RENAL PATHOLOGY 2 Flashcards
Covers Vascular Kidney Disorders & Tubulointerstitial disorders,
Etiology of chronic pyelonephritis
oInadequately treated acute pyelonephritis
orecurrent and persistent bacterial infection due to urinary tract obstruction, urine reflux, or both
What electrolyte imbalance must be watched for in the recovery phase of acute tubular injury?
Hypokalemia
Pre renal causes of acute kidney injury due to volume sequestration
pancreatitis, peritonitis, rhabdomyolysis
Underlying mechanism for Thrombotic Thrombocytopenic Purpura
Deficiency of ADAMTS13–> Very large vWF multimers –> bind platelet surface glycoproteins and activate platelets spontaneously –> microthrombi

Gross morphology of reflux associated chronic pyelonephritis
Scars in the upper and lower poles
Irregular, discrete overlying deformed and blunt calyces

Why is there eventual supression of renin synthesis in bilateral RAS/ RAS in a solitary functioning kidney?
Lack of pressure natriuresis
(see image for detailed explanantion)

3 causes of Classical Distal Renal Tubule Acidosis (Type 1)
- Sjogren Syndrome
- Rheumatoid arthritis
- Drugs- Lithium
Morphology of chronic transplant rejection
- intimal thickening , vascular occlusion
- interstitial fibrosis, tubular atrophy

Morphology of acute cellular rejection
- extensive interstitial inflammation and tubular inflammation
- Inflammation of vessels with/without necrosis
definition of oliguria
urine output of less than 400 mL/day or less than 20 mL/hr.
In a patient with bilateral functioning kidneys and unilateral RAS, what happens to the renin levels in the non stenotic contralateral kidney?
decreased renin secretion
How does typical HUS lead to microthrombi formation?
Shiga like toxin(Stx) binds to the globotriasylceramide Gb3 receptor on the renal endothelium –> damage to the endothelium–>platelet activation and vasoconstriction, reduced NO –> microthrombi.
Important renal manifestation of invasive cervical cancer?
bilateral hydronephrosis and renal failure
Diagnosis?
fever+ eosinophilia+ rash + hematuria, rising serum creatinine
Acute Drug-Induced Interstitial Nephritis
Morphologic feature of analgesic nephropathy
Papillary necrosis assoc with dystrophic calcification

Identify this important cause of renal artery stenosis from the clues below:
young to middle aged female hypertensive patients
mid and distal portion of the artery
“string of beads” on angiography
Fibromuscular disease
Mechanism of analgesic nephropathy
Phenacetin and its metabolites concentrate in the medullary interstitium–> induce generation of reactive metabolites–> direct covalent binding and oxidative damage –>cell injury
Kidney morphology in multiple myeloma
Dilated tubules with eosinophilic casts with Tamm-Horsfall protein trapping light chains

Post renal causes of acute kidney injury
- obstruction at the urethra or bladder outlet
- bilateral ureteral obstruction
- unilateral obstruction in a patient with a single functioning kidney.
Gross appearance of the kidney in malignant nephrosclerosis
fibrinoid necrosis + intraluminal thrombosis and rupture of glomerular capillaries and arterioles –> petechial hemorrhage on the cortical surface –>flea bitten kidney appearance

Morphology of antibody mediated acute rejection
inflammation of glomeruli and peritubular capillaries

Two microscopic features of chronic pyelonephritis
Thyroidization of tubules – atrophied/dilated tubules with colloid like casts
Chronic interstitial inflammation and fibrosis

Pre renal causes of acute kidney injury due to decreased circulating blood volume
Hemorrhage
Burns
Diarrhea
Diuretics
Gross appearance of the kidney in benign nephrosclerosis
Finely granular cortical surface (grain leather)

Diagnosis
Glycosuria, aminoaciduria, hypercitraturia, and phosphaturia
Hypokalemia
Urine ph<5.5
Bicarbonate 15-18mEq/L
Fanconi Syndrome assoc with proximal (Type 2) RTA
Causes for renal dysfunction in multiple myeloma
- Bence Jones proteinuria
- Amyloidosis of AL type, formed from free light chains (usually of λ type).
- Light-chain deposition disease - light chains (usually of κ type) deposit in GBMs and mesangium in nonfibrillar forms
- Hypercalcemia and hyperuricemia
Morphology of acute tubular necrosis
casts in tubular lumen
Flattened dilated lumina with sloughing off of apical cytoplasm

Which important complication of acute pyelonephritis is shown in the attached image?
Papillary necrosis

Mechanism of drug induced acute interstitial nephritis
Drugs act as haptens–>covalently bind to some plasma membrane /extracellular component of tubular cells –>immunogenic–> IgE or cell-mediated immune reactions directed against the tubular cells or the BM.
- Term that best describes the morphology shown in the attached image
- What is the underlying cause?
- Onion skinning seen in hyperplastic arteriolosclerosis
- Severe hypertension

What is the most likely etiology responsible for the finding shown?

Atherosclerotic Renal Disease
Radiologic finding assoc with acute pyelonephritis
CT scan with contrast - striated nephrogram

2 conditions associated with nephrosclerosis
hypertension
diabetes
How does hypertension lead to hyaline arteriolosclerosis?
Increased intraluminal arteriolar pressure–> damaged vessel wall–>leakage of plasma proteins.
Why do RBCs in the vasa recta sickle?
The low oxygen tension or relatively hypoxic, hypertonic, and acidotic environment of the inner medulla predisposes red blood cells in the vasa recta to sickle
How does diabetes mellitus lead to hyaline arteriolosclerosis?
glucose combines with proteins in the basement membrane of arterioles–>a process called nonenzymatic glycosylation (NEG) –>causes the basement membrane to leak proteins from the plasma into the vessel wall.
What will be the gross morphology of the kidney in the condition described below?
sudden onset of pain at the costovertebral angle, fever, malaise
Dysuria, frequency, urgency
Condition : Acute pyelonephritis
Gross morphology: grayish whiote focal abscesses

How do NSAIDs cause acute kidney injury?
decreased synthesis of vasodilatory prostaglandins–> ischemia.
Pre renal causes of acute kidney injury due to reduction in effective arterial blood volume
Cardiogenic shock
Sepsis
Morpholgic change in wall of blood vessels in response to hypertension
Hyaline arteriolosclerosis

List some causes for a non anion gap acidosis
a. Loss of bicarbonate from the gastrointestinal tract- diarrhea
b. Loss of bicarbonate from the kidney- proximal renal tubular acidosis
c. inappropriately low renal acid excretion - classical distal RTA [cDRTA], generalized distal RTA [type 4 RTA]
d. Progressive CKD
2 important causes for renal artery stenosis
- Atherosclerosis
- Fibromuscular dysplasia
2 main causes for acute tubular necrosis
- Ischemia
- Direct toxic injury to tubules
How does an individual contract typical HUS?
Intestinal infection by Escherichia coli strain O157:H7 through ingestion of _contaminated ground meat (_as in hamburgers)
Types of RTA
- Proximal RTA (type 2)
- Classical distal RTA (type 1)
- Hyperkalemic RTA (type 4)
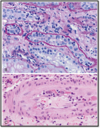
Idenitfy the morphologic feature shown in the attached image and list conditions associated with it

- Fibrinoid necrosis + concentric, laminated (“onion-skin”) thickening of the walls
- Malignant hypertension
Identify the pattern of transplant rejection whose mechanism has been described below:
preformed antibodies specific for antigens on graft endothelial cell
Occurs within hours, immediately after the graft is implanted and blood flow is restored
Hyperacute rejection
Is this pre renal acute kidney injury OR acute tubular necrosis?
BUN/ Cr ratio >20:1
Urine sodium <25mEq/L
FeNa <1%
Urine osmolality >500mOsm/kg
Favors pre-renal disease
Type of RTA described below:
urine pH <5.5
a positive urinary anion gap
Low aldosterone
Hyperkalemia
Type 4 RTA
Pre renal causes of acute kidney injury due to reduction in cardiac output because of profound vasoconstriction
NSAIDs
Hepatorenal syndrome
Severe heart failure
Deficiency of which enzyme necessary for breaking down bone within osteoclasts presents with renal tubular acidosis ?
Carbonic anhydrase II is an enzyme that generates carbonic acid from water and carbon dioxide to help create the acidic milieu necessary to break bone down within the osteoclasts.
Carbonic anhydrase II deficiency syndrome manifests as the following triad:
- Osteopetrosis
- Renal tubular acidosis
- Cerebral calcification
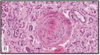
Conditions associated with the renal morphology shown

Image shows Urate nephropathy
Condition assoc is Gout
Characteristic finding of acute tubular necrosis on urinalysis
Muddy brown granular casts

What type of infarct is seen in the kidney- pale or red?
Wedge shaped pale infarcts

Identify the pattern of transplant rejection whose mechanism has been described below:
CD8+ CTLs activated by alloantigens within the graft may directly destroy graft cells, or CD4+ cells secrete cytokines and induce inflammation, which damages the graft
Within days-weeks
Acute cellular rejection
Most common cause of acute kidney injury?
Acute tubular necrosis
What pattern of pathologic calcification is assoc with nephrocalcinosis- Dystrophic/ metastatic?
Metastatic calcification
Complications of acute pyelonephritis
- Papillary necrosis
- Pyonephrosis
- Perinephric abscess
- Chronic pyelonephritis
- Septicemia with endotoxic shock
Identify the pattern of transplant rejection whose mechanism has been described below:
antibodies bind to vascular endothelium and activate complement via the classical pathway –>inflammation –> endothelial damage–>graft failure
Antiobody mediated acute rejection
Light microscopic morphology of hyperacute transplant rejection
oArteries - acute fibrinoid necrosis
oGlomeruli- thrombotic occlusion of capillaries

Type of RTA described below:
Positive UAG
Urine pH >5.5
Hypokalemia
defect in acid secretion by type A intercalated cells in the distal nephron
Classical Distal Renal Tubule Acidosis (Type 1)
Is this pre renal acute kidney injury OR acute tubular necrosis?
BUN/ Cr ratio < 15:1
Urine sodium >40mEq/L
FeNa >2%
Urine osmolality 300-350mOsm/kg
Favors acute tubular necrosis
Diagnosis?
recurrent fever, flank pain, dysuria
Gross: large, yellowish orange nodule
LM: accumulation of foamy macrophages intermingled with plasma cells, lymphocytes, polymorphonuclear leukocytes, and occasional giant cells.
Xanthogranulomatous pyelonephritis

What are some clinical clues to suspect renovascular hypertension?
Sudden-onset hypertension prior to 30 years of age or after 55 years of age.
Severe or refractory hypertension
Severe hypertension with heart failure/flash pulmonary edema
Sudden onset of worsening azotemia after the institution of an ACE inhibitor or ARB
Epigastric abdominal bruit in the setting of increased BP
Why is the medulla spared in diffuse cortical necrosis?
Vasa recta that supply arterial blood to the medulla arise from juxtamedullary efferent arterioles, proximal to vessels supplying the outer cortex. Thus, occlusion of outer cortical vessels (e.g., by vasospasm, thrombi or thrombotic microangiopathy) leads to cortical necrosis and spares the medulla.
3 thrombotic microangiopathies assoc with renal manifestations
Typical Hemolytic uremic syndrome (HUS)
Atypical Hemolytic uremic Syndrome (HUS)
Thrombotic thrombocytopenic purpura (TTP)
Gross morphology of obstruction associated chronic pyelonephritis
Diffuse scarring with thinned out cortex.

4 manifestations of sickle cell nephropathy
Renal Infarction
Hematuria
Hyposthenuria
Papillary necrosis
In which clinical scenario would you be likley to encounter the finding shown ?

Finding shown: Diffuse cortical necrosis
Clinical scenario: Any condition associated with hypovolemic or endotoxic shock
Intrinsic causes of acute kidney injury
- Acute tubular injury
- Drug induced interstitial nephritis
- Intratubular obstruction
- Glomerular diseases
- Occlusion of large renal vessles
most common cause of tubulointerstitial nephritis in the United States
Medications
List 3 conditions in which papillary necrosis is seen?
diabetics, sickle cell disease, obstructive uropathy
Recap the 3 major categories of acute kidney injury and how they are distinguished based on FeNa, BUN/Cr, UNa, UOsm, Urinalysis

key distinguishing feature between renal papillary necrosis due to diabetes versus analgesic nephropathy
DM: All of the affected papillae are at the same stage Analgesic nephropathy: several papillae are at different stages of necrosis
Why is the left kidney affected more than the right kidney in sickle cell nephropathy?
longer left renal vein is compressed between the aorta and the superior mesenteric artery —> increased venous pressure a “nutcracker phenomenon.”—> leads to increased relative hypoxia in the renal medull –> sickling.
2 drugs assoc with proximal RTA
Acetazolamide, Ifosfamide
Identify the condition described
Neurologic symptoms
Fever
Thrombocytopenia
Hemolysis –microangiopathic hemolytic anemia
Kidney Failure

Thrombotic Thrombocytopenic Purpura
List drugs causing acute drug induced interstitial nephritis
- Mnemonic: SMART CAN*
- *S**= SULFONAMIDES
- *M**=METHICILLIN
- *A**=AMPICILLIN
- *R**=RIFAMPICIN
- *T**=THIAZIDES
- *C**=CIMETIDINE
- *A**=ALLOPURINOL
- *N**=NSAIDS
Mechanism of atypical HUS
Impaired function of complement regulatory proteins - Factor H, complement Factor I and CD46 OR Autoantibodies against complement regulatory proteins
Identify the pattern of transplant rejection described below:
T cells –>react against graft alloantigens–>
cytokines–> stimulate the proliferation and activities of fibroblasts and vascular smooth muscle cells in the graft –>intimal thickening and vascular occlusion
Chronic transplant rejection
In a patient with bilateral functioning kidneys and unilateral RAS, what happens to the renin levels in the stenotic ischemic kidney?
Renin in the ischemic kidney is elevated
6 causes for renal infarction
- AFib–> Left atrial thrombus formation → systemic circulation
- Mural thrombi overlying myocardial infarcts in the LV
- Atherosclerotic emboli from the abdominal aorta or renal artery
- Thrombosis superimposed on underlying atherosclerosis
- Infected valves in bacterial endocarditis
- Sickle cell nephropathy
