[T or F] Posterior Cul-De-Sac fluid accumulation in a pregnant woman is an abnormal finding
FALSE
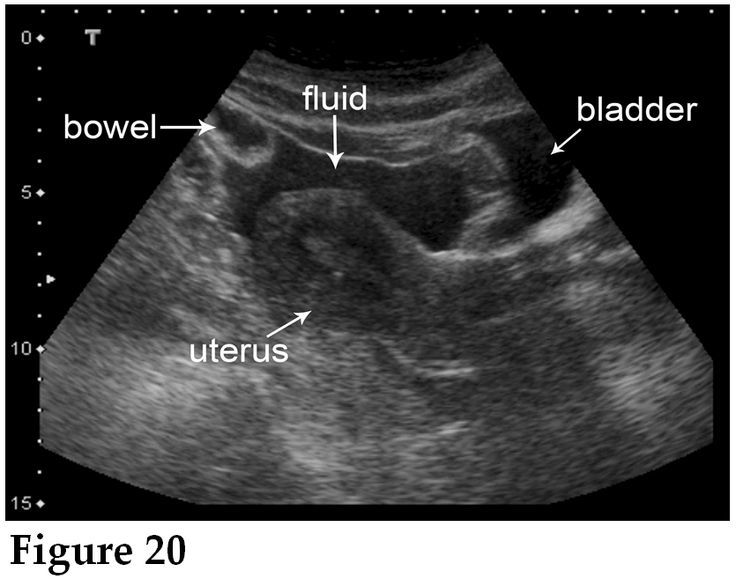
(this is a normal finding for preggos along with corpus luteum ovarian cyst UNLESS IT’S IN THE SETTING OF ECTOPIC. THEN IT MEANS HEMOPERITONEUM)
Which CA does breastfeeding reduce - 2
- Breast
- Ovarian
Breastfed infants have a Decreased risk of what conditions - 5
- SinoPulmonary infection (Ear, Lung, GI, UTI)
- Necrotizing Enterocolitis
- Type 1 DM
- CA
- Childhood Obesity
For pts taking OCP
How does Estrogen affect Thyroid function?
Estrogen (OCP, Pregnancy) ⬆︎ T4 binding globulin –> mostly euthyroid state (slight HYPERthyroid sx) and normal TSH
How does fetal hyperglycemia affect newborns? - 3
it –> macrosomia, hypOglycemia, birth malformations
What are the 4 main inquries pts should be asked when coming in for L&D checks?
Can Mom Feel Baby?
Contractions?
Movement from Fetus?
Fluid leak vaginally?
Blood leak vaginally?
Which 4 drugs can you give to treat HTN in pregnant patients?
Mothers Loathe Nefarious HTN
Methyldopa / Labetalol > Nifedipine / Hydralazine
Explain what Pseudocyesis is
Somatization of stress –> activates [hypothalamic-pituitary-ovarian] axis –> early pregnancy sx without there actually being a baby in utero = nonpsychotic woman who mentally AND PHYSICALLY presents like she’s pregnant (may even misinterpret a pregnancy test!)
US and clinic pregnany test will be negative
Risk factors for Pseudocyesis - 2
- infertility hx
- prior abortion
Neonatal Abstinence Syndrome
Classic Signs-4 ; What drug usually causes this?
STTD
- Sneezes a lot
- Tremors w/sweating
- Tachypnea w/HIGH PITCHED CRY
- Diarrhea
From intrauterine exposure to Opiates (i.e. Heroin/Methadone)!
s/s of intrauterine cocaine exposure - 3
- Excessive sucking
- Jitteriness
- Hyperactive Moro reflex
Postpartum depression affects women during what time periods?
________________
What 2 methods are used to screen for this?
[within 1st year > first 3 mo]
________________
- [PHQ2 –(if both +)–> PHQ9]
- Edinburgh Postnatal Depression Scale
Screen prenatal, postnatal and well child
Give brief descriptions that differentiate Postpartum
Blues vs Depression vs Psychosis
- Blues = onsets PPD1, peaking at PPD5 and subsiding PPD14, worst w/lactation
- Depression = can onset between [1 month - 12 months after birth] Traditional s/s. Previous Depression hx is RF
- Psychosis = RARE but onsets IMMEDIATELY after birth
CP of [Edward’s Trisomy 18] - 8
- Prominent Occiput
- [Dysplastic malformed ears]
- Micrognathia (small jaw & mouth)
- VSD
- [shielded chest with wide nipples]
- Overlapping Fingers
- Absent Palmar creases
- Rocker-bottom feet
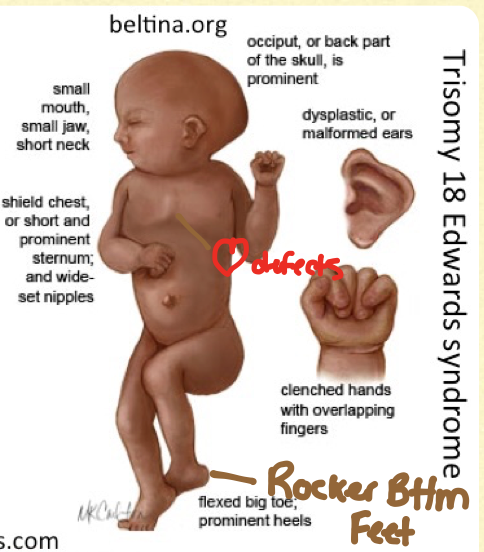
These pts die within 1st month of life
What are 5 ways to determine if a pt truly has Leakage of Amniotic Fluid?
- Amnisure immunoassay (detects placental ⍺-microglublin1)
- POOL test (there’s pool of fluid in vaginal vault)
- NITRAZINE test (fluid turns blue when placed on nitrazine paper since amniotic fluid is alkaline)
- FERN test (fern-like estrogen crystals under microscopy)
- US to determine fluid quantity (Normal = 6-23 cm AFI)
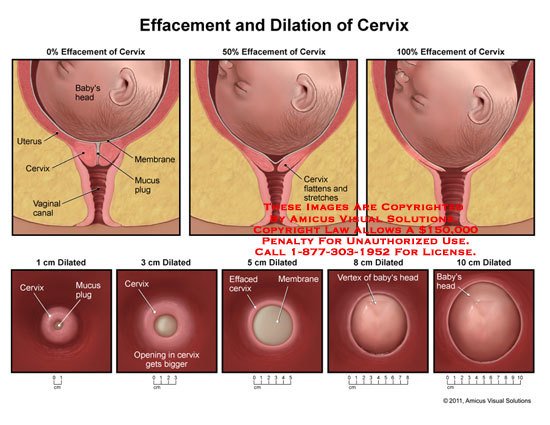
What are the 2 clinical features for diagnosing ACTIVE labor? -4
Labor = LAPD
- [Strong Contractions every 3-5 min]
- [Cervix Dilation > 6 cm]
- [Cervix growing at 1-2 cm/hr]
- [Cervix effaced]
Fetal Heart Tracing is IRRELEVANT to diagnosing active labor
After the Rupture of Membranes, when is it safe for labor to begin?
[1 - 18 hours after ROM] (no sooner ; no later)
________________
labor starting ≥18H after ROM ➜ chorioamnionitis ➜ neonatal sepsis
________________
- Do not confuse this with PPROM (Preterm Premature Rupture Of Membrane)*
- Chorioamnionitis Tx = Abx –> Delivery*
What constitutes an infant as “Full Term”?
37 - 42WG
For Antepartum patients, their NST (Non Stress Test) should be reactive
What is the Fetal Heart Tracing criteria for this?-4 Does this happen in pts in labor?
reactive = appropriate [fetal cerebral oxygenation]
- within a 20 min period there are
- at least two HR acclerations that are
- 15 bpm over baseline
- 1.5 small boxes long (15 sec)
THIS IS NOT REQUIRED FOR PTS IN LABOR
What is the normal Fetal Heart Rate and variability on a NST?
110 - 160/min (w/variability of 6-25)
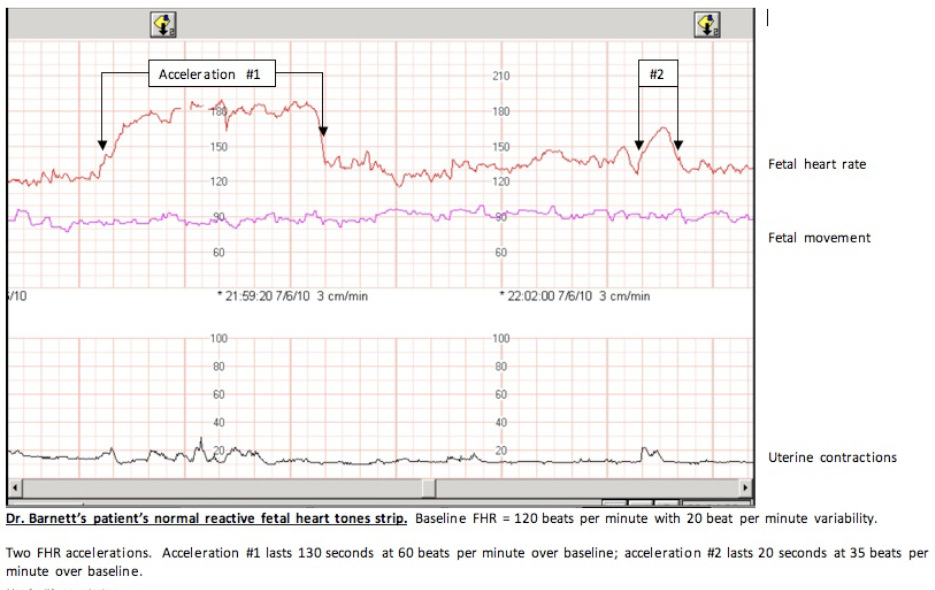
Normal Fetus’ should have a reactive NST
Criteria for PreEclampsia is Gestational HTN + [Proteinuria or End Organ Damage]
How do you clinically diagnose Gestational HTN? - 6
- NO previous HTN
- ≥ 20 WG (2nd trimester)
- Systolic > 140
- Diastolic > 90
- At least 2 readings taken > 6 hrs apart
- BP taken in seated or semi-reclined position
FYI: PreEclampsia can still occur superimposed on Chronic HTN
Criteria for PreEclampsia is Gestational HTN + Proteinuria
Which demographic are at greater risk for this?
Af American Women
greater risk of having PreEclampsia, it being severe and suffering placental abruptio and Eclampsia
What are the 4 major causes of Postpartum Hemorrhage? - 4
The 4 T’s!
Tone (Uterine aTony)
Trauma (Perineal vs Cervix lacerations vs Uterine inversion/prolapse)
Tissue (retinaed/invasive placental tissue)
Thrombin (rare bleeding DO)
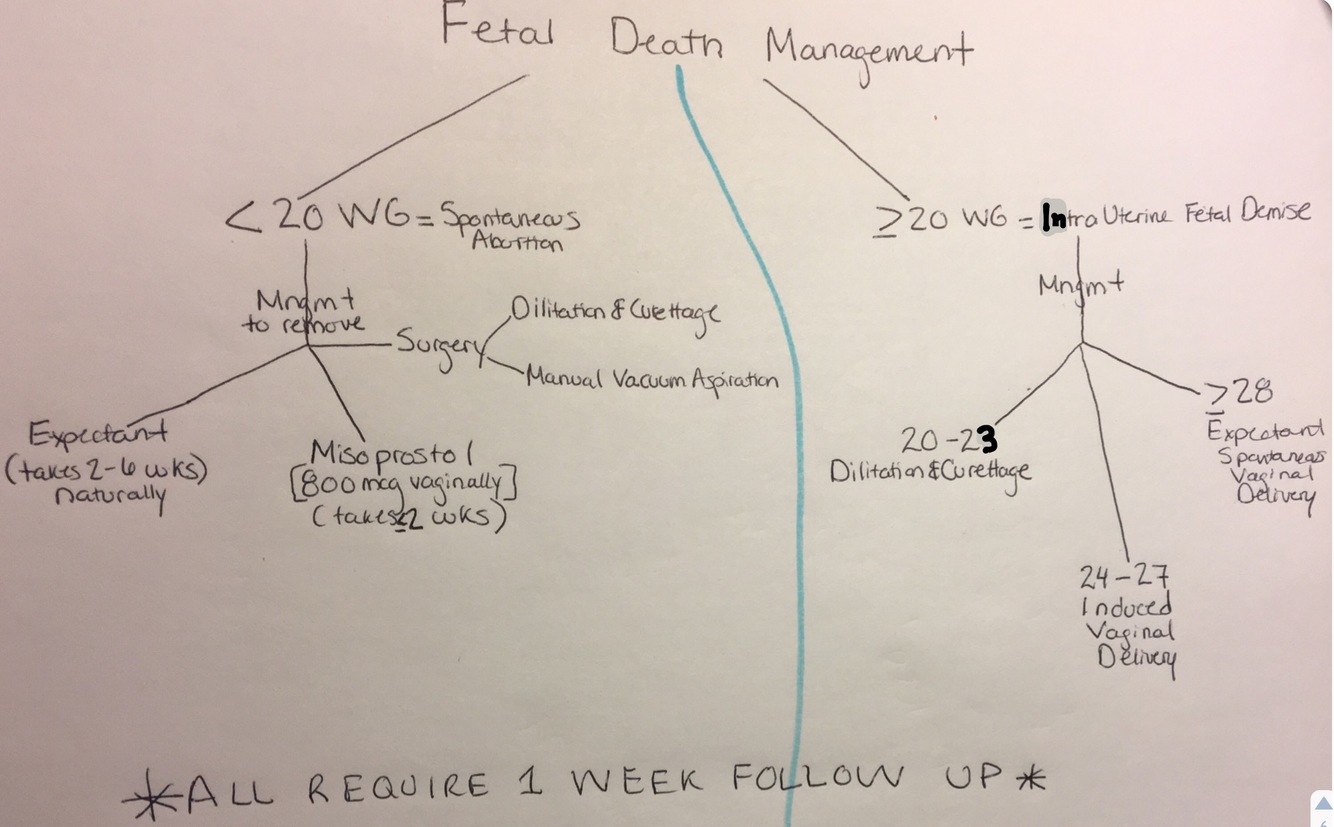
What is Intrauterine Fetal Demise (IUFD)?
________________
Dx?-3
fetal death ≥ 20WG BUT before onset of labor
________________
- No fetal cardiac activity on US
- No fetal heart tones on Doppler
- No/minimal subjective fetal mvmnt
This commonly occurs in uncomplicated pregnancies















































































































































-
✅FACTIONLESS258
-
✅F1 (ID/RENAL/ENT/ALLERGY)85
-
✅F2 (GI / RHEUM-ORTHO / HEME-ONC/ENDOCRINE/ SURGERY)125
-
✅F3 (PEDS/PREGNANCY/REPRO/UROLOGY/BREAST)169
-
✅F4 (PSYCH/EYE/DERM/BIOSTAT/TOX/Rx)40
-
✅Surgery277
-
✅Infectious Disease151
-
Pulmonary135
-
renal112
-
CARDIOLOGY217
-
Gastrointestinal141
-
✅Hematology/Oncology166
-
psYchiatry223
-
Rheumatology / Orthopaedic141
-
DM & Endocrine105
-
✅NEUROLOGY371
-
✅Derm52
-
Biochem/Rx/Optho67
-
Pregnancy & Child Birth377
-
✅PEDS95
-
Tox7
