Marino - Pancreas Flashcards
What is the starting point for acute pancreatic pathophys?
- Pathophysiology starts with intracellular activation of enzymes: conversion of pancreatic zymogens to their active forms within the acinar cell
- Local, systemic disease results from inflammatory processes and enzyme injury
What are the (4) protective mechanisms of the pancreatic acinar cell?
- Normal physiology protective mechanisms:
1. Inactive proenzymes
2. Membrane enclosed: no proteases in the cytoplasm
3. Separate pathways (compartments):
a. Secretory: Zymogen granules
b. Degradative: lysosomes -> can digest, activate some digestive proteases, so this sorting is important
4. Trypsin INH: scavenges activated proteases - NOTE: most efficient protein-synthesizing cell in the body

What are the normal nueronal/hormonal stimuli for pancreatic acinar cell secretion?
- Stimulus secretion COUPLING mechanism
- 1o stimulus: Ach and Ca IC signaling mechanism
- CCK/secretin: hormonal
- VIP/Ach: neuronal

What are the 2 key mechs of injury in acute pancreatitis?
- Blockage of secretion: reduction in exocytosis process due to stimulation
-
Co-localization of ZG and lysosomes, leading to premature zymogen activation and auto-digestion from within the acinar cell
1. Out of zymogen granules and into the cytoplasm, digesting the cell
2. AUTO-DIGESTION occurs from within, and expands to the rest of the pancreas

How are cytokines implicated in acute pancreatitis?
- Proteases activate complement
- C3a and C5a recruit PMNs and macrophages
- Inflammatory cells release cytokines: TNF-a, IL-1, PAF, and nitric oxide (NO)
- Vascular injury and inflammatory responses
- Local initially, then spread (in extreme cases)
What are the 3 local effects of acute pancreatitis? Clinical manifestation?
- LOCAL EFFECTS:
1. Auto-digestion of pancreas
2. Pancreatic swelling (edema)
3. Fat necrosis and hemorrhage - CLINICAL CORRELATE:
1. Pain, N/V
What is this?

- Normal pancreas: low-power view of lobules
- See attached image for high-power view

What is going on here?

-
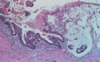
Acute pancreatitis: low-power view of fat necrosis between lobules -> dead adipocytes (no nucleus)
1. Can still see outline of the cell, but the wall becomes crinkly, and you will eventually see macros in here - Note the septate-appearing destruction of the pancreatic parenchyma (bottom left corner)
- Compare to attached normal image

What is this? What might the micro image look like?

- Gross image of fat necrosis in between pancreatic lobules in acute pancreatitis
- MICRO: fat necrosis with outlined, wrinkled appearance of the cells
1. Vessel walls dying (necrotic), so you can’t see endothelium -> hemorrhage into these spaces

What is this? Un-labeled arrows?

-
Acute pancreatitis: microvascular leak + edema
1. Fat necrosis: outlined, wrinkled appearance
2. Acute inflammation,
3. Destruction of pancreatic parenchyma, and
4. Destruction of blood vessels (can’t see endothelium) and interstitial hemorrhage - ARROWS: pancreatic parenchyma (top L), inflam infiltrate (top R), vessel w/necrotic walls (bottom R)
- Compare to attached “normal” image

What happened here?

-
Acute pancreatitis: high-power view of:
1. Coagulative necrosis (with ghost cells),
2. Hemorrhage
3. Degenerating polys - Note residual acini in bottom right
- Normal pancreas (high-power) attached here for comparison: A = acinus, D = duct, and I = islet

What is this? Circles? Micro?

- Acute necrotizing pancreatitis (gross): red-black from hemorrhage (blue), and contains interspersed foci of yellow-white, chalky fat necrosis (green), which can usually be seen on imaging
- Vascular injury can lead to hemorrhage into the pancreatic parenchyma
- In its most severe form (hemorrhagic pancreatitis), extensive parenchymal necrosis is accompanied by dramatic hemorrhage w/in substance of the gland
- MICRO: necrosis of acinar and ductal tissues, and islets of Langerhans
- REMEMBER: islets are the COCKROACHES, so it takes a lot for them to die

What is this? Arrows? Enzymatic causes?

- Severe, acute hemorrhagic pancreatitis
- BLACK ARROW: tan and yellow areas of fat necrotis -> lipase
- GREEN ARROW: hemorrhage -> elastase causes vascular damage
What is the systemic containment response to acute pancreatitis?
- Circulating a1-antitrypsin: inactivates circulating proteases
- Circulating a-macroglobulin: binds to circulating trypsin, and facilitates monocyte clearance of macroglobulin-trypsin complexes
What are the 4 types of containment failure in sever pancreatitis? Provide the cause and clinical correlates for each.
- INFLAMMATORY: TNF-alpha, IL-6 -> fever, malaise, confusion
- VASCULAR: kallikrein activation (potent vasodilator), thrombin activation, elastase, chymotrypsin -> hypotension, DIC/hemorrhage
- RESPIRATORY: phospholipase A2 (PLA2: compromises alveolar integrity) -> hypoxemia
- METABOLIC: fat saponification -> hypocalcemia
- NOTE: these are all systemic responses; pt that is feverish, low BP, and difficulty breathing -> ICU
What are the 3 steps in acute pancreatitis pathophys?
- STEP 1: acinar cell injury
1. Insult to pancreas: ETOH, obstruction, etc.
2. IC activation of zymogens
3. Cell necrosis and auto-digestion - STEP 2: local inflammatory response
1. Cytokines/chemokines released by acinar cells, and inflammatory cells recruited
2. Inflam mediators released: TNF-alpha, IL-1
3. Pancreatic and vascular injury - STEP 3: systemic response (hours - days)
1. Circulating inflam mediators: PAF, TNF-alpha
2. Systemic inflam response syndrome (SIRS): multi-organ failure in very severe cases
What are the causes, symptoms, dx, and mgmt of acute pancreatitis?
- MAIN CAUSES: gallstones and alcohol
- MAIN SYMPTOMS: abdominal pain, N/V
- DIAGNOSIS: elevated serum amylase and lipase, inflamed pancreas on CT scan
- MGMT: IV fluids to manage hypotension, pain meds, remove stones if causative
What are the etiologies of acute pancreatitis?
- MISCELLANEOUS: autoimmune, drugs, infection, iatrogenic, hyperlipidemia, scorpion bite, trauma, shock, hypercalcemia, genetic
- SCORPION BITE: cholinergic storm, so cAMP and Ca pathways hyperstimulated
- GALLSTONES: HTN, blocking duct
- MECH: blockage of secretion, co-localization of lysosomal/zymogen synthesis, enzymatic damage

What are the diagnostic criteria for pancreatitis?
- 2 of the following 3:
1. Abdominal pain, N/V
2. Elevated serum amylase and lipase >3x upper limit of normal
a. A lot of things INC amylase and lipase, so need to be careful here -> has to be a significant elevation
3. CT imaging showing pancreatic inflammation
What are the 2 hereditary forms of pancreatitis?
- Shared feature of most forms is a defect that INC or sustains the activity of trypsin (see attached)
1. Circulating trypsin more difficult to degrade, and stays in circulation longer (His = histidine) - 40% risk of malignancy due to chronic inflam
- Implicated genes:
1. PRSS1 (7q34): serine protease 1 (trypsinogen 1); cationic trypsin, and GOF muts prevent self-inactivation (AUTO DOM, and most common)
2. CFTR (7q31): cystic fibrosis transmembrane conductance regulator; epi anion channel, & LOF muts alter fluid pressure and limit bicarb secretion, leading to inspissation of secreted fluids and duct obstruction - NOTE: muts in CFTR -> 1) DEC bicarb secretion by pancreatic ductal cells, 2) promoting protein plugs, 3) duct obstruction, and 4) devo of pancreatitis

How does pancreaticobiliary anatomy permit gallstone obstruction?
- Gallstones travel down CBD, and can get lodged right at the ampulla of vater
- This would obstruct both the CBD and pancreatic duct, leading to HTN in the pancreas

What is this? What is it used for?

- ERCP: can be used in the diagnosis of CBD stones
What 5 factors suggest gallstone etiology of pancreatitis (GAP)?
- Age >50
- Female
- Amylase >4000 IU/L
- AST >100 U/L
- Alk phos >300 IU/L
What is endoscopic papillotomy?
- Endoscopic procedure used to relieve obstruction and drain
- Tx for GAP

How can congenital anomalies predispose to pancreatitis? Most common?
- Complex process by which dorsal and ventral pancreatic primordia fuse during panc devo prone to “imperfections”
- PANCREAS DIVISUM: most common (10% of pop, but pancreatitis uncommon) -> caused by a failure of fusion of fetal duct systems of dorsal and ventral pancreatic primordia
1. Inadequate drainage (dorsal duct smaller) may predispose these ppl to recurrent bouts of pancreatitis
2. Can put stent in to facilitate drainage

How is pancreatitis managed clinically?
- SUPPORTIVE MGMT, incl:
1. Close observation (hospitalization) + NPO
2. Very aggressive IV fluid replacement: 10-15L over 24 hrs to maintain vascular space and prevent ischemia of pancreas
3. Relief of pain
4. Nutritional support (if prolonged course)
5. Antibiotics (if biliary pancreatitis) - In general, not an infectious disease: due to metabolic injury and protease activation
- Retroperitoneal, epigastric pain, right above the aorta -> radiates to the back
- Alcohol: we don’t have access to the obstructions, so tx is supportive
What are the lab predictors of a poor outcome in pancreatitis?
- Admission Hct >44% w/failure to DEC after 24 hrs of IV fluids -> hemoconcentrated
1. This implies fluids being put in are escaping vascular space due to compromise from proteases - Admission BUN > 25 mg/dl w/INC after 24 hrs of IV fluids -> means kidneys continuing to perceive there is not enough volume in the vascular space
- CRP > 150 mg/L at 48 hrs -> general marker of inflammation, indicating local inflam response
What are the 3 prognosis scoring systems for pancreatitis?
- Ranson Criteria (pancreatitis-specific): 11 parameters measured on admission and at 48 hrs
-
APACHE II (any ICU admission; calculator): 12 physiologic parameters
1. Worst values in the first 24 hours - BISAP score (pancreatitis-specific, calculator): 5 parameters (BUN, SIRS, age, medical status, pulmonary effusion) -> “bedside” index
How can a CT help with pancreatitis prognosis?
- INTERSTITIAL pancreatitis (85%): <10% multi-organ failure rate, <1% infection rate, ~3% mortality
1. Edematous, swollen pancreas - NECROTIZING pancreatitis (15%): 50% multi-organ failure rate, 15-20% infection rate, and 17% mortality
1. Have to worry about these folks going to operating room & having pancreas debrided
What are some of the complications of acute pancreatitis?
- Fluid collections
- Pseudocysts
- Fistulas: ascites, pleural effusions
- Splenic vein thrombosis
Chronic pancreatitis: pathophys, cause, symptoms, dx, mgmt
- PATHOPHYS: recurrent injury w/tissue destruction and fibrosis
- CAUSE: chronic alcohol
- SYMPTOMS: chronic abdominal pain, diabetes, steatorrhea (diarrhea from fat malabsorption)
- DX: imaging studies
- MGMT: pain meds, insulin, enzyme supplements
What are the etiologies of chronic pancreatitis?
- Miscellaneous:
1. Cystic fibrosis
2. Hereditary
3. Tropical
4. Autoimmune

What is the pathophysiology of chronic pancreatitis?
- Often do not seek medical attention for subacute attacks
- Larger ducts do get calcified, and you can see this on imaging -> DIAGNOSIS
- Stellate cells: pro-fibrotic process -> these are in the liver too, and can lead to cirrhosis there
- Without acinar cells, islets, you have steatorrhea, weight loss, and diabetes

What is going on here? Arrows?

- Chronic pancreatitis: fibrosis, atrophy, dropout of acini, variably dilated ducts w/altered architecture
- TOP: extensive FIBROSIS
- 2nd: atrophy has left only residual islets
- 3rd: ducts
- BOTTOM: sprinkling of chronic inflammatory cells and few islands of acinar tissue
- Attached image: dilated ducts with inspissated eosinophilic ductal concretions

What is this?

- Chronic pancreatitis: end-stage with replacement of exocrine acini and ducts by fibroadipose tissue
- Preservation of islets of Langerhans: cockroaches
What is the clinical presentation of chronic pancreatitis?
- Chronic abdominal pain: 80% -> may be on narcotics for this
- Malabsorption (steatorrhea): 35% -> first food source to be affected is fat, so oily diarrhea
- Diabetes: 35%
What are 4 causes of pain in acute pancreatitis?
- INC pressure: physically encased in peritoneum, but inflamed due to acute bouts of pancreatitis in the setting of chronic disease
- Biliary strictures: can also be obstructed
- Neural inflammation: fibrotic, so no expansibility
- Acute focal pancreatitis: blockage from calcified stones and protein plugs leads to ductal dilatation, building pressure
- NOTE: can also get pseudocysts

How is pain managed in chronic pancreatitis?
- BY CAUSE:
1. Any cause -> narcotics
2. Acute exacerbation -> abstinence, enzymes (negative feedback that allows pancreas to rest -> controversial, and may not be helpful)
3. Neural inflam -> nerve block of SYM trunk
a. Splanchniectomy: surgical excision of segment of one or more splanchnic NN (removes nociception via splanchnic, SYM nervous system)
4. Ductal HTN -> drainage (stent, surgery)
5. Pseudocyst pressure -> drainage (stent, surgery) - NOTE: most pts end up on narcotics b/c there is not much that can be done for them
Cause and tx for steatorrhea in chronic pancreatitis?
- Fat malabsorption occurs b4 protein or carb -> lipase deficiency
- TREATMENT: reduce dietary fat intake
1. Oral enzyme supplementation
2. Acid suppression therapy: gastric acid can INH whatever proteases are available, so want to suppress this
Diabetes in chronic pancreatitis?
- Only in severe disease: >80% of gland destroyed
- Loss of insulin AND glucagon, so hard to control, aka, brittle diabetes (different than T1D)
1. Very hard to regulate b/c no counterbalance from glucagon - Low insulin requirements; ketoacidosis rare
CF: pathophys, symptoms, dx, tx
- PATHOPHYS: genetic disorder of defective Cl- secretion
- Pediatric presentation
- SYMPTOMS: lung infections, chronic pancreatitis, hypertonic sweat
- DX: sweat chloride test
- TX: antibiotics, pancreatic enzymes
Etiology of CF?
- Auto recessive: most common lethal genetic mut in Caucasians (gene frequency 1:25)
- Most CF is caused by 3bp deletion (DF508) that affects the folding, processing, and func of the CF gene product: cystic fibrosis transmembrane conductance regulator (CFTR)
1. CFTR is a cAMP-activated chloride channel
2. F = phenylalanine - NOTE: CFTR is also a major player in secretory diarrhea (not just in CF, but everybody)
What is the pathophys of CF?
- Defective Cl- secretion
- Inspissated (thickened) secretory product
- Obstruction of ducts and lumens
- Infection, inflammation, and tissue destruction
What are the clinical manifestations of CF?
- Obstructive/inflammatory lung disease
- Chronic pancreatitis: blockage of ducts due to thickened secretion
- Hepatobiliary tract disease
- Meconium ileus in infants: thickened concretions in bowel, causing obstruction
- Hypertonic sweat
- Infertility
How is CF diagnosed?
- CLINICAL SYMPTOMS: frequent pulm infections, esp. pseudomonas
1. Diarrhea (steatorrhea), malabsortion, failure to thrive
2. Frequent episodes of dehydration - TESTING: sweat chloride test
1. Pulmonary function tests
2. Genetic testing
What is the clinical mgmt for CF?
- Daily pulmonary toilet (vibration via banging on the back)/inhalers.
- Treatment of pulmonary infections
-
High-dose pancreatic enzymes: can manage this (lung disease is primary issue for these pts)
1. Chronic pain, an important part of alcoholic pancreatitis, is not really a key feature here - Gene transfer
What do you see here?

- Pancreas early in CF: numerous ducts severely distended with inspissated, dark pink secretions, atrophy of acini, and mildly INC fibrous tissue
1. Ducts much more prominent than in normal pancreas - ARROWS: pancreatic lymph nodes
- Compare to normal pancreas attached here: minimal pink fibrous tissue, and minimal thin secretions in ducts

What is this? White arrows? Black arrows?

- Pancreas in CF: ducts severely dilated with pink-purple inspissated secretions
- WHITE: atrophic acini
- BLACK: islets, likely w/autolysis artefact
What do you see here?

- Pancreas late in CF: fibroadipose replacement of exocrine portion
- Can eventually be totally replaced
What are the 2 categories of pancreatic cysts? Subtypes?
- BENIGN cysts:
1. Pseudocysts: most common of these two
2. Rare, non-neoplastic cysts - CYSTIC NEOPLASMS: vary in progression to adenocarcinoma
1. Serous cystic tumors
2. Mucinous cyst neoplasms
3. Intraductal papillary mucinous neoplasms
4. Solid, pseudopapillary neoplasms
What is the diagnostic eval for pancreatic cysts?
- Imaging studies to assess cyst size
- Endoscopic ultrasound
–Assess structure
–Obtain fluid and tissue for analysis
•Serum tumor markers
–CEA for mucinous cystic neoplasms
•ERCP for intraductal papillary mucinous neoplasms
–Endoscopic retrograde cholangiopancreatography
What is this?

- Serous cystic neoplasm: typically in WOMEN, and 25% assoc w/VHL
- Benign, multicystic
-
TAIL of the pancreas and small (1-3 mm)
1. Location really helps with these (i.e., body vs. tail) - HISTO: lined by glycogen-rich cuboidal cells, and contain clear, thin, straw-colored fluid
- See attached GROSS image

What is this?

- Mucinous cystic neoplasm: women, and can be precursors to invasive carcinoma
- Also in the TAIL
- HISTO: columnar, mucin-producing epithelium assoc w/dense stroma similar to ovarian stroma (cellular, busy)
1. Thick tenacious mucin
2. KRAS oncogene & TP53 tumor suppressor genes frequently mutated

What do you see here?
- Intraductal papillary mucinous neoplasm: mucin producing, and in larger ducts (expands them)
- Men>women, and in the HEAD of the pancreas
- Can progress to cancer
- HISTO: 2 features useful in distinguishing these from mucinous cystic neoplasms:
1. Absence of dense “ovarian” stroma seen in mucinous cystic neoplasms, and
2. Involvement of a pancreatic duct - Frequent GNAS, KRAS, p53 mutations reported

What is this?

- Solid, pseudopapillary neoplasm: young women
- Often cause abdominal discomfort b/c large
- Can be locally aggressive, but most pts are cured after complete surgical resection
- HISTO: solid sheets that become dishesive
- GROSS: large, well-circumscribed malignant neoplasm with solid and cystic components filled with hemorrhagic debris
1. Not true fibrovascular cores, but cells holding onto vessel wall as tumor separating, giving a pseudopapillary appearance

What is this?

- Solid pseudopapillary neoplasm: large, well-circumscribed malignant neoplasms have solid and cystic components filled with hemorrhagic debris
- HISTO: s_olid sheets_ that become dishesive
- Not true fibrovascular cores, but cells holding onto vessel wall as the tumor is separating, giving a pseudopapillary appearance (see attached)

What is this?

- Pancreatic pseudocyst: hemorrhagic fat necrosis walled off by fibrous and granulation tissue (trying to hold everything in)
- NO EPITHELIAL LINING
- Can drain these surgically
- BENIGN -> no malignant potential
- NOTE: she said this was important, & mentioned it in her review session

What are the risk factors, common presentations, and prognosis for pancreatic cancer?
- Vast majority are adenocarcinomas of ductal orgin
- RISK FACTORS: cigarette smoking
1. Alcohol in setting of chronic pancreatitis
2. Hereditary pancreatitis
3. Family hx of pancreatic cancer - PRESENT: with abdominal pain and weight loss
- PROGNOSIS: poor, unless caught very early
Diagnosis of pancreatic cancer?
- CLINICAL: weight loss, abdominal pain, jaundice
1. Jaundice actually a good thing b/c if tumor is in head of pancreas (causing jaundice), physician may catch it earlier -> those who have it in body/tail don’t present until too late - LAB: elevated serum CA19-9 -> no tumor marker good, but this one most used; assoc w/bile ducts
- IMAGING: mass on CT or MRI, endoscopic US with FNA
What is Trousseau sign?
- Migratory thrombophlebitis: occurs in about 10% of pancreatic cancer pts
- Attributable to elaboration of platelet-activating factors and procoagulants from the carcinoma or its necrotic products
What do you see here?

- Pancreatic cancer mass on CT: can see the pancreatic duct here, which you should not be able to see -> this suggests obstruction
- CBD and biliary tree also obstructed, so dilated intrahepatic bile ducts here too

What are the mgmt considerations for pancreatic cancer?
- 70% arise in head of the pancreas.
- At presentation: 40% w/mets (unresectable; S4)
2. 40% w/advanced local disease (Stage 3: also unresectable)
3. 20% organ-confined disease (resectable), but <50% of these can be cured - Chemo, radiation tx have limited effectiveness
- At presentation, 10% have chance of cure post-sx
What are the surgical options for pancreatic cancer?
- CURE: distal pancreatectomy for tail lesions (S1)
2. Whipple resection for head lesions (major reconstructive surgery) - PALLIATION: relieve biliary obstruction (drainage)
1. Relieve gastric outlet obstruction
2. Splanchniectomy for pain control: more effective here than in chronic pancreatitis
What does survival look like for pancreatic cancer?
- POOR
- 90% of these are ductal adenocarcinomas

What is the predominant histology of pancreatic cancer?
- 90% ductal adenocarcinomas
- 10% miscellaneous, including:
1. Cystic neoplasms
2. Acinar cell neoplasms
3. Lymphomas and sarcomas
4. Neuroendocrine tumors (gastrinoma, insulinoma, glucagonoma)
What are the 3 recognized precursors of pancreatic cancer?

- Infiltrating ductal adenocarcinoma of the pancreas has 3 precursors:
1. PanIN (attached): pancreatic intraepithelial neoplasm
2. IPMN: intraductal papillary mucinous neoplasms
3. Mucinous cystic neoplasms - KRAS, p53: do not need to memorize this whole sequence, just the concept of progression

What is this?

- Pancreatic carcinoma: 60% in head of pancreas
- Hard grey stellate masses
- Most are ductal, and produce mucin
- Highly invasive and produces a DESMOPLASTIC response

What is this? How can you tell?

- Well-differentiated pancreatic carcinoma in background of extensive fibrous tissue: can tell it is not just fibrosis due to cytologic and cellular atypia (and staining)
- ATTACHED:
1. A: benign duct in chronic pancreatitis with equally sized cells showing no nucleoli
2. B: ductlike gland in pancreatic ductal adenocarcinoma with nuclear pleomorphism and distinct nucleoli
3. Ductlike structures in pancreatic ductal adenocarcinoma showing intense nuclear labeling by Ki-67 (A) and p53 (B) - Ki-67 tells you if cell is actively replicating; usually don’t have to do the p53

What do you see here?

- Moderately differentiated pancreatic carcinoma: poorly formed glands, back-to-back
- Numerous cells with huge nuclei and individually invading tumor cells
- Note the poorly formed glands with anaplastic cells in the attached image

Why is this image important?

- Accurate histo assessment of resection margins is key in pancreatic cancer b/c sx offers only chance for a cure
- Resectable adenocarcinomas in the pancreatic head: the retroperitoneal resection margin is an independent prognostic factor
- WHIPPLE resection: can be very challenging to check margins
What is this?

- Pancreatic adenocarcinoma: sometimes difficult to appreciate how difficult it is to call a pancreatic resection margin positive or negative on frozen section
- LEFT: well-differentiated adenocarcinoma with surrounding stromal fibrosis
- RIGHT: residual neoplastic glands (arrows) with marked therapeutic changes, incl. stromal fibrosis and acinar atrophy

What syndromes/genes are associated with pancreatic neoplasms (table)?
- Focus on the #’s in red
- KRAS and p53

What are the roles of the following genes: p16, p53, SMAD-4, GATA-6 (table)?

