Pathogenesis of Type II DM Flashcards
(22 cards)
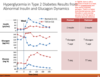
outline the natrual history of Type 2 diabetes in regards to beta cell function, insulin resistance, insulin secretion, post prandial gluose levels, fasting glucose levels.
beta cell functino gradually decreases over time
as weight is gained, insulin resistance increases
as beta cell function decreases, insulin secretion increases first(because of insulin resistance, which contributes to beta cell burnout), and then it decreases
post prandial glucose increases as insulin resistnace increases
fasting glucose also increases over time

reduced hepatic glucose output determines the __ glucose levels
increased hepatic glucose uptake determines __ stores
increase in peripheral (muscle/skeletal) glucose uptake accounts for 80% of all glucose disposal.

reduced hepatic glucose output determines the fasting glucose levels
increased hepatic glucose uptake determines glycogen stores
increase in peripheral (muscle/skeletal) glucose uptake accounts for 80% of all glucose disposal.

3 key organs that are affected by inslun resistance
- liver. insulin usually prevents glycogen breakdown (it’s an anabolic hormone). if the liver is resistant to insulin, then glycogenolysis can still happen adn there is an increase in glucose output
- muscle. insulin causes muscle cells to take up glucose. if it is resistance, cells do not take up as much glucose, leaving it in the blood stream.
- adipose tissue. same as muscle cells.

subcutaneous vs visceral fat in type II diabetes
Ct scnas from men matched for BMI shows that VISCERAL obesity drives CV risk progression independent of BMI. Visceral fat is not dormant– it is releasing cytokines– ceasing a pro-hypertensive sedate, pro-inflammatory state, and pro-thrombotic state

outline how insulin resistance can cause an increase in hypercoagulability

role of ffas in hyperglycemia
- adipose is resistant to insulin, so it breaks down (lipolysis), releasing FFas into the blood.
2 FFA mobilization causes increased FFA oxidation in muscle and liver
- beucase there is FFAs around, there is less glucose utilization by cells, and the liver has to thus store it through increased gluconeogenesis.
- overall, more FFAs= hyperglycemia because glucose cannot be used up.
Higher portal FFA results from metabolically more
“active”visceral fat mass
FFA as competitors for glucose metabolism – preferential oxidation reduces cellular glucose uptake

6 aspects of metabolic/insulin resistnace syndrome
- hyperinsulinemia
- abdominal obesity
- hypertension
- typertriglyceridemia/low HDL
- small dense LDL
- impaired glucose tolerance.
clinical precursors to overt DM2
metabolic/insulin resistnace syndrome
gestational diabetes
polycystic ovarian syndrome

Genetics – Monogenic forms of diabetes (insulin resistance forms)
- Insulin receptor mutations; TypeAIR, leprechaunism, rabson-mendenhall
- lipoatrophic diabetes
- PRAR- gamma mutations

outline normal insulin action/moa
insluin released by beta cells binds to cells all over the body, triggering the MAP kinase pathway to promote cell grwoth, as well as the Pi3K pathway, which triggers GLUT receptors (ex/ GLUT 4 on muscles and fat) to go onto the surface of the cell, making the cell absorb glucose

how does this glucagon-insulin dynamic change in T2dm?

. Insulin is a potent inhibitor of islet glucagon release. If the cell is not repsonsive to insulin, glucagon is not inhibited and it will continue to facilitate glycogenolysis and glucose release from stores and lipogenlysis
outline some genetic problems that contribute to insulin secretion

how does glucotoxicity affect insulin secretion?Chronically high glucose levels results in increased oxidative stress, which impacts the beta cells ability to produce insulin, creating a vicious cycle. High glucose levels also worsen insulin resistance as well. Chronically ugh glucose affects the beta cell. Fortunately, if early enough caught, there can be recovery of beta cell function
Chronically high glucose levels results in increased oxidative stress, which impacts the beta cells ability to produce insulin, creating a vicious cycle. High glucose levels also worsen insulin resistance as well. Chronically ugh glucose affects the beta cell. Fortunately, if early enough caught, there can be recovery of beta cell function

how does hyperglycemia affect insulin resistnace?
it interferes with the translocation of GLUT4 transpoters in the muscle and adipose tissue– so less GLUT4 receptors can get placed onto the membrane when insulin binds and triggers its placement. therefore ti causes insulin resistance- less glucose is taken up by the cells when insulin binds.

how does lipotoxicity affect type II DM/insulin resistance/beta cell dysfunction?

If we have insulin resistance, we have increased FFAs that decrease glucose uptake peripherally in muscle and liver, but also impede insulin secretion from pancreas as well. So its not just reduced tolerance, but it’s also impaired beta cell function.
Inflammatory markers released from adipocytes result in insulin resistance.

which gut peptide is impaired in type 2 dm?
INCRETIN
G astrointestinal incretin hormones potentiate insulin secretion in the postprandial period
◦ glucagon-like peptide-1 (GLP-1)
◦ glucose-dependent insulinotropic peptide (GIP)
◦ may be responsible for up to 70% of post-prandial insulin secretion
Type 2 diabetes the incretin effect is impaired, diminished or absent
Patients take food in GI tract, presence of food causes incretin release. This potentiates pancreas release of insulin, which allows more cells to take up glucose, bringing blood glucose levels down.
GLP gets broken down by DPP4, more GLP sticks around if you don’t have DPP4


note the cyclical nature

outline the renal contribution of the kideny to type II DM
T he kidney also has been shown to produce glucose
Hyperfiltation in early diabetes nephropathy. These patients might absorb more glucose into the system then needed. There is an up regulation of the SGLT2 expression.
- overall elevation of GFR



