what does injury to the mamillary bodies cause?
psychosis, memory deficits and confabulation.
what does injury to bilateral amygdala cause?
hypersexuality, hyperorality and hyperphagia (kluver-Bucy)
injury to what part of the thalamus can cause language deficits?
medial thalamus
injury to what part of the thalamus can cause problems with sleep-wake cycle?
anterior and medial thalamus
what are AAN recommendations for initial workup of dementia/
B12, CBC, CMP, Thyroid function, depression screening.
what makes up the circuit of papez?
entorhinal cortex–>hippocampus–>fornix–>mamillary bodies–>anterior nuc of thal–> cingulate gyrus
What chromosome is Presenilin-1 on? What percentage of familial AD is associated with this gene?
14, 80%
what chromosome is Presenillin 2 on? What percentage of familial AD is associated with this gene?
1, 5%
what chromosome is Apolipoprotein E4 on? What percentage of familial AD is associated with this gene?
- None Triples risk of AD as a modifier but does not cause AD per se.
what chromosome is Amyloid precursor protein (APP) on?
21
what are common early features of AD?
deficits in recent memory, visuospatial skills, verbal dysfluency, anomia.
in what regions is PET hypometabolism in diffuse lewy body disease?
occipital regions
what are the 3 cardinal aspects of diffuse lewy body disease? What are three additional common features?
Parkinsonism, fluctuating cognition, visual hallucinations. Also can have dysautonomia, neuroleptic sensitivity, sleep disorder.
which class of medications should be avoided in diffuse lewy body disease?
typical neuroleptics.
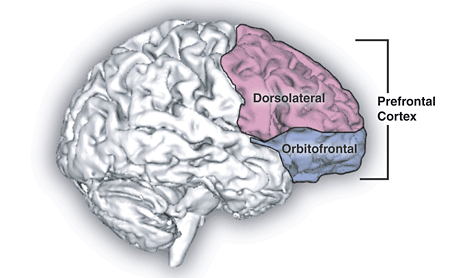
Lesion to what area causes personality change, perseveration, apathy and depression?
dorsolateral frontal lobe
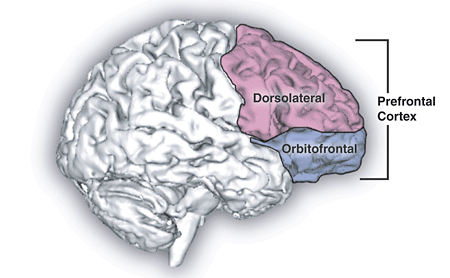
lesion to what area causes OCD traits, disinhibition, hypersexuality, impulsiveness and anti-social behavior?
orbitofrontal lobe
lesion to what area causes psychosis and memory disturbance?
temporal lobe
what chromosomal locus is the most commonly associated with familial FTD? what gene?
17q21, progranulin
in what age range is the mean onset of FTD?
55-60
what are the three main variants of FTD?
- Behavioral- Primarily right frontal degeneration 2. progressive nonfluent aphasia- anomia, word finding difficulty, object naming deficits, effortful speech with impaired comprehension. primarily left insula degeneration 3. semantic Dementia - normal fluency but with semantic paraphasias, anomia and impaired comprehension. unilateral or bilateral temporal lobe.
where is hypometabolism on PET in FTD
Frontal and anterior temporal regions.
what are typical deficits in lesions of dominant temporal lobe?
amnesia for verbal information, wernike’s aphasia
what are typical deficits in lesions of non-dominant temporal lobe?
amnesia for non-verbal and temporal-spatial info, amusia.
what is the role of the circuit of papez?
memory formation











-
Neuro Anatomy16
-
Fvbxxd2
-
movement disorders84
-
basic neuroscience7
-
Neuromuscular260
-
cranial nerves and brainstem19
-
behavior and memory95
-
cranial nerves and neuro ophthalmology72
-
vascular neurology59
-
neurocritical care48
-
Headache21
-
Epilepsy and Sleep100
-
psychiatry81
-
neuroimmunology11
-
neuro oncology71
-
infections29
-
neurology of systemic dz24
-
nutritional and toxic disorders29
-
Child Neuro99
-
Pathology111
-
Radiology16
