Pathology Flashcards
What process do they arrows likely represent after a stroke?

Wallerian degeneration of cortical spinal fibers.
What are the small oval cells? What is the common stain for them?

Astrocytes: small, no cytoplasm
GFAP
What are the small cells on the very outer layer? They form the arachnoid membrane.
What do they stain with?

Meningothelial cells
Stains positive for epthelial membrane antigen (EMA)
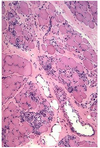
What type of cells are these? What do they produce? What do they stain with?

Choroid Plexus: Large cuboidal epithelium overlying blood vessels, connective tissue and meningothelial cells.
- Produces CSF
- Stains positive for transthyretin
What cell type is circled?
Alive or dead?
When do they appear after ischemia?

Neurons become brightly eosinophilic with loss of the Nisl substance within 6-24 hours of ischemia (“Red neurons”).
What are these cells? What would they stain + for?
When do they appear after ischemia?

Reactive astrocytes. GFAP, as always :)
12-36 hours
What are these cells? When do they invade after a stroke?

Polymorphonuclear cells invade the ischemic territory within hours and peak at 48-72 hours.
When does vascular proliferation occur after a stroke?
What imaging correlate does it have?
After 48 hrs. Should allow for some contrast enhancement due to BBB breakdown.
What is caused the area in the circle? What is the finding the arrow is pointing to?

Cystic cavity surrounded by gliotic tissue with glial strands (circle)
– There is compensatory (ex-vacuo) ventricular enlargement
What type of stroke caused this? What is the underlying vascular problem identified on pathology?

Lacunar infarction
• Infarctions ranging in size from 1 mm to 1.5 cm (arrow)
• Classically, the walls of small arteries become thickened from the formation of hyalinemembranes (lipohyalinosis) (circle)
– Caused by chronic hypertension
- These arteries may also rupture and cause hemorrhage
Old guy found down and brought back to life. Died of inability to feed himself. What was the cause?

Watershed infarction. Couldn’t eat due to man in a barrel like weakness and couldn’t get food to his mouth. So sad.

What cells are killed of by transient global hypoperfusion?
Transient shock or cardiopulmonary arrest causes focal ischemic injury to neurons with high metabolic rates:
– Layer 3 and 5 of cortex
– Hippocampus
– Purkinje cells
What is this pathology? What is the black stain?

Tearing of the endothelial lining of the blood vessel with extravasation of blood
into the vessel wall
Seen in:
– Marfan’s syndrome
– Fibromuscular dysplasia,
– Ehlers-Danlos type IV
– Trauma
I believe that is reticulin staining.
What is this process? How can you differentiate it from viral encephalitis?

Vasculitis
• May be part of a systemic vasculitis or isolated to the CNS.
• Requires transmural vessel wall inflammation
17 year old out parting at Elich’s and then got gastro and is overweight on OCPs. Presents with seizure then rapid decline.
Wa happened?

Venous Sinus Thrombosis
• Venous congestion over the convexities with parietal petechial hemorrhages.
Associated with:
– Post-partum
– Dehydration
– Hypercoagulable states
– Adjacent inflammation
(e.g., mastoiditis).
15 year old presents with first seizure. What is the cause of this pathology? Is there normal tissue?

AVM
Located in cortex
Composed of both large arteries (open arrow) and veins (solid arrow) without
intervening capillaries.
Between vessels there is gliotic nonfunctional hemosiderin stained tissue (circle).
10 year old shows up after seizure and has an MRI with popcorn lesions.

Cavernous Malformation
Located in cortex or less frequently in the brainstem.
• Composed of thinwalled vessels (arrow).
• There is no intervening parenchyma between the vessels (circle).
Name the common vascular malformations, if they have arterial flow, what the vessels in the malformation are, if there is a draining vein, and if the intermixed brain tissue is normal.

What are the most common locations for hypertensive hemorrhages in order of frequency?
Hypertensive Hemorrhage
• Commonly occur in the:
– Putamen (65%)
– Pons (10%)
– Cerebellum (10%)
– Thalamus
• These are the same locations of lacunar infarctions.

What study should be ordered on a patient with a similar presentation (before autopsy)?

Angiography.
Subarachnoid Hemorrhage
• Caused by aneurysmal rupture ortrauma
• Overlying the blood is the arachnoid membrane (arrow).
What was the mechanism of injury for this patient?

Area of hemorrhagic necrosis from cerebral contusion.
– Usually affects the crest of gyri.
– Frequently seen in subfrontal and anterior temporal lobes as the base of the brain slides over the irregular skull base
• Blood is removed by macrophages leaving an irregular tan discoloration.
What is the mechanism of the injury seen here?

Diffuse Axonal Injury
• Widespread ruptured axons from trauma.
– Neuroimaging is normal but patients are comatose, may see microhemorrhages in white matter tracts.
- On gross examination, there is white matter atrophy.
- The injured axons dilate (“axon retraction balls”)
Name the herniation and vessel at risk.

Subfalcine: an edematous cingulate gyrus (arrow) compresses the ipsilateral anterior
cerebral artery as it runs in the falx cerebri.
Name the herniation and vessel at risk

Uncal Herniation
• The medial temporal lobe (uncus) herniates across the tentorium cerebelli compressing:
– the ipsilateral 3rd nerve
– the midbrain resulting in compression of the contralateral cerebral peduncle on Kernohan’s notch
– the posterior cerebral arteries resulting in occipital lobe infarcts.