Case studies and Quiz Flashcards
(67 cards)
How do you make a haematological diagnosis?
Clinical history and exam
Imaging
Cytogenetics
Molecular genetics
Immunophenotyping
Chromosomal Analysis
A 5-year-old boy of Indian ethnic origin presented with lymphadenopathy and a mediastinal mass on chest radiology
WBC 180 × 109/l, Hb 93 g/l and platelet count 43 × 109/l. Blood film shows blast cells.
Think about
What is the most likely diagnosis?
What is the mediastinal mass?
ALL
Mediastinal Mass = Thymoma
Why does a mediastinal mass occur?
The very high WBC (180 × 109/l) in a child means a diagnosis of leukaemia is almost certain
The low Hb (93 g/l) and platelet count (43 × 109/l) are the result of bone marrow infiltration
The mediastinal mass is the thymus, which is infiltrated by T lymphoblasts
What would be the best technique to confirm the diagnosis of ALL?
1 Immunophenotyping
2 Cytochemistry
Immunophenotyping
48-year-old male – railway engineer
2-week history bleeding gums
Attended dentist - severe bleeding
1 episode of haematuria
Minor bruising
Attended Accident and Emergency department
Left subconjunctival haemorrhage
Small bruises over abdomen
No enlarged lymph nodes
No hepatosplenomegaly
What test is most likely to reveal the cause of the problem?
Liver function tests
Creatinine
Coagulation screen
Blood count, film and coagulation screen
Blood count, film and coagulation screen
Normal Renal function
Minor liver derangement (longstanding)
Alanine transaminase 97 iu/l (0‒37)
Alkaline phosphatase 72 iu/l (30‒130)
Bilirubin 24 μmol/l (0‒17)
FBC
WBC 7.5 × 109/l (4.0‒11)
Hb 109 g/l (130‒170)
MCV 83 fl (83‒01)
Platelets 21 × 109/l (120‒400)
Coagulation screen
PT 13.4 s (9.6‒1.6)
APTT 21.5 s (24‒32)
Fibrinogen 0.97 g/l (1.8‒3.6)
How could you explain a SHORT APTT and a low fibrinogen?
What other test do you need?
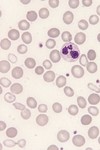
Blood Film
Do you think these are myeloid cells or lymphoid?
How would you prove it?

- Granules strongly suggest myeloid
- Proof
–Cytochemistry
–Immunophenotyping
–But note that neither test is actually necessary
Which diagnosis do you suspect?
- Chronic myeloid leukaemia
- Acute promyelocytic leukaemia
- Some other type of acute myeloid leukaemia
- Acute lymphoblastic leukaemia
Acute promyelocytic leukaemia
Which of the following tests would be most useful to confirm the diagnosis of APML?
1Cytochemistry
2Immunophenotyping
3Cytogenetic analysis/FISH/molecular genetic analysis
Cytogenetic analysis etc
- A 68-year-old retired secretary
- Gradual onset of fatigue, lethargy and exertional dyspnoea
- Non-smoker, not much alcohol, good diet
- On examination
–Pallor (conjunctival and nail bed)
–Mild ankle oedema
•What one test would you do next?
FBC
- WBC 4.7 × 109/l (3.7–9.5)
- Hb 76 g/l (115–150)
- MCV 110 fl 82–98 fl
- Neutrophil count 1.4 × 109/l (NR 1.7–6.1)
- Platelet count 182 × 109/l (NR 145–350)
- Which test should be done next?
1Blood film
2Bone marrow aspirate
3Liver function tests
4Thyroid function tests
5Serum vitamin B12 and red cell folate
Blood Film
•Her blood film looked like this, what is it?
•There were macrocytes but no oval macrocytes or hypersegmentation of neutrophils
- Serum vitamin B12 — normal
- Red cell folate — normal
- Liver function tests — normal
- Thyroid function tests — normal
- Ferritin — 875 μg/l (normal range 20–200)
- What do you suspect and what would you do next?
- Bone marrow aspirate
- 12% blast cells (normal < 5%)
- 45% of erythroblasts were ring sideroblasts
DIAGNOSIS: myelodysplastic syndrome (MDS) (MDS with excess of blasts)
- Initially the patient tolerated the anaemia and required no treatment
- Later she needed red cell transfusion
- Later still she needed platelet transfusions
- Predicted survival was 1.1 years
- However, she was still alive 7 years later
The ferritin was 875 μg/l (NR 20–200) Why?
Does it matter?
1Yes
2No
3Probably not
Probably not
- A 72-year-old Indian woman
- Vegetarian, teetotal, non-smoker
- Shortness of breath on exertion
- Fatigue
- Painful gums and tongue
- Unable to eat spicy food
- On examination: pallor only
- WBC normal
- Hb 52 g/l
- MCV 122 fl
Platelet count normal
What is the most important test
1 Vitamin B12 and folate assays
2Liver function tests
3Thyroid function tests
4Bone marrow aspirate
Blood alcohol level

Vitamin B12 and folate assays
- Vitamin B12 180 ng/l (NR 125‒600)
- Red cell folate 227 pg/l (NR 215‒650)
- Thyroid function normal
- Liver function tests mildly impaired (bilirubin 20 μm/l, AST 110 iu/l (NR 40‒135)
- Lactate dehydrogenase (LDH) 3870 iu/l (NR 50‒450)
- What would you do next?
Bone Marrow Aspirate and look for giant metamyelocyte and megaloblasts

Do you think the patient has a myelodysplastic syndrome?
1 Yes
2 No
No
- Parietal cell antibodies: positive
- Intrinsic factor antibodies: positive
- Schilling test: 0% excretion
- The patient turned out to be a vegan
- You should now know the correct diagnosis and be able to explain how you would treat the patient
•The patient turned out to be a vegan
- A 70-year-old woman was referred to a vascular surgeon because of gangrenous toes
- They looked a bit like this
- History
–Not diabetic
–Had smoked 20‒30 cigarettes a day since age of 18 years
–Breathless on exertion and morning cough
•Examination
–Reduced femoral and distal pulses on side of affected toes
–Not breathless at rest, no cyanosis
–Plethora, conjunctival suffusion
–Spleen not felt
•What simple tests would you do first?

- Blood gases were normal
- Blood count was not
–WBC 18.6 × 109/l
–Hb 180 g/l
–Platelet count 1648 × 109/l
•Ultrasound examination of the abdomen showed normal kidneys and increased splenic size
The most likely diagnosis is
1Chronic myeloid leukaemia
2Essential thrombocythaemia
3Polycythaemia vera
4Chronic obstructive pulmonary disease
Polycythaemia vera
What test would you do next to try to confirm the diagnosis?
1Molecular analysis for JAK2 mutation
2Measure total volume of red cells in circulation
3Bone marrow aspirate and trephine biopsy
?
You now know the diagnosis. How would you treat the patient?
1Venesection alone
2Imatinib
3Venesection plus hydroxycarbamide
432P
Venesection plus hydroxycarbamide
•Why is phlebotomy unsuitable as the only treatment for this patient?
?
What is abnormal?

- Percentages of white cells are meaningless unless you use them to produce an absolute count
- What are the two possible explanations of
Neutrophils 1%
Lymphocytes 99%?












