Lower Limb Radiology Flashcards
Label

- 1a: ala
- 1b: foraminae
- 2: sacroiliac joint
- 3a: iliac crest
- 3b: ASIS
- 3c: AIIS
- 4a: ischial spine
- 4b: ischial tuberosity
- 5a: pubic body
- 5b: superior pubic ramus
- 5c: inferior pubic ramus
- 5d: pubic symphysis
Label

- 1a) head of femur
- 1b) neck of femur
- 1c) greater trochanter
- 1d) lesser trochanter
- 1e) femoral shaft
- 2) acetabulum
- 3) superior pubic ramus
- 4) inferior pubic ramus
- 5) ischial spine
Label

- 1a) head of femur
- 1b) neck of femur
- 1c) greater trochanter
- 1d) lesser trochanter
- 1e) proximal femoral shaft
- 2) acetabulum
- 3) ischial tuberosity
Label

- 1a) distal femoral shaft
- 1b) lateral femoral condyle
- 1c) medial femoral condyle
- 2a) proximal shaft of tibia
- 2b) intercondylar eminence of tibia
- 2c) lateral tibial plateau
- 2d) medial tibial plateau
- 3) patella
- 4a) head of fibula
- 4b) proximal shaft of fibula
Label

- 1) patella
- 2) femur
- 3) tibia
- 4) fibula
- 5) patella tendon
- 6) quadriceps tendon
- 7) suprapatellar pouch
Label

- 1a) distal tibial shaft
- 1b) plafond
- 1c) medial malleolus
- 2a) distal fibular shaft
- 2b) lateral malleolus
- 3) talus
Label

- 1) posterior malleolus
- 2) fibula
- 3) talar dome
- 4) calcaneum
- 5) navicular
An 81 year old woman fell in her garden, and has pain in her right groin. Her right leg does not appear shortened or externally rotated. Her X-ray is shown.
What can you see?
What is meant by the ‘pubic ring’ and why is this important?

- Fracture of superior and inferior pubic rami
- White sclerotic line present –> broken ends of bone are impacted up against each other
- Mass in centre –> faeces is sigmoid colon surruounded by gas (dark grey surrounding area)
- Pubic ring –> strong protective ring, but when one part of it breaks, another part is likely to have broken

A 30 year old man was thrown from his motorbike at speed. His X-ray is shown.
- What injury is demonstrated?
- How does it normally occur?
- What potential injuries could this person have?

- Open book fracture –> separation at the pubic symphysis joint
- Left side of pelvis moving up relative to right side which can move down –> vertical shear fracture
- Potential for injury to vessels and nerves, pelvic organs (e.g. urethral rupture)

A 78 year old woman fell in her home. She could not get up again due to pain in her right groin. An ambulance was called.
- What can you see?
- What do you think has happened?
- Do you need an X-ray? Justify your answer!

- Fractured neck of femur
- Right leg is externally rotated and short (hallmark features)
- X-ray shows fracture
- No impaction (more grey than white)

An 48 year old man presented to the ED with 3-day history of left hip pain after falling in the shower. He was struggling to walk. On examination his left leg was a little shorter than the right and slightly laterally rotated.
What action would you take? Justify your course of action / investigation / management!
- Where is the fracture and why does it not have the normal appearance of a fracture (a black line)?
- Why is the lesser trochanter more visible on the left than on the right?

- X-ray patient
- Due to young age of patient, is there underlying bone condition?
- Fracture of left neck of femur
- Impacted type of fracture –> abnormally white line
-
Lesser trochanter is more visible than usual on the left
- Due to external rotation of the femur

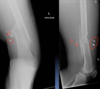
What do you make of the X-rays? How would you describe the injury? What do think the mechanism of injury was? Any concerns about other structures that could potentially be injured? What would you do next?

- Gunshot
- Comminuted fracture of femur
- Danger to popliteal and femoral vessels lying posteriorly
- Assess perfusion of leg and potential CT
A mother brought her six-week old daughter to the ED. The child had become very irritable after the mother had accidentally twisted the infant’s right leg whilst changing her nappy.
The child was irritable and became distressed when her right leg was examined.
- Take an xray!
- After xray, what action would you take now?

- Could child have disorder that means they are prone to breaks e.g. osteogenesis imperfecta
- Non accidental injury?
-
Spiral fracture of the shaft of the femur
- Tend to occur due to twisting movement
- Spiral fractures in infants that are not weight-bearing are suspicious
- Immediately involve someone more senior (do not go back to the parents)
What abnormalities can you see in the X-ray of this child’s lower limb bones?
Can you explain the abnormal appearance?

- Bowing of the femurs
- Signs of previous/old fractures
- Abnormal stripy lines –> ‘zebra stripes’
- Typically seen in osteogenesis imperfecta

A 70 year old woman presented to her GP with a long history of pain in her left knee that was becoming worse and limiting her movement.
On examination the patient had a good range of movement, but there was some discomfort in her left knee on movement and crepitus (crunchy noise and feeling when moving joint).
- The patient’s X-ray is shown. What can you see? What is the diagnosis?

- Osteoarthritis
- When looking at AP; joint space looks ok
- When looking at lateral view; joint space between posterior part of patella and anterior femur has disappeared
- Can see osteophytes

This 75 year old woman presented with difficulty walking and knee pain. How would you describe these X-rays?

- Very severe presentation of osteoarthritis
- Joint space almost completely disappeared
- Between tibia and femur
- Between femur and patella
- Huge osteophytes
- Joint space almost completely disappeared

A 30 year old man presented to the ED with left knee pain after a cycling accident.
On examination there was no deformity, but it was painful for him to weight-bear. Movements of his knee were painful, and this limited his movements.
- X-ray the patient

- AP normal
- In lateral; lipohemarthrosis
- White beneath horizontal line and grey above it
What is a lipohemarthrosis?

Results from an intra-articular fracture with escape of fat and blood from the bone marrow into the joint, and is most frequently seen in the knee.
- A long horizontal line is seen in the suprapatellar pouch
- Above line: fat
- Below line: blood
- Fracture is inside joint

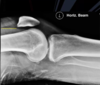
What normal variant can be seen in this image?

- Bipartite patella
- A congenital condition that occurs when the patella is made of two bones instead of a single bone

A 25 year old man presented to the ED with right ankle pain after a fall.
He was struggling to walk. His ankle was swollen and tender on examination. Movement was limited due to pain.
What can you see? What injuries are present?

- Oblique fracture of the distal fibula
- Large distance between talus and medial malleolus
- Talar shift
- Likely to injure deltoid ligament

A 30 year old woman presented to the ED with right ankle pain after a fall. She was struggling to walk. Her ankle was swollen and tender on examination. Movement was limited due to pain.
- What can you see on these X-rays?
- After looking at these X-rays, the doctor managing the patient re-examined the patient, concentrating on the lateral aspect of the leg, and then requested an AP and lateral fibula.
- Why would the doctor do this?

- Talar shift
- Disruption of ligaments –> this is a serious ankle injury
- Doctor requested an AP and lateral fibula
- (view next slide)
- Need to look further up the fibula after excessive external rotation of the ankle

AP and lateral fibula:
- What can you see on this X-ray?
- What is the name for this type of fracture?
- Why does it happen?

- Oblique fracture through the proximal fibula
-
Maisonneuve fracture
-
Comination of an unstable ankle injury with a fracture of the proximal fibula
- Due to rotational forces on the ankle that first disrupt the deltoid ligament, then injure the interosseous membrane, then fracture the proximal fibula
-
Comination of an unstable ankle injury with a fracture of the proximal fibula
-
Maisonneuve fracture
What is a maisonneuve fracture?
A combination of a fracture of the proximal fibula together with an unstable ankle injury (widening of the ankle mortise on x-ray)
