Molavi Chapter 27 - Brain and Meninges Flashcards
(16 cards)

Normal white and gray matter
The white matter (left) has a coarser texture and is dotted by astrocytes cells with scant cytoplasm and oligodendrocytes with a halo (from washed-away myelin).
The gray matter right) has a finer background texture and is made up of neuropil with interspersed large neuron cell bodies.

The normal cerebellum
Multiple layers are visible: The spindly arachnoid mater, a layer of white matter (the “molecular layer”), a thin layer of Purkinje neuron bodies, and a grainy granule cell layer.

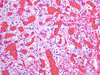
Cerebral infarct
Sheets of histiocytes or macrophages with round contours and bubbly cytoplasm.
Indicates either an infarct or a demyelinating lesion. Hemorrhage suggests infarct.

Reactive astrocytosis
Activated astrocytes are seen here. Rather than having a near-invisible layer of cytoplasm, they expand to have a large, stubby, dense layer of pink cytoplasm.
Astrocytic lesion WHO grading
WHO grade 1 astrocyte lesion: Pilocytic astrocytoma
WHO grade 2 astrocyte lesion: Diffuse astrocytoma
WHO grade 3 astrocyte lesison: Anaplastic astrocytotma
WWHO grade 4 astrocyte lesion: Glioblastoma

Pilocytic astrocytoma
Usually occurs in the posterior lobes of children and adolescents.
A circumscribed, very indolent form of astrocytoma. The “pilo” comes from the hair-like fine processes in the background of this tumor.
Rosenthal fibers and eosinophilic granular bodies (both bright eosinophilic astrocytes processes, better seen below) are often seen, hallmarks of slow-growing astrocyte tumors.


Oligodendroglioma
Usually occurs in frontal/temporal lobes of adults.
A diffuse-type lesion. On histology it looks like a discohesive collection of normal oligodendroglia with small, round nuclei surrounded by clear halos (retraction artifact seen only in formalin-fixed tissues). The chromatin is clumpy, like a plasma cell, but overall is uniform.
Architecturally, they like to cluster around existing neurons. A net-like capillary array (chicken-wire capillaries, like in myxoid liposarcoma) is often present. Microcystic pattern and calcifications may be present.

Meningioma
Can vary widely in appearance, but this one is classic. Arises from arachnoid-type cells associated with the dura mater, and is therefore almost always dural based.
Classic meningiothelial cells occurr in syncytium with its neighbors, Meningiomas of all types have whorls, and when these whorls necrose they may form Psammoma bodies. Grade 2 meningiomas may become glycogen-filled and take on a clear-cell morphology, or may grow on a myxoid background.

Solitary fibrous tumor / Hemangiopericytoma
Another type of dural-based, enhancing, well-circumscribed tumor.
Histologically characterized by a blue, cellular tumor with prominent stereotypical gaping vessels called “staghorn” vessels.
Hemangioblastoma
An uncommon, highly vascular CNS tumor that typically occurs in the posterior fossa. Typically seen in von Hippel-Lindau syndrome.
Unfortunately, the tumor looks a lot like renal cell carcinoma with its packets of lipidized clear tumor cells and vast, delicate capillary network.
Also, VHL patients are at increased risk for RCC too! So who’s to say it’s not metastasized RCC? For this reason an oil red O stain (fat stain performed only on frozen sections) and immunostains are often necessary to differentiate the two.

Schwannoma
Note the classic alternating Antoni A (high cellularity) and Antoni B (low cellularity with white background) areas. Most often seen as an acoustic neuroma in the CNS.
Tends to make little palisaded arrays called “Verocay bodies” (arrow). Hyralinized, thick, pink vessels are common.


Craniopharyngioma
“Adamantinomatous” appearance (looks like a developing tooth!). Nests of cells are bounded by dark, palisaded cells with central areas of stellate cells in a myxoid stroma. There are also keratin debris (“wet keratin”).
When seen in adults, they area more often the papillary-type, resembling a non-keratinizing squamous cell carcinoma.

Ependymoma
Arises from the ventricle-lining ependymal cells. Hence, when neoplastic, they tend to encircle and obstruct ventricles.
Histologically is a circumscribed lesion with pale, oval nuclei that align themselves around vessels and send down processes like “spokes on a wheel.” This is called a pseudorosette (shown). When they make an array around a tiny open lumen (not a vessel), this is a true rosette.

Medulloblastoma
Characterized by sheets of small blue cells with high N/C ratio, high mitotic rate, and necrosis. There are frequent apoptoses (arrowhead) and mitotic figures (arrow). Chromatin is very fine in texture, like a neuroendocrine cell.
Nuclei tend to be in a wedge or carrot shape, especially when molded into rosettes.
Stains for glial lineage
GFAP (cytoplasmic) and Olig-2 (nuclear)
IDH
Isocitrate dehydrogenase
Often mutated in glioblastoma and is a poor prognostic factor (classified as IDH WT vs IDH mutant).
Oncogene. The mutated protein produced 2-hydroxybutyrate, an epigenetic modifier.
