Chapter 8: Physical and Chemical Injuries Flashcards
what is associated with pressure, irritation, or sucking trauma, is present in 10% of the population, and is a single white line on the occlusal plane of the buccal mucosa?
linea alba
is linea alba typical unilateral or bilateral?
bilateral
what is the treatment for linea alba?
no biopsy or treatment is necessary
___ is the scientific name for cheek chewing
morsicatio buccarum
what are the scientific names for labial mucosa chewing and tongue chewing?
- morsicatio laborium
- morsicatio linguarum
there is a higher prevalence of morsicatio buccarum in those under ___ or with ___
under stress or with psychologic conditions
morsicatio buccarum is typically found where?
bilaterally on the anterior buccal mucosa
how does morsicatio buccarum appear clinically?
thickened, shredded white areas which may be ulcerated
what is the treatment for morsicatio buccarum?
no treatment is required; not a premalignant condition
___ is the result of acute or chronic trauma that can cause surface ulcerations
traumatic ulcerations
where are the most common oral locations of traumatic ulcerations? what is the injury due to?
- lips, tongue, and buccal mucosa
- injured from dentition
___ appears as areas of erythema surrounding a central removable, yellow fibrinopurulent membrane
traumatic ulcerations
___ can develop immediately adjacent to an oral traumatic ulceration
a rolled white border of hyperkeratosis
the unique form of chronic traumatic ulceration is termed ___ or ___
eosinophilic ulceration or TUGSE (traumatic ulcerative granuloma with stromal eosinophilia)
describe TUGSE and its treatment
- traumatic ulcerative granuloma with stromal eosinophilia
- exhibits a deep pseudoinvasive inflammatory process and is slow to resolve
- incisional biopsy is usually curative
___ are chronic ulcerations found under the tongue in infants due to trauma from nursing
riga-fede disease (a form of traumatic ulcerations)
what is the treatment for traumatic ulcerations?
- remove source of injury if possible
- medications for pain releif - topical analgesics
- biopsy is warranted in cases that do not resolve after 2-4 weeks
5% of all burn admissions to hospitals are from what?
electrical burns to the oral cavity
what are the two types of electrical burns?
contact and arc
what is required for contact burns?
a good ground and must involve electrical current passing through the body from the point of contact to the ground site
what can electric current cause?
cardiopulmonary arrest and it can be fatal
most electrical burns affecting the oral cavity are what type?
arc
in arc electrical burns of the oral cavity, ___ acts as a conducting medium and an electrical arc flows between the electrical source and the mouth
saliva
most cases of oral electrical burns are a result of what?
chewing on the female end of an extension cord or biting a live wire
most electrical burns occur in what age patient? what area is affected?
kids younger than 5 and affect the lip
what is the clinical presentation of oral electrical burns?
- appears as a painless, charred, yellow area that doesn’t bleed
- edema develops within a few hours
- on the 4th day, the area becomes necrotic and begins to slough (may bleed profusely)
most thermal burns of the oral cavity arise from what?
the ingestion of hot foods or beverages
describe the location and clinical appearance of thermal burns
- typically appear on the palate or posterior buccal mucosa as zones of erythema and ulceration
some patients hold medications within their mouths rather than swallow them, which can be caustic. what type of injury does this describe?
chemical injury
what are common medications that can cause chemical injuries in the oral cavity?
- aspirin
- bisphosphonates
- two psychoactive drugs - chlorpromazine and promazine
other than medications, what are some other things that cause mucosal necrosis (chemical injury) by patient or dentist misuse?
- tooth-whitening products
- hydrogen peroxide
- phenol
- silver nitrate
- certain endodontic materials
- cotton roll
what tissues are targeted in noninfectious oral complications or antineoplastic therapy (aka anticancer treatment)?
tissues with rapid turnover, like the oral epithelium
how many people a year suffer acute or chronic oral side effects from anticancer treatment?
half a million people
___% of patients receiving head and neck radiation have oral ramifications
100%
___% of patients receiving BMT have oral complications
75%
what are the two predominant problems with anticancer therapy?
mucositis and hemorrhage
hemorrhage associated with anticancer treatments is secondary to ___. what are the most common presentations of hemorrhage?
- secondary to thrombocytopenia (from bone marrow suppression)
- oral petechiae and ecchymosis secondary to minor trauma are the most common presentations
how does mucositis that results from anticancer therapy present clinically?
- white discoloration from a lack of sufficient desquamation of keratin
- soon follows by a loss of keratin and replacement by atrophic mucosa
- areas of ulceration develop
what are 5 main complications of anticancer therapy other than hemorrhage and mucositis?
- xerostomia
- loss of taste
- osteoradionecrosis
- trismus
- developmental abnormalities
describe xerostomia that results from anticancer treatment
- salivary glands are very sensitive to radiation
- increase in caries risk
describe loss of taste that results from anticancer treatment
- loss of all four tastes (hypogeusia) develops, but taste returns in about 4 months
- some patients have a permanent altered taste (dysgeusia)
osteoradionecrosis associated with anticancer treatment occurs in about ___% of people receiving head and neck radiation
5%
the risk of osteoradionecrosis associated with anticancer treatment increases dramatically if what procedure is performed and during what time frame?
local surgical procedure is performed within 3 weeks of therapy or within 1 year after therapy
most cases of osteoradionecrosis associated with anticancer treatment are secondary to ___
local trauma
___ is the main associated factor for osteoradionecrosis associated with anticancer treatment
radiation dose
before therapy, what should be eliminated to avoid cases of osteoradionecrosis associated with anticancer treatment?
all foci of infection should be eliminated
what is BRONJ?
bisphosphonate-related osteonecrosis of the jaw
what are bisphosphonates used for?
- inhibit osteoclasts
- possibly interfere with angiogenesis
- slow osseous involvement of cancer
- treat paget’s disease
- reverse osteoporosis
which generation bisphosphonates have a low potency and are readily metabolized?
first generation
second generation bisphosphonates are more potent than first generation, and are termed ___ due to the addition of a nitrogen side chain
aminobisphophonates
___ generation bisphosphonates are incorporated into the skeleton and have a half-life of 10 years; what location is the incorporation of the medication the highest?
- second
- the incorporation of the medication is highest in areas of active remodeling, such as the jaws
there is a strong association of ___ with aminobisphosphonates
gnathic osteonecrosis
95% of BRONJ occurs in patients who have received ___ for cancer. 85% of these patients had what type of cancer?
- IV formulations for cancer
- multiple myeloma
what is the prevalence of osteonecrosis in pateints taking IV bisphosphonates? what bout patients taking oral bisphosphonates?
- 6-8%
- 1:100,000
60% of BRONJ occurs after ___, ad the remaining 40% occur ___. what fraction are asymptomatic?
- dental procedures
- spontaneously
- 1/3
what is the treatment for BRONJ?
- formulation of the drug
- extend of disease
- duration of drug use
should routine dental therapy be modified for patients with BRONJ?
no
in the dental office, what should you do for patients taking PO bisphosphonates before bone manipulation? what about for patients taking IV bisphosphonates?
- informed consent before bone manipulation
- bone manipulation should be avoided in patients taking bisphosphonates
if BRONJ is suspected, you should refer your patient to who?
the oral surgeon
how can methamphetamines be ingested?
powdered stimulant can be smoked, snorted, injected, or taken orally
most methamphetamine users are male or female? what age?
men ages 20-40
many methamphetamine users develop delusions of ___
parasitosis (neurosis that produces the sensation of snakes/insects crawling on or under the skin)
rampant dental caries can occur with methamphetamine use. what surfaces are affected first? what is it that actually causes rampant dental caries?
- affects facial smooth and interproximal surfaces first
- due to poor oral hygiene and extreme xerostomia, leading to consumption of sugary and acidic drinks/foods
meth potentiates which local anesthetics for up to 6 hours?
sympathomimetic amines
use of local anesthetics with epinephrine in meth patients can lead to what 3 things?
- hypertensive crisis
- cerebral vascular accident
- myocardial infarction

linea alba

morsicatio buccarum

morsicatio linguarum

traumatic ulceration

traumatic ulceration

traumatic ulcerative granuloma with stromal eosinophilia
TUGSE

riga-fede disease

electrical burn

thermal burn

chemical burn
(from tooth-whitening strips)

chemical burn
(from aspirin)

chemical burn
(hydrogen peroxide)

chemical burn
(phenol)

chemical burn
(endodontic materials)

chemical burn
(cotton rolls)

noninfectious oral complications of antineoplastic therapy

noninfectious oral complications of antineoplastic therapy

noninfectious oral complications of antineoplastic therapy
patient received head and neck radiation

osteoradionecrosis
patient received head and neck radiation

osteoradionecrosis

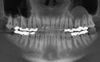
medication-related osteonecrosis of the jaw
aka bisphosphonate-related osteonecrosis of the jaw

medication-related osteonecrosis of the jaw
aka bisphosphonate-related osteonecrosis of the jaw

methamphetamine-related dental caries
___ is persistent scaling and flaking of the vermillion border, and typically involves both lips
exfoliative cheilitis
exfoliative cheilitis arises from excessive production and desquamation of ___
superficial keratin
exfoliative cheilitis is usually due to chronic injury secondary to ___
habits such as lip licking
is exfoliative cheilitis more common in males or females?
females
what is the treatment for exfoliative cheilitis?
cessation of habits, corticosteroids, psychotherapy, or ruling out other underlying cause (fungus, for example)

exfoliative cheilitis
___ appears as a nonblanching zone with a red, pruple, blue, or black color
submucosal hemorrhage
what are two types of submucosal hemorrhage?
oral petechiae and purpura
what are some causes of oral petechiae/purpura?
- repeated coughing or vomiting
- convulsions
- oral sex
- anticoagulant therapy
- thrombocytopenia
- disseminated intravascular coagulation
- viral infections, especially mono and measles
what is the treatment for submucosal hemorrhage?
no treatment is required if the hemorrhage is not associated with systemic disease; the areas should resolve spontaneously

submucosal hemorrhage (petechiae/purpura)
___ is a clinically evident lesion caused by pigmented materials that can be implanted in the oral mucosa
amalgam tattoo
(can happen with other materials, but amalgam is by far the most common)
what are some ways that amalgam can be incorporated into the oral mucosa?
- previous areas of mucosal abrasion can be contaminated by amalgam dust within the oral fluids
- broken amalgam pieces can fall into extraction sites
- contaminated dental floss can create linear areas of pigmentations
- endodontic retrofill can be left in the soft tissue
- high-speed drills can drive fine particles in tissue
in addition to amalgam, submucosal implantation of what other pigmented materials can occur?
- pencil graphite
- coal dust
- metal dust
- broken carborundum disks
- dental burs
___ appear as macules or (rarely) as raised lesions which are blue, black, or gray in color
amalgam tattoos
any mucosal surface can be involved with an amalgam tattoo
what are the most common sites?
- gingiva and alveolar mucosa
- buccal mucosa
what do PA radiographs of amalgam tattoos look like?
- they are usually negative
- when metallic fragments are visible on the radiograph, the clinical area of discoloration is large and extends past the size of the fragment
how should you confirm the diagnosis of an amalgam tattoo to rule out melanoma?
- take a radiograph of the affected areas
- no treatment required if it can be detected via radiograph
- to rule out melanoma, a biopsy must be done if it is not detected on the radiograph

exfoliative cheilitis

amalgam tattoo

amalgam tattoo

amalgam tattoo

amalgam tattoo
over 50% of college students have body piercings beyond the ___
earlobe
describe forked tongue
- the anterior 1/3 is split down the middle by pulling fishing line through a pierced hole and tightening the loop over a period of 3 weeks
- if a laser or surgical instrument is used, cautery is necessary to prevent the halves from reuniting
what is susuk?
implantation of a form of talisman (magical charm) in the orofacial region
susuk is common in what area of the world, and is placed why who?
- southeast asia
- placed by a native american magician or medicine man
what is susuk placement thought to do?
- enhance or preserve beauty
- relieve pain
- bring success in business
- provide protection against harm
the majority of people with susuk are ___
muslim, although islam prohibits black magic
for this reason, individuals may deny placement of susuk even when confronted with evidence
what is susuk shaped like? what is it made out of?
- shaped like a needle; one pointed end and one blunt end
- most are silver or gold and are 0.5x0.5mm
___ vary from one to many and are inserted subcutaneously
susuk pins
most patients with susuk are what age?
middle-aged adults
what do susuk pin implants look like?
no clinical evidence exists; only found via routine radiograph

forked tongue

susuk
are forked tongues and susuk associated with harmful effects? what is the treatment?
no, so no treatment is required
___ occurs due to nicotine, which stimulates melanin production
smokers melanosis
in patients with smokers melanosis, 20% of tobacco smokers 3% of nonsmokers have ___
oral pigmentation
smokers melanosis most commonly affects what gingiva?
anterior facial gingiva
in patients with smokers melanosis, reverse smokers show changes on ___
hard palate
in patients with smokers melanosis, cessation of smoking results in ___
gradual disappearance
when is a biopsy considered in smokers melanosis cases?
when pigmentation is in unexpected locations or if there are clinical changes

smokers melanosis
___ appear as dome-shaped, slight radiopaque lesion arising from the intact floor of the maxillary sinus
antral pseudocysts
antral pseudocysts consis of ___
an exudate (serum, not mucin) that has accumulated under the sinus mucosa and caused a sessile elevation
antral pseudocysts are common found ___
on panoramic radiographs
antral pseudocysts are present in ___% of the population
2-15%
what is the treatment for antral pseudocysts
no treatment necessary
antral pseudocyst
___ arises from introduction of air into the subcutaneous or fascial spaces of the face and neck
cervicofacial emphysema
when can cervicofacial emphysema arise?
- after use of compressed air
- after difficult/prolonged extractions
- result of increased intraoral pressure (sneezing) after an oral surgery procedure
in patients with cervicofacial emphysema, what should you avoid during oral surgery?
do not use air-driven handpieces
in cervicofacial emphysema, initial change is ___. after the initial air spreads, what happens?
- a painless soft tissue enlargement
- the enlargement increases and it becomes painful
what is the treatment for cervicofacial emphysema?
broad-spectrum antibiotics
resolves within 2-5 days

cervicofacial emphysema
