
19 x 6 = 114
How do we differentiate between Narrow and Broad Tachycardia?
Narrow Tachycardia = < 3 small squares
Broad Tachycardia = > 3 small squares
Narrow complex tachycardia origins:
1) Sinus tachycardia
2) atrial tachycardia
3) atrial flutter
4) atrial fibrilation
5) AV re-entery tachycardia
6) AV nodal re-entery tachycardia
Broad complex tachycardia origins:
1) Ventricular tachycardia
2) accelerated idioventricular rhythm
3) torsades points
What are the two Main underlying questions one should ask (Hypothetically) when Identifying the paitent Cardiac rhythem?
1) Where does the Rhythem arise from?
(SA/ Atria/ AV/Vent. )
2) How is the Impulse conducted?
(Normal/Impaired/Accelerated)
What is the way to asses the state of the paitent and get the clinical context needed for ECG interpretation?
In other words what other information should be checked in order to interprate the ECG correctly?
ABCDE Aproach:
Airway - obstructed?
Breathing - Respiratory rate, chest precussions and auscultation, and oxygenation.
Circulation - Pulse rate, Blood Pressure and Capillary Refill time
Disabillity - Consciousness and Neurological State
Exposure - Making sure body is fully examinated
What should be checked if there is no Ventricular Activity Present?
Paitent - Pulse
Electrodes - Connected
Gain - Set to a High enough range
What is the basic set of 7 questions that should be answered to determine the HR properly from the ECG?
(By order)
(These will ultimatly let us know the Impulse conduction and Impulse origin)
1) How is the Paitent? (ABCDE)
2) Ventricular Activity Present?
3) Ventricular rate?
4) Ventricular rhythem Regular/Irregular?
5) QRS - Broad/Narrow ?
6) Atrial activity present?
7) Atrial activity and Ventricular Activity related?
What are the 3 classifications of ventricular rate?
1) Bradycardia - below 60 BPM
2) Normal - Btw 60 and 100 BPM
3) Tachycardia - above 100 BPM
How can we tell if the Ventricular Rhythem is Regular or Irregular?
Examples for Irregular and Regular Rhytems?
QRS Complexes spacings are Constant (Equal) = Regular
QRS Complexes spacings are Variable = Irregular
Regular Rhytems - Atrial Tachycardia, AV Block
Irregular Rhythems - Sinus Arrhythmia (Cyclic change from respiration) and Atrial Fibrilation (Choatic Rhytem)
What is the Importnace of the finding out if the QRS Complex is Narrow or Broad?
What is the meaning of each?
Determining the Origin of the Impulse!
- Narrow = Fast Depolarization of Ventricular Myocytes: AV to His and Purkinje transition has happened, Supraventrucular Origin.
- Broad = Slow Depolarization of Ventricular Myocytes: 1) Supraventricular origin with Aberrent conduction 2) Ventricular Origin
What are the 4 types of Atrial Activity?
1) P waves (Regular)
2) Flutter Waves
3) Fibrilation Waves
4) Unclear Activity
From the P wave look, how can we tell the origin of the Impulse?
P wave upright - SA Node
P wave inverted - AV Node
How can we differintaite between Atrial Fibrilation and Atrial Flutter?
Fibrilation - 400-600/Min, Choatic low-amplitude activity
Flutter - 300/Min, Sawtooth activity
When examining the relationship between the Atria and Ventricels rhythem activity, what should be noticed?
P / QRS Ratio: (Number of inflections)
if 1 = Normal
if above 1 = conduction between Atria and Ventricles is partialy blocked!
if below 1 = AV Dissociation, Ventricles are operating independently (Faster)!

(1) Normal Sinus Rhythem
A) P waves are upright (lead II)
B) 1:1 P/QRS ratio
C) HR is 75/min - CONSTANT
(in Lead aVR P wave is Inverted)

(2) Sinus Arrhythmia (Physiological)
A) P waves are upright (lead II)
B) 1:1 P/QRS ratio
C) HR Increases during Inspiration
(in Lead aVR P wave is Inverted)

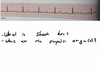
(3) Sinus Bradycardia
A) P waves are upright (lead II)
B) 1:1 P/QRS ratio
C) HR is lower than 60 BPM (46/min here)
(in Lead aVR P wave is Inverted)
What are some possible causes for Sinus Bradycardia?
1) Apears in sleeping athletes
2) Beta-Blockers
3) Ischemic heart disease
4) Hypothyrodism
5) Hypothermia
6) Raised ICP (Cushing reflex)
7) Sick sinus syndrome

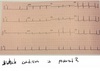
Sinus Tachycardia
P/QRS ratio is 1:1, P wave is Normal, HR>100BPM
1) Drugs like Adrenaline/ Atropine
2) Anxiety/Fear/Pain/Fever/Excercise
3) Ischemic Heart disease and H. Failure
4) Pulmonary Embolism
5) Anaemia or Fluid loss
6) Hyperthyrodism
In Sinus tachycardia never attempt to slow the Heart rate before you ____________ !
In Sinus tachycardia never attempt to slow the Heart rate before you have established the cause! Could be:
1) Drugs like Adrenaline/ Atropine
2) Anxiety/Fear/Pain/Fever/Excercise
3) Ischemic Heart disease and H. Failure
4) Pulmonary Embolism
5) Anaemia or Fluid loss
6) Hyperthyrodism
What are the problems presented in Sick Sinus syndrome?
1) Sinus Tachycardia
2) Sinus Bradycardia
3) Sinus Arrest
4) SA Block
What will apear on the ECG strip when there is Sinus arrest?
P wave will suddenly fail to apear in the expected place.
It will apear after a variable gap or AV will compensate with a “Junctional escape beat”
What happens in SA Block?
Sinus Node is depolerized normally.
Impulse doesnt reach the Atria.
P wave will be missing but will apear regulary in the nexy cycle (Usually).
Sick Sinus Syndrom:
Symptoms and Causes?
Symptoms: Dizziness, Fainting and Palpitations.
Most common cause is degeneration of SA Node, But also:
1) Ischemic Heart Disease 2) Drugs 3) Cardiomyopathy
4) Amyloidosis 5) Myocarditis

Ectopic Beats:
Upper is Atrial Ectopic Beat (Extrasystole)
Early and Differently Shaped P wave (With following QRS) indicating the different origin in the Atria
Lower is AV Junctional Ectipic Beat
Early and Inverted P wave (With following QRS), Indicating that origin is low atria in AV Node.

Atrial Fibrilation (AF)
1) First Diagnosed AF
2) Paroxysmal AF - Self terminating, 2 to 7 days
3) Presitent AF - more than 7 days
4) Long lasting AF - more than a year, attempt to restore Sinus Rhythem
5) Permenant AF - more than a year, NO attempt to restore Sinus Rhythem

Atrial Fibrilation (AF)
Absence of Distinct P wave
Irregulary Irregular Ventricular Rhythem
Atrial Fibrilation can be Asymptomatic, but generally what are the possible Symptoms?
1) Fast Irregular Palpitations
2) Breathlessness
3) Fatigue
Causes of Atrial Fibrilation?
Give an Important Risk arising from it.
1) Hypertension and Hyperthyrodism
2) Ischemic and Vulvar Heart disease
3) Cardiomyopathies and Myocarditis
4) Atrial Septal Defect (Congenital)
5) Alcohol and Heart Surgary
6) Pulmonary Embolism and Pneumonia
- Thromboembolism can develop from AF (Risk)
What are the Key issues for managing paitents with Atrial Fibrilation?
How?
- Reducing Stroke Risk - AF increases risk 5 times! - Warferin is a preferred treatment
- Ventricular Rate Control - Beta Blockers
- Rhythm Control - Cardioverting to Sinus Rhythm
How does Electrical Cardioversion for AF paitents work?
Alternative Surgical Procedure?
Intravenous Heparin is initiallly introduced and followed by a 4 weeks long oral anticoagulnts introduction.
Diffibrilator is set to synchronized mode with 100 -120J biphasic and increases as the procedure goes on.
Alternatively Catheter Ablation of AF could be used, Invasive surgical process - Last line option.

Atrial Flutter
Could be considered a subtype of Atrial Tachycardia
Recognizable by :
Sawtooth Baseline
Attrial Rate - 300/min and Ventricular Rate - 150/min
Indicating an 2:1 AV block

Atrial Flutter
AV Node could not keep up with the Impulse rate comming from the Atria and there is an AV Block formed.
Usually AV block - 2:1, Here the Upper one is 4:1 and the Lower one is Variable.
Type 1 : Cavotricuspid Isthamus
Type 2 : Less Common, After Cardiac Surgery in Areac of Scartissue.
What is the way to present the Atrial Flutter ECG sawtooth baseline more drastically for diagnostic purposes?
What is the treatment?
What are the Risks of Atrial Flutter?
Messaging of the Carotid Sinus or Adenosine input.
Normal Sinus Rhythm can be restored with Electrical Cardiovesrion like in AF, but Radiofrequency Ablation is more favorable here for the Sinus rhythm maintenance.
In Atrial Flutter the irregular blood flow promotes the formation of thromboembolisms therefore antithrombotic treatment is also considered.

Atrial Tachycardia
Could be Multifocal or Focal
Characteristics:
Inverted P wave (Lead 2)
AV Block
What is the most probable cause of Atrial Tachycardia?
What could be mistaken to be Multifocal Atrial Tachycardia?
What other condition could be considerd as a subtype of Atrial Tachycardia?
- Digoxin Toxicity
- Atrial Fibrilation (due to Irrgular nature)
- Atrial Flutter

AV Re-Entry Tachycarida
1) Accesory Pathway (Alternative AV circuit)
2) Delta Wave - slurred Initial Upstroke caused by Myocyte to Myocyte followed by normal QRS
- Lacking intrinsic slowness of AV Node, PR is short (<0.12s)

Wolff - Parkinson - White Pattern (WPW)
Allows for Atrioventricular Re-Entry Tachycardia (AVRT)
Type A - Accessory Pathway on Left side
Type B - Accessory Pathway on Right side

(a) Orthodromic AVRT:
95%, Regular and narrow QRS , HR - 130-200
Also Known as Short RP Tachycardia; Inverted P wave represents Retrorgade accessory depolerizing the Atria.
(b) Antidromic AVRT:
5%, Ventricular Tachycardia Broad and Regular QRS (Myo. to Myo.)
Both (a) and (b) Have the WPW Pattern

Orthodromic AVRT
There is a regular-narrow complex tachycardia (204/min) with inverted P waves (distorting the ST segments) following each QRS Complex
What other arrhythmia could occur due to WPW ?
What are the Termination Possibilities of AVRT?
Prevention of AVRT?
WPW could yeild Ventricular or Atrial Fibrilation.
to Terminate AVRT we have to increase the vagal inhibition of the AV Node by either Valsava Manuever or Carotid sinus massage. (Works for AVNRT as well)
In order to prevent further episodes of AVRT we can use catheter ablation of the Accessory Pathway.

Normal AV Node Conduction
Occurs via the Fast Pathway

Atrioventricular Nodal Re-Entry Tachycardia
a) An ectopic beat is travelling down the slow pathway when the fast pathway is refractory
b) The Impulse than conducts back up the fast pathway, which has recovered from the refractory period.
(This is the typical type called slow-fast AVNRT aka as Shirt RP Tachycardia)

Atrioventricular Nodal Re-Entry Tachycardia (AVNRT)
There is a regular-Narrow Complex tachycardia
P wave may showen at the end of the QRSs in some leads.
If ECG shows WPW patterns than this is AVRT (Similar).
What are the Supraventricular Tachycardias?
Sinus Tachycardia
Atrial Fibrilation
Atrial Flutter
Atrial Tachycardia
AVRT
AVNRT
(some reffer only to AVRT and AVNRT)
Give 5 examples for Ventricular Rhythms :
Ventricular Ectopic Beat
Accelerated Idioventricular Rhythm
Monomorphic Ventricular Tachycardia
Polymorphic Ventricular Tachycardia
Ventricular Fibrilation

Ventricular Ectopic Beat
(Ventricular Extrasystole)
Types: Ventricular Bigeminy, Ventricular Couplet, Ventricular “R on T” .
Identified by its Broader QRS (Myocyte to Myocyte)

Ventricular Bigeminy
Every normal complex is followed by ventricular ectopic beat

Ventricular Couplet
Two ventricular ectopic beats occuring one after another

“R on T” VEB
a ventricular ectopic beat occuring on top of the T wave of the previous Beat
How do we classify VEBs
(Ventricular Ectopic Beats)
Frequent: above 60 per Hour
Multifocal / Unifocal (Origin Based)
Amount : Bigeminy / Trigeminy / Quadrogeminy / Couplet
* If there are three or VEB = Ventricular Tachycardia



VEBs arising from the Right Ventricular Base
as the table mentions:
Positive QRS in inferior Leads and LBBB
are indications for Right Base VEB
also it presents in a Couplet type
(This card is extra knowledge)
What are the characteristics of Accelerated Idioventricular Rhythm?
How does it look like on an ECG?

How do we distinguish between Ventricular Tachycardia and Supraventricular Tachycardia with aberrant conduction?
(Hint: Related to QRS complex and disscused in preveous cards)
Broad Complex Tachycardia is always assumed to be VT Unless proven otherwise! (80% Dominance)
The presence of Atrioventricular Dissociation could also indicate (in 50% of) VT: Independent P Wave Activity, Fusion Beats, Capture Beats.
SVT Could be recognized by responsiveness to AV Node manipulation

Atrioventricular Dissociation
1 ) Independent P Waves - Deforming the QRS
2 ) Capture Beats - Overriding QRS
3) Fusion Beats - Atrial and Ventricular Activation Simultaneously

Polymorphic Ventricular Tachycardia
Two Catagories (With underlying cause):
1) Normal QT - from MI, Coronary Reprefusion etc…
2) Prolonged QT/ “Torsades de Pointes” - Hypocalcemia, Acute Myocarditis, Long QT Syndrome etc..

Ventricular Fibrillation (Causes):
1) MI 2)Cardiomyopathy 3)Myocarditis
4) Electrolyte Disturbance 5) Drugs (Pro-Arrthymic ones)
6) Long QT and Barguda Syndromes
7) Cardiac Trauma 8) Electrical Shock



(1) SA Block - Two beats were ‘skipped’ , although the SA node was depolerized conduction was blocked.
(2) First Degree AV Block - No beats were ‘skepped’ but there was a Prolonged PR Interval.
Normally PR interval is 0.12 - 0.2 Sec
Here it is 0.28 due to Partial Blockage.

Second-Degree AV Block
- Mobitz I - PR gradually lengthens with each beat, until one P wave fails to produce a QRS complex. (the one Shown in the Picture!)
- Mobitz II - PR fixed and normal in each beat, occasionally one P wave fails to produce a QRS complex .
- 2:1 AV Block - Alternate P waves are not followed by QRS complexes

Second-Degree AV Block
- Mobitz I - PR gradually lengthens with each beat, until one P wave fails to produce a QRS complex.
- Mobitz II - PR fixed and normal in each beat, occasionally one P wave fails to produce a QRS complex .
- 2:1 AV Block - Alternate P waves are not followed by QRS complexes (the one Shown in the Picture!)
3rd Degree AV Block
There is a complete block of AV conduction, Sinus Rhythem in the Atria and Narrow Complex (‘Junctional’) Escape Rhythm in the Ventricles.
*Notice the Irregular Change in Length of the PR interval from beat to beat!
**This is NOT the same as Atrioventricular Dissociation as QRS is Narrow we understand that it has Supraventricular origin of impulse!
Possible causes of 3rd Degree AV block?
(Extra Knowledge)
1) Lyme Disease
2) Congenital Disorders
3) Fibrosis or Calcification of Condiction System
4) Myocardial Infiltration
5) Neuromuscular Disease
6) Hypothyrodism




What phenomena is unique to LBBB ?
What are other Criteria help in identifying LBBB?
(Left bundle branch block)
-Interventricular Dyssynchrony
- “Notched Tower” Could be seen on lead I instead of V6 + Wide QRS on V6

3rd Degree AV Block
P wave rate is higher than the QRS complex rate.
*Notice the Irregular Change in Length of the PR interval from beat to beat!
**This time we can actually see Atrioventricular Dissociation as QRS is Broad we understand that it has Ventricular origin of impulse!
What Accelerated Conduction Conditions are there?
1) Wolff-Parkinson-White Syndrome (WPW)
2) Lowon- Ganong - Levine (LGL)
3) Accelerated AV Nodal Conduction (Intrinsic)
Complete the sentence:
A quick rule of thumb regarding assesing the QRS Axis is that if the QRS complexes are predominantly positive in leads I and II, the QRS axis is ____ .
Normal
A quick rule of thumb regarding assesing the QRS Axis is that if the QRS complexes are predominantly positive in leads I and II, the QRS axis is Normal .


What is the Normal Axis Range?
-30 to +90 Degrees
(+90 to 120+ is an extention with high likelihood of abnormalities)
Knowing that lead I and lead II are positive tells us that the QRS Axis is normal.
How?
(Remeber the Mental Image of the Geometry behind it)
(Ignoring aVF for now)



What are the conditions that would present as Right Axis Deviation in the ECG?
Right Axis Deviation Related Conditions:
- Right Ventricular Hypertrophy
- WPW Syndrome (Accessory Pathway on Left)
- Antrolateral Myocardial Infraction (Impluse away)
- Dextrocardia
- Left Posterior Fascicular Block (very Rare)
- Also in Healthy Individuals
What are the conditions that would present as Left Axis Deviation in the ECG?
Extreme Left Axis Deviation Related Conditions:
- Left Anterior Fascicular Block - (Fibrosis/ MI)
- WPW Syndrome - (Accessory Pathway on Right)
- Inferior Myocardial Infraction (Impluse away)
- Ventricular Tachycardia
- Also in Healthy Individuals






Extreme Right Axis Deviation, Causes?
(Extra Knowledge, This is rare and mostly apparent due to misplacement of electrodes)
Extreme Right Axis Deviation, Causes:
- Ventricular Tachycardia with extreme axis shift
- Ventricualr Pacing

Sinus Arrest
Arrows show the position where the P waves should have appeared

Biphasic P Wave
Normal P wave of Lead V1
Where/When would we find Inverted P waves presenting?
-Electrodes Missplacement
- Lead aVR
-Dexocardia
-Atrial Ectopics
-AV Junctional Rhythems
-Ventricular Tachycardia (Retrograde Conduction)
-Ventricular Ectopics (Retrograde Conduction)

P Pulmonale - Tall P waves
Enlargement of Right Atria
Above 2.5 Small Squares (3.5 is shown here), Causes:
- Primary Pulmonary Hypertension
- Secondary Pulmonary Hypertension
- Pulmonary Stenosis
- Tricuspid Stenosis

P Mitrale
P waves are wider than 3 small squares (0.12 Sec)
They have a minor Notch, Could indicate an enlargement of the Left Atria.
This is usually a result of Mitral valve Disease.
It increases the Risk of Atrial Fibrilation.
What are the Basic Parameters of a Normal PR Interval?

What are the conditions relevant to short PR Interval?
Shorter than 0.12 sec !
(Conditions you should think of..)
PR Interval<0.12 sec
- AV Nodal rhythm
- Wolff-Parkinson-White Syndrome
- Lown-Ganong-Levine (LGL) Syndrome
- Accelerated AV nodal conduction

AV Nodal Rhythm
- Inverted P wave: Origin of Impulse is located below SA, around Atria.
- PR Interval is shorter than 3 small squares (0.12 sec), which means Origin of Impulse is from low atria in the area of AV Node.
**Atria depolarization impulse is sent while Ventricles depolarization impulse, PR is Reduced.

WPW Pattern
Delta Wave: Ventricular Pre-Excitation (slurred R wave)
Short PR Interval: The time diffrence between Atrial and Ventricular Depolarization is shorter.
This Implies that there is an AV re-entry Tachycardia (AVRT) episode caused by an Accesory pathway (Bundle of Kent) in this individual heart.
Lown-Ganong-Levine Syndorme (LGL)
- Cause
- ECG Signal
Lown-Ganong-Levine Syndorme (LGL)
- Accessory Pathway (James fibers) bypass the AV Node and reconnects to the Bundle of His (not to Ventricular Muscle like in WPW). AVRT Present!
- No Delta wave like in WPW but shorter, PR Interval is Shorter, AVRT - meaning HR is High. This a pretty theoretical diagnosis and it is still a debate whether this exists.

Accelerated AV Nodal Conduction
PR is shorter than 0.12 sec
No pain or other symptomes
No history of AVRT

First degree AV Block - PR is Longer than 0.2 sec
Commonly caused by Vagally induced Bradycardia, AV nodal conduction decreases as Vagal tone rises.
Other causes are - Ischemic heart diseases, Hyper/Hypo- Kalaemia, Acute rheumatic myocarditis, Lyme disease, Beta blockers, Digoxin and rate modifying calcium channel blockers.
What are the conditions where the PR Interval is Inconsistent or could Not be measured?
PR Interval - Inconsistent or can not be measured
- Mobitz Type I AV Block
- Mobitz Type II AV Block
- 2:1 AV Block
- Third-Degree (Complete) AV Block

Mobitz type I AV Block
There is a progressive lengthening of the PR Interval, a P wave then fails to be conducted, then the PR interval ‘Resets’ and the cycle comes again.
Calling a cardiologist is essential and should be fast.

Mobitz Type II AV Block
The PR Interval is normal and constant, but there is a occasional failure of AV Condoction and a P wave is not followed by QRS Complex.
Calling a cardiologist is essential and should be fast.

2:1 AV Block
Every alternative P wave fails to be conducted.

3rd Degree AV Block
Atrial (P wave) rate is approximately 75/Min
Ventricular (QRS) rate is around 30/Min
No relationship between P and QRS.
Call a cardiologist in this situation!
*Atrioventricular Dissociation is happening only if QRS rate is higher than P rate.
PR interval which is not Isoelectric
What are the most probable causes of PR Interval Elevation and PR Interval Depression?
PR interval which is not Isoelectric
PR Interval Elevation - Pericarditis
PR Interval Depression - Atrial Involvment in Acute Coronary Sydrome.

Atrioventricular Dissociation
The Ventricular (QRS) rate is higher than the P rate.
QRS Complexes simply march into the P waves.
There are occasional ventricular ectopic beats.
In complete (3rd Degree AV) Block, how can we tell whether the Origin of Impules is below or In the AV Node Area?
3rd Degree AV Block
QRS Complex is Narrow - From Bundle of His (In AV Node Area).
QRS Complex is Broad - From Left or Right Bundle Branches (Below AV Node Area).
What are the leads in which Q wave detection may indicate Pathological conditions?
Pathological Qs
aVF
V1-V4
III - if the T wave is not inverted
What are the variations in Q waves Parameters that are considered Pathological or Abnormal?
Pathological or Abnormal Q waves
More than 1 small square wide
More than 25% Precent of the Height of the R wave

Septal Q waves
Normal, Small Q waves - Seen in I, II, aVL, V5, V6 Leads

Normal Q waves in Lead III
Narrow Q waves that are followed later by inverted T waves.

SוQוווTווו Pattern
- This means Pulmonary Embolism
- There is also T wave Inversion in Leads V1-4
- Paitent with Beta blockers so Sinus Rhythm
What could be the Problems with a Paitent that has Q waves that are Wide or Deep?
Specify as much as possible..
1. ST Segment Elevation myocardial Infarcation
2. Left ventricular Hyperthrophy : Larger septum=Bigger Q wave
3. WPW : Delta waves looks like Infarction (Depending on location of Accessory Pathway)
4. Bundle Branch Block : “Rabbit ears on V1…”

Anteroseptal ST Segment Elevation MI (Day 2)
Day after MI the region effected is harder to depolerize - Deep Q waves are seen in leads V1-3 with residual ST elevation.

Inferior Myocardial Infarction (After a year)
Deep Q waves are present in the area; Leads II, III and aVF
Why do deep Q waves are seen in MI?
MI - Q Waves
- When an area is necrotized in the myocardium it is harder to depolerize it; hence the specific area observing lead will see the electrical activity flowing away from it = Negative Deflection which is your Q wave on the ECG!

WPW - Inverted Delta Wave
Depending on the location of the Accessory Pathway the Delta wave could seem like a deep Q wave!
This is a “Pseudo-Infarction” !
Use the Upright Delta wave in Lead II to not be confused by it.

Normal ECG QRS Complex (R and S)
- R wave Increases in height from Lead V1 to V5
- R wave is smaller than S wave in lrads V1 and V2
- R wave larger than the S wave in leads V5 and V6
- Tallest R wave is max: 25 mm
- Deepest S wave is max: 25 mm
*** Only in 1mV=10mm Calibration of ECG

Left Ventricular Hypertrophy
- There are Taller R waves in leads I, aVL, V5 and V6 with Deeper S waves in V1, V2 and V3.
- Best Diagnostic Criteria is Sokolow-Lyon Criterion: The Sum of the S wave in Lead V1 and R wave in Lead V5 Should be Less than 35 mm .

Right Ventricular Hypertrophy
- Key for Diagnosis - Dominant R wave in V1 (Opposite to the regular R progression)
- Associated with: Right Axis Deviation, Deep S waves in V5 V6 and RBBB
What are the is Important to look for after assembling a diagnosis of RBBB, LBBB, Left or Right Ventricular Hypertrophy?
Strain Pattern
ST Segment Depression and T wave Inversion

Posterior Myocardial Infarction
- There is a dominant R wave in Lead V1
- ST Segment depression in anteroseptal chest leads (V1-4)
- Tall and Upright T waves

Wolf Parkinson White Syndrome (Type A)
- Dominant R wave in Leads V1-3 + Short PR with Delta waves
- Left sided Accessory Pathway: Dominant R in V1-3 (Right sided : Dominant S in V1-3)

Dexocardia
- R waves are decreasing as chest leads progress in number.
- Right sided chest leads allow a more “normal” ECG
What should we suspect if the QRS Complex is too small?
(Calibration 1mV=10 mm)
Small QRS
- Obesity
- Emphysema
Both conditions increase the distance between the electrodes and the heart.
If the QRS complex is getting smaller as the ECG measurement progresses - Consider Pericardial Effusion
(other card)

Pericardial Effusion
Upper - Small QRS, because of fluid accumulation in the Pericardium less current reaches the electrodes
Lower - Electrical altenans: variations in QRS size
Beck’s triad (Severe Clinical Symptomes): Low BP, Elevated Jugular Pressrue and Impalpable Apex Beat.
This could indicate the development of a Cardiac Temponade! - Urgent Pericardial Aspiration is required!
What are the conditions associated with a wide QRS Complex (More than 0.12 Sec or 3 mm)?
Wide QRS
- Bundle Branch Block
- Ventricular Rhythms
- Hyperkalaemia

Cabrera’s Sign
The Presence of a Notch 40msec into the ascending portion of the S wave in Leads V3 and V4.
This is an Indication of previous Myocardial Infarction in a paitent with LBBB.

Incomplete Left Bundle Branch Block
There is an abnormal QRS morphology in V6 - “Notched Tower” - that signfys that this is a LBBB, But the duration and all other QRS Complexes are fine in shape meaning this is an Incomplete block.
What are the conditions to consider once spotting a ST segment elevation on the ECG?
(Some of the answers are extra knowledge)
ST Segment Elevation
- Myocardial Infarction
- Left Ventricular Aneurysm
- Prinzmetal’s (vasospastic) angina
- Pericarditis
- LBBB
- Brugada Syndrome
- High take-off
What are the 3 types of Acute Coronary Syndrome?
(Memorize the chart)

What are the 4 stages of evolution Myocardial Infarction?
What changes in ST Segment, T wave, Q wave and R wave?
(Molnar’s Figure)


Inferior STEMI
- Leads II, III and aVF show ST segment Elevation
- Leads I and aVL show ST segment Depression
- This is happening as the ECG is recorded and the orientation is assessedby the location of the Electrodes on the body wall.

Anterior STEMI
- Leads V1-4 show ST segment elevation
- This is happening as the ECG is recorded and the orientation is assessedby the location of the Electrodes on the body wall.

Anterolateral STEMI
- leads V4-6, I and aVL are showing ST elevation
- This is happening as the ECG is recorded and the orientation is assessedby the location of the Electrodes on the body wall.

Left Ventricular Aneurysm
- 10% survival rate
- Presistant ST segment elevation indicate it
- Could present as Heart failure, Embolic events and further arrhythmias

Prinzmetal’s (Vasospastic) Angina
- ST Segement elevation and settling down is happening while the paitent experiences pain and afterwards the pain ends (unlike STEMI).

Pericarditis
- ST Segment Elevation in almost every lead!
- ST Segment elevation is charactristically ‘saddle shaped’ (concave upwards)
- T wave inversion occurs only after the ST Segment have returned to baseline.
- Q waves do not develop (not as after STEMI)

LBBB -Appropriate Discordance
- Seeing the ‘Notched Tower’ we can understand that this is a LBBB.
- In leads V1-V3 there is an apparant “ST Elevation”, The baseline ST segments and T waves tend to be shifted in a discordant direction (“appropriate discordance”), which can mask or mimic acute myocardial infarction.
- Sgarbossa Criteria allows the STEMI Diagnosis here

Brugada Syndrome
- Heredetary condition, Cardiac Sodium channel Defect, present as RBBB (“rabbit ears V1”) and Presistant ST elevation in Leads V1-V3.
- Thought to be responsible for 50% of Sudden cardiac death with ‘normal’ heart.
- Type 1: Coved ST elevation with Inverted T waves.
- Type 2: Saddle ST elevation with Positive/Biphasic T
- Type 3: Saddle ST elevation with Positive T wave

High Take-off
- ST segment elevation is shown in leads V2-V4 following a deep S wave.
- This is considered as early repolarization, a variant of Normal ECG signal in Chest leads when presented this way.
- Notice: No reciprocal ST segment depression in other leads as in Acute Coronary Syndromes.
What are the conditions to consider if a paitent presents an ECG with ST segments that are the Depressed?
ST Segment Depression
- Myocardial Ischemia
- Acute Posterior Myocardial Infarction
- Reciprocal changes in ST segment elevation myocardial infarction
- Drugs (e.g. digoxin)
- Ventricular Hypertrophy with ‘Strain’

Myocardial Ischaemia
- Shows only when patient experiences Angina!
- ST segment Depression in Leads V3,V4,V5 and aVF
- Inversion and Pseudonormalization of T waves could also be seen in ECG recoredings.
Digoxin Effect
- ‘Reverse Tick’ ST Segment Depression is shown in lateral leads (normally in leads with higher R wave).
- Symptoms Depends on context of uptake and level but generally it could cause anorexia, nausea, vomiting, abdominal pain and visual disturbances.
- Theraputic: T reduction and QT Shortening
- Toxicity: T inversion and arrythmias due to low K

Ventricular Hypertrophy with ‘Strain’
- Leads of interest are V5 and V6
- ‘Strain’ pattern is said to be present when in addition to tall R waves and Deep S waves there is also - ST segment Depression and T wave Inversion.
- The mechanism of ‘Strain’ is yet unclear.

J (Osborn) Waves
- Small positive deflection at the junction between the QRS complex and the ST Segment, shown normally in inferior and lateral leads.
- Associated with 80% precent of Hypothermia cases but could apear in other patients.
- Hypothermia patients may show other ECG abnormalities such as Atrial Fibrilation, AV block, Ventricualr Arrhythmias and even Asystole.

Hyperkalaemia
- Tall tented T waves
- Flattening and even loss of P wave (Severe)
- lenghening of PR interval
- Shortening of the QT interval
- Widening of the QRS complex (Severe)
- Ventricular Fibrilation or Asystole
**Confirmed only by Plasma level Pottasium meaurments and requires urgent treatment

Acute Anterior Myocardial Infarction
- Tall Hyperacute T waves may a rise from a localized Hyperkalaemia caused by damaged Myocytes that release Pottasium as they die. This is an Early stage on acute coronary syndrome.
- Here we see this represent in leads V2 -V4, the Anteroseptal Leads.
- Identifying the border between tall and normall T waves is always subjective and needs practice.
What are the possible conditions for an ECG with Small or Tall T waves?
(‘small’ and ‘Tall’ is a subjective term and simply needs practice to learn how to Identify)
Small T waves
- Hypokalaemia
- Pericardial Effusion
- Hypothyrodism
Tall T waves
- Hyperkalaemia
- Acute Coronary Syndrome

Hypokalaemia
- ECG presents Small T waves, Prominent U waves First Degree AV Block and Left Axis Deviation.
- In other cases it can present Depression of ST segment as well.
- Symptoms that should occur together with it are muscle weakness and Cramps.
- Happens normally after use of Diuretics
which Leads have Inversion of T waves Normally?
Inverted T waves - Normally in:
- Lead aVR and V1
- Lead V2 in young People
- Lead V3 in Black People
- Lead III could also transiently show this (after holding a big breath disappears)
What is unique to Myocardial Ischemia in regard to T waves?
What is the term for the temporarily change in orientation of those T waves?


Wellens Sign
- Presented in Patients with unstable angina, here it is shown in the anterior chest leads (V2-V3) mostly.
- It is a Deep T wave Inversion that spans over 2mm in normal calibration.
- It represents Proximal Stenosis in the LAD, Left anterior Descending coronary artery - Should be confirmed with Angiography.
Apart from Myocardial Ischemia, what other conditions cause T wave Inversion?
(Refering only to those that allow usage of ECG as a diagnostic tool and not as supporting symptom)
T wave Inversion
- STEMI
- NSTEMI
- Left Ventricular Hypertrophy with Strain
- Digoxin Effect
- Repolarization Abnormalities following Paroxysmal Tachycardia
- Bundle Branch Block
- Pericarditis and Ventricualr Pacing

T waves Inversion ECGs
- a) Evolving STEMI: after ST elevation returns to baselineit continues as T inversion. (Q waves also).
- b) Digoxin Effect: Reverse Tick ST segment continues as T wave Inversion in V5-V6.
- c) ‘Strain’ Pattern in Left ventricualr Hypertrophy, Large QRSs show in lateral leads.
Which Lead will usually be chosen for measurment of QT Interval?
What are the Limits for Men and Women?
How do we know whether the QT interval is Long/Short/Normal?
QT Interval
- The Lead that has the Longest QT interval will be measured - Usually V2 or V3
- Upper limit: Men - 460 msec, Women - 450 msec
- Lower limit for Both Sexes: 390 msec
- These limits are not set in stone and calculation aids to get the Idea of a specific patient limit, the faster the heart rate the shorter the QT. (QTc=Corrected)
- Bazett’s Formula: QTc = QT /√(RR)
What are the Conditions that are to be considered in cases when the QT interval is Longer than Normal?
Long QT Interval
- Hypocalcaemia-Shows Trousseau Sign :carpal spasm when occluding brachial artery with cuff.
- Anti-arrhythmic Drugs effect - may cause ‘torsades de pointes’.
- Acute Myocarditis - along with ST alteration, T inversion, Arrhythmias and Heart Blocks.
- Long QT Syndrome-Pottasium or Sodium channel Defects, High Risk of Arrhythmias+Cardiac Arrest.
What are the Conditions that are to be considered in cases when the QT interval is Shorter than Normal?
Short QT Interval
- Short QT Syndromes - Calcium or Pottasium Defects, High Risk of Arrhythmias+Cardiac Arrest.
- Hypercalcaemia - along with U wave, Cardiac Arrest is very possible in this term.
- Hyperkalaemia- High Risk of Arrhythmias+Cardiac Arrest.
- Digoxin Effect
- Hyperthermia

U wave
- If Prominant: Hypokalaemia, Antiarrhythmics Drugs or Digoxin.
- If Inverted: (In over 90% these present)
- Ischemic Heart disease
- Hypertension
- Valvular Regurgitation
- Dilated Cardiomyopathy

Artificial Pacemakers
- Upper ECG - Ventricular Pacing: Spikes are followed by QRS Complex
- Lower ECG - Atrial Pacing: Spikes are followed by P wave
