Definition of epilepsy
Recurrent unprovoked seizures
A 21 year old woman comes to see you who had her 1st seizure the morning after drinking with her friends. He roommate heard her shaking, she bit her tongue and had urinary incontinence. Labs, CT, MRI and EEG were all normal. When should you start this patient on medication?
It is a general rule that you don’t give meds to a seizure patient after their 1st seizure with a normal MRI and EEG. This is because patients have a 50/50 chance of having another seizure after their 1st seizure. You would start her on meds if she came back with a second seizure.
A patient presents to the ED with their 1st seizure ever. His MRI is shown below. EEG shows 3Hz spike wave discharges. What does the EEG tell you?
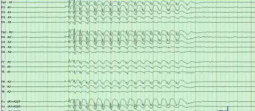
This patient has inter-ictal waves and has a high risk of seizing again.
A 21 year old woman comes to see you who had her 2nd seizure ever the morning after drinking with her friends. He roommate heard her shaking, she bit her tongue and had urinary incontinence. How do you determine what type of medication to give her?
1) Identify the epilepsy syndrome: all meds work for focal epilepsy, avoid phenytoin and carbamazepine for generalized epilepsy. 2) Tailor the medication according to side effects: levatoracitam = not for use in patients with psychiatric issues. 3) Tailor medication according to other medical conditoins: no drug interactions.
A 21 year old woman comes to see you who had her 1st seizure the morning after drinking with her friends. He roommate heard her shaking, she bit her tongue and had urinary incontinence. Her EEG showed 4-5 Hz spike-wave discharges. You start her on levetiracetam. She calls two weeks later complaining of severe anxiety and irrability while still on the low dose. What do you tell her?
Ask her to stick it out for a month to see if the side effects terminate. However, if she has an allergic reaction or suicidality you need to stop immediately.
What determines if a patient has refractory epilepsy?
Failure to respond to 2nd medication. Note that 50% of patients respond to the 1st medication and 14% respond to the second medication.
What is the prognosis for pregnant women who receive medication for epilepsy?
1/3 unchanged 1/3 improve 1/3 worsen
Teratogenic effects of antiseizure drugs. What drugs are the worst?
1.1% risk of major malformations. Valproic acid (lowers child’s IQ), topiramate & phenobarbital all carry the highest risk.
What drugs have the best safety profile for pregnancy?
Lamotrigine, levetiracetam, carbamazepine, phenytoin and oxcarbazepine. You also want to make sure she is only on one medication and on the lowest effective dose.
Is breastfeeding okay with AEDs?
Yes, the child has already been exposed.
Most common cause of seizure in elderly?
Stroke
Best drugs to use in elderly patients to manage seizures
Low drug interaction drugs: levetiracetam, gabapentin. Use low doses due to decreased drug metabolism.
Best therapy for focal temporal lobe refractory epilepsy.
Epilepsy surgery. Seizure focus is identified and removed. This is especially effective for refractory temporal lobe epilepsy.
Sequelae for epilepsy surgery.
Memory deficit and visual field defects. Note that patients must also stay on their AEDs for 2 years after surgery.
Best therapy for generalized refractory epilepsy or patients who are not candidates for epilepsy surgery.
RNS. It detects and stops seizures.
Older therapy for generalized refractory epilepsy or patients who are not candidates for epilepsy surgery.
Vagal nerve stimulation. Stimulates vagal afferents ever 30 seconds.
Lifestyle management of seizures in children with severe epilepsy syndromes and developmental delay.
Ketogenic diet, 4:1 ratio of fat to protein/carbs in diet. Note that this works just as well as antiepileptic drugs.
When can patients stop AEDs?
No seizures for 2 years, normal MRI and normal EEG.
Common comorbidity with epilepsy?
Depression (30%).
-
Psychiatry-Psychotherapy20
-
Neuro II - First Aid112
-
Psychiatry-Sex & Gender21
-
Psychiatry-Suicide & Violence11
-
Psychiatry-Dissociative Disorders6
-
Histology-Eye32
-
Anatomy-Ear48
-
Physiology-Auditory System29
-
Physiology-Vestibular System22
-
ICS-Dizziness15
-
Anatomy-Orbit35
-
Physiology-Optics19
-
Physiology-Visual Pathways22
-
Physiology-Visual Physiology19
-
Anatomy-Eye Movements35
-
Anatomy-Cerebellum28
-
ICS-Multiple Sclerosis15
-
Biochemistry-O2 Toxicity21
-
Anatomy-Face24
-
Anatomy-Infratemporal Fossa24
-
Anatomy-Facial & Trigeminal Nerves28
-
Physiology-Cranial Nerve Deficits14
-
Psychiatry-Interventional Psychiatry7
-
ICS-Headache24
-
Pharmacology-Migraine Therapy11
-
Pharmacology-Anti-Epileptic Drugs39
-
ICS-Epilepsy19
-
ICS-Neurologic Exam17
-
Anatomy-Nasal Cavity & Sinuses21
-
Microbiology-Eye, Ear & Sinus Infections29
-
Pathology-Eye w:some Nose & Ear67
-
Biochemistry-Brain Metabolism Disorders20
-
Pathology Lab-Eyes, Ears & PNS29
-
Anatomy-Upper Brainstem30
-
Anatomy-Basal Ganglia25
-
Anatomy-Dorsal Thalamus30
-
ICS-Movement Disorders22
-
Pharmacology-Neurodegeneration21
-
Pharmacology-Antipsychotics21
-
Psychiatry-Schizophrenia20
-
Anatomy-Hypothalamus18
-
Anatomy-Olfatory & Limbic22
-
Cytology-Cortex17
-
Psychiatry-Neuropsychiatry17
-
Physiology-Aphasia, Agnosia20
-
Psychology-Stress15
-
ICS-Dementia13
-
ICS-Delirium20
-
Epidemiology-Randomized Control24
-
Physiology-Placebo5
-
Imaging30
-
Psychiatry-ADHD21
-
Pharmacology-Stimulants14
-
Microbiology-Prions and Viral CNS Infections16
-
Pathology Lab-Demyelinating CNS20
-
ICS-TBI26
