HEART PATHOLOGY -2 Flashcards
Myocardium, Valvular Heart Disease, Pericardium, Neoplasms
List all possible cardiac causes responsible for this finding
Deborah Dalmeida MD

- The gross image shows a pale infarct in the kidney. The infarct could be caused secondary to an embolus. Cardiac conditions assoc with embolism include:
a. Dilated cardiomyopathy
b. Patent Foramen ovale
c. Artificial valve
d. Infective endocarditis, Non Bacterial Thrombotic endocarditis
e. Mural thrombus following an MI
f. Mitral valve prolapse, mitral annular calcification
g. Myocarditis.
Deborah Dalmeida MD
Using the clues provided, identify the valvular lesion
a sudden rise and then drop in pulse pressure
Head bobbing
murmur perceived best along the left sternal border- best heard with the patient leaning forward, after exhaling
Deborah Dalmeida MD
Aortic regurgitation
Deborah Dalmeida MD
List cardiac and vascular conditions assoc with increased risk for Infective endocarditis
Deborah Dalmeida MD
Rheumatic heart disease with valvular scarring
mitral valve prolapse
degenerative calcific valvular stenosis
bicuspid aortic valve (whether calcified or not)
artificial (prosthetic) valves
unrepaired and repaired congenital defects.
Deborah Dalmeida MD
1. What is this morphologic lesion called?
foci of T lymphocytes, occasional plasma cells, and plump activated macrophages called Anitschkow cells
2. Which condition is it seen?
Deborah Dalmeida MD

- Aschoff bodies
- Seen in acute rheumatic fever
Deborah Dalmeida MD
1. Identify the lesion
50 year old male, history of dyspnea. History of hospitalization with fever associated joint pain and subcutaneous nodules 20 years ago.
Listen to the heart sound and observe Wigger’s Diagram
2. What is the change seen in the Wigger’s diagram that clinches the diagnosis?
Deborah Dalmeida MD

- Mitral regurgitation
- Abrupt rise in left atrial pressure indicated by the tall v wave.
Deborah Dalmeida MD

List the complications of prosthetic valves
Deborah Dalmeida MD
Prosthetic valve endocarditis
Anticoagulant related hemorrhage
Thrombosis/thromboembolism
Deborah Dalmeida MD
50% to 70% of patients with this lesion provide a history of which condition?
Deborah Dalmeida MD

acute rheumatic fever
Deborah Dalmeida MD
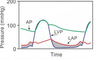
1. Identify the lesion
70 year old male, history of exertional syncope and angina.
Listen to the heart sound and observe Wigger’s Diagram
2. What is the change seen in the Wigger’s diagram that clinches the diagnosis?
Deborah Dalmeida MD

- Aortic stenosis
- Left ventricular pressure (LVP) > Left atrial pressure (LAP)
Deborah Dalmeida MD

Identify this lesion that develops following papillary muscle rupture after an MI
Deborah Dalmeida MD
Mitral regurgitation
Deborah Dalmeida MD
1. What’s the most likely cardiac tumor to be associated with this condition?
5 year old child
Physical examination reveals mutliple hypomelanotic macules
USG abdomen shows multiple renal cysts
2. What is the syndrome/disease described above?
Deborah Dalmeida MD
- Rhabdomyoma
- Tuberous sclerosis
Deborah Dalmeida MD

- What’s the etiology?
bronchospasm, flushing, diarrhea
tricuspid regurgitation
2. What are the elevated biomarkers?
Deborah Dalmeida MD
- Carcinoid heart disease due to a carcinoid tumor
- serotonin, metabolite 5-hydroxyindoleacetic acid (5HIAA)
Deborah Dalmeida MD
What pathologic pattern of cardiomyopathy best fits this description?
abnormally stiffened myocardium (because of fibrosis or an infiltrative process) leading to impaired diastolic relaxation, but systolic contractile function is typically normal or near normal
Deborah Dalmeida MD
Restrictive cardiomyopathy
Deborah Dalmeida MD
Fever
Pleuritic chest pain localized to the retrosternal area
pericardial friction rub
diffuse ST segment elevation
Deborah Dalmeida MD
Acute Pericarditis
Deborah Dalmeida MD
1. Identify the lesion
left ventricular cavity compressed into a “banana-like” configuration
Asymmetric septal hypertrophy
harsh systolic ejection murmur- heard best at the left lower sternal border, intensity increases on Valsalva
2. What is the cause of the dynamic LV outflow tract obstruction in this lesion?
Deborah Dalmeida MD

- Hypertrophic cardiomyopathy
- Asymmetric hypertrophy of the ventricular septum leading to abnormal motion of the anterior mitral valve leaflet
Deborah Dalmeida MD
1. Identify the lesion
52 year old male, history of palpitations and exertional dyspnea. History of hospitalization with fever associated joint pain and subcutaneous nodules 20 years ago.
Listen to the heart sound and observe Wigger’s Diagram
2. What is the change seen in the Wigger’s diagram that clinches the diagnosis?
Deborah Dalmeida MD
- Mitral Stenosis
- Left atrial pressure (LAP) exceeds left ventricular pressure (LVP)
Deborah Dalmeida MD

Using the clues provided, identify the valvular lesion and the most likely cause of this lesion in patients <60 years old
weakened and delayed upstroke of carotid
murmur heard best at the base of the heart but often radiates to the neck and apex
Deborah Dalmeida MD

The lesion is aortic stenosis
The cause is a congenital bicuspid aortic valve which has developed calcific deposits (look at the image carefully)
Deborah Dalmeida MD
- most frequent primary tumor of the pediatric heart
- Condition assoc with this tumor
Deborah Dalmeida MD

- Rhabdomyoma
- Tuberous sclerosis
Deborah Dalmeida MD
Causes for “culture-negative” endocarditis
Deborah Dalmeida MD
- Coxiella burnetti
- Bartonella sp
- HACEK (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella)
Deborah Dalmeida MD
1. Identify the lesion
30 year old male, history of exertional dyspnea. History of loose joints, stretchy skin, since childhood.
Listen to the heart sound and observe Wigger’s Diagram
2. What is the change seen in the Wigger’s diagram that clinches the diagnosis?
Deborah Dalmeida MD

- Aortic regurgitation
- Wide pulse pressure (Increased systolic aortic pressure and decreased aortic diastolic pressure)
Deborah Dalmeida MD

most common primary tumor of the adult heart
Deborah Dalmeida MD
Myxoma
Deborah Dalmeida MD
What pathologic pattern of cardiomyopathy best fits this description?
ventricular chamber enlargement with impaired systolic contractile function
Deborah Dalmeida MD
Dilated cardiomyopathy
Deborah Dalmeida MD
1. Using the clues provided, identify the valvular lesion and the most likely cause of this lesion in patients >70 years old
weakened and delayed upstroke of carotid
murmur heard best at the base of the heart but often radiates to the neck and apex
Deborah Dalmeida MD

The valvular lesion is aortic stenosis
The cause is degenerative
Deborah Dalmeida MD
What pathologic pattern of cardiomyopathy best fits this description?
abnormally thickened ventricular wall with abnormal diastolic relaxation but usually intact systolic function
Deborah Dalmeida MD
Hypertrophic cardiomyopathy
Deborah Dalmeida MD
List 4 possible causes for the condition seen in this image.
Deborah Dalmeida MD

- Alcohol
- Beri beri (wet)
- Coxsackie myocarditis
- Chronic cocaine use
- Chagas disease
- Doxorubicin
Deborah Dalmeida MD
jugular venous distention
systemic hypotension
pulsus paradoxus
EKG – Low voltage QRS and electrical alternans
Deborah Dalmeida MD
Cardiac tamponade
Deborah Dalmeida MD
This lesion is associated with concentric or eccentric hypertrophy?
Deborah Dalmeida MD

Aortic regurgitation- assoc with eccentric hypertrophy due to volume overload
Deborah Dalmeida MD
What is the mechanism responsible for findings seen in the attached image?
28 year old female presenting with fever, Tender, subcutaneous nodules in the pulp of the digits and hemorrhagic nontender lesions on the palms or soles
Deborah Dalmeida MD

The vignette described is of infective endocarditis. The image shows splinter hemorrhages. The mechanism responsible is microthromboemboli.
Deborah Dalmeida MD
What is the Microscopic morphology of the tumor described below?
left atrial mass
sessile or pedunculated lesions
position dependent intermittent valvular “ball-valve” obstruction
Deborah Dalmeida MD
•Microscopic features:
stellate or globular myxoma cells embedded within an abundant acid mucopolysaccharide ground substance
Peculiar vessel-like or gland-like structures
The diagnosis is atrial myxoma
Deborah Dalmeida MD
List 4 causes for restrictive cardiomyopathy
Deborah Dalmeida MD
Amyloidosis
hemochromatosis
glycogen storage disorders
endomyocardial fibrosis
Metastatic tumors
radiation
Deborah Dalmeida MD
seen in rheumatic mitral stenosis due to calcification and fibrous bridging across the valvular commissures
Deborah Dalmeida MD

“fish mouth” or “buttonhole” stenosis
Deborah Dalmeida MD
What is the complication of infective endocarditis shown in the image?
Deborah Dalmeida MD

Ring abscess
Deborah Dalmeida MD
1. Diagnosis?
most common recognized cause of restrictive cardiomyopathy in nontropical countries
Small, semitranslucent nodules resembling drips of wax may be seen on the atrial endocardial surface
•Congo red stain - characteristic apple green birefringence under polarized light
2. What is the composition of this deposit?
Deborah Dalmeida MD
- Cardiac amyloidosis
- Transthyretin
Deborah Dalmeida MD
- single or multiple vegetations
- along the line of closure of the leaflets or cusps
- not invasive and do not elicit any inflammatory reaction.
Deborah Dalmeida MD

Nonbacterial Thrombotic Endocarditis
Deborah Dalmeida MD
- asymptomatic or fatigue, dyspnea, palpitations, precordial discomfort, and fever.
- Findings in attached image
Diagnosis?
Deborah Dalmeida MD

Lymphocytic myocarditis (think of viral etiology)
Deborah Dalmeida MD
1. Identify this valvular lesion
associated with heritable disorders of connective tissue
mid systolic click
associated with heritable disorders of connective tissue – Marfan Syndrome
2. Describe the gross finding seen in this condition
Deborah Dalmeida MD

- Mitral valve prolapse
- interchordal ballooning (hooding) of the mitral leaflets
Deborah Dalmeida MD
- single most important long-term limitation for cardiac transplantation
- Microscopic feature of this lesion
Deborah Dalmeida MD

- Allograft arteriopathy
- diffusely stenosing intimal proliferation
Deborah Dalmeida MD
•history of prior radiation to left side of the chest.
fatigue, hypotension, and reflex tachycardia
jugular venous distention, hepatomegaly with ascites, and peripheral edema
Kussumaul sign +
Deborah Dalmeida MD
Constrictive pericarditis
Deborah Dalmeida MD
What is the composition of the exudate responsible for the gross appearance seen in this image?
Deborah Dalmeida MD

Fibrinous pericarditis- exudate contains plasma proteins, including fibrinogen, yielding a grossly rough, granular, dry and shaggy appearance (termed “bread and butter” pericarditis)
Deborah Dalmeida MD
The attached image is a cross section of myocardium.
What pattern of cardiomyopathy would one be likely to see in this condition - restrictive/ dilated / hypertrophic cardiomyopathy?
Deborah Dalmeida MD

Restrictive cardiomyopathy
Deborah Dalmeida MD
- What is the gross appearance of the affected valve in Carcinoid heart disease?
- Which metabolites will be elevated?
Deborah Dalmeida MD
- pearly white fibrosis of the tricuspid valve
- Serotonin, 5HIAA
Deborah Dalmeida MD
Why does the Valsalva maneuver increase the intensity of the murmur of HOCM?
Valsalva–>decreased preload to right side of the heart–>decreased LVEDV–>further approximates the interventricular septum to the mitral apparatus –>worsens outflow obstruction at systole –>increased murmur intensity
Why does the Valsalva maneuver increase the intensity of the murmur of MVP?
Valsalva–>decreased preload to right side of the heart–>decreased LVEDV–>the critical volume at which prolapse begins is reached earlier at systole –>click and murmur occur closer to the first heart sound–>intensity of mumur increases
How does sustained handgrip decrease the intensity of the murmur of aortic stenosis?
Sustained handgrip–>increased afterload –>decreased forward flow from the heart into the aorta–>decreased murmur intensity.
How does squatting increase the intensity of the murmur in mitral regurgitation?
Squatting–>rise in afterload–> movement of blood in the left ventricle across the regurgitant mitral valve–> into the left atrium rather than entering the systemic circulation across the aortic valve –> increased intensity of murmur
How does squatting decrease the intensity of the murmur of HOCM?
Squatting–> Increased preload –>Increased LV volume and stretching of LV walls –> increased distance between mitral valve leaflet and inter-ventricular septum –> decreased LV outflow obstruction –> decreased intensity of HOCM murmur
