How much water is normally excreted in the stool? Where does it all go?
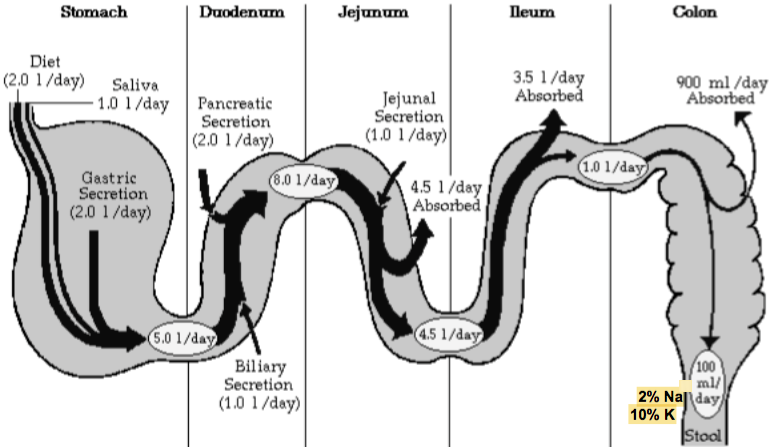
- Normal stool water: 125mL +/- 75mL (so, diarrhea when H2O in stool exceeds 200mL)
- About 9L enters gut each day (2L dietary)
1. 4.5L absorbed by jejunum
2. 3.5L by ileum
3. 900mL by colon - NOTE: PNS activity wanes as we age, INC chances of constipation (diabetes also a contributing factor)
What are the 5 groups of laxatives?
- Dietary fiber and bulk-forming: all taken orally, and INC water delivery to the colon
- Surfactant: stool softeners that lower surface tension b/t gut contents and intestinal wall
- Osmotic: contain Mg cations or o/non-absorbable molecules, and exert an osmotic effect that retains water in the lumen of the G. I. tract
- Stimulant: predominantly act on lg bowel, and INC intestinal permeability, back diffusion of water and electrolytes, and propulsive contractility
- Miscellaneous
What are the 4 dietary fiber/bulk-forming laxatives?
- Psyllium husk
- Semisynthetic celluloses
- Polycarbophils
- Functional fiber
- NOTE: all taken orally, and form gritty substance when added to water (except new formulation of functional fiber that completely dissolves and has no taste)
What are the class, characteristics, AE’s for psyllium husk?
- CLASS: dietary fiber/bulk-forming laxatives
- CHARACTERISTICS: hydrophilic muciloid that forms gelatinous mass when mixed with water
- AE’s: allergic rxns, flatulence, borborygmi, intestinal obstruction
1. May INH coumadin (Warfarin) absorption
What are the class, characteristics, AE’s for semi-synthetic celluloses (carboxymethyl and methyl)?
- CLASS: dietary fiber/bulk-forming laxatives
- CHARACTERISTICS: hydrophilic and digestable; form a colloid mass with water
- AE’s: may bind and impede drug absorption
What are the class, characteristics, AE’s for polycarbophils?
- CLASS: dietary fiber/bulk-forming laxatives
- CHARACTERISTICS: hydrophilic, polyacrylic resins; absorb 60-100x their weight in water
- AE’s: Ca+ polycarbophils release Ca+ that is contraindicated with tetracycline usage
What are the class, characteristics, MOA, and net result of functional fiber?
- CLASS: dietary fiber/bulk-forming laxatives
- CHARACTERISTICS: isolated, non-digestible carbs that have beneficial effects in humans
1. Best type of fiber is dietary fiber -> advise to INC intake b/c diet with sufficient amt of fiber should foster normal bowel function (25-38g/d) - MOA: INC delivery of water to colon, INC bulk, and reduce pressure in sigmoid colon
- NET RESULT: more formed stools
What are the 3 surfactant laxatives? MOA?
- Docusates: dioctyl sodium (Ca2+) sulfo-succinate
- Poloxamers
- Castor oil
- MOA: reduce water tension b/t stool and intestinal epithelium
What are class, characteristics, and AE’s for the docusates?
- CLASS: surfactant laxatives (capsules)
- CHARACTERISTICS: anionic surfactant primarily used as stool softener
1. Reduce strain of defecation, and DEC water tension b/t stool and intestinal epithelium
2. No effect on intestinal peristalsis - AE’s: not for use during abdominal pain or vomiting
1. Can irritate intestinal mucosa and INC absorption of other drugs
2. Recommended for SHORT-TERM USE: w/use <1 (to 2) wks, no long-term consequences, but can cause epithelial damage and inflammation when used long-term
What are the class, characteristics, and AE’s for the poloxamers?
- CLASS: surfactant laxatives
- CHARACTERISTICS: non-ionic surfactant similar to docusates; stool softener
- AE’s: diarrhea
1. Not for use during abdominal pain or N/V
What are the class, characteristics, and AE’s for castor oil?
- CLASS: surfactant laxatives
- CHARACTERISTICS: rapid-acting, effective anionic surfactant that produces CATHARSIS (complete evacuation of the colon; much more potent)
1. Stimulates intestinal peristalsis - AE’s: colic, dehydration, and electrolyte imbalance with OD
1. Can induce uterine contraction in pregnant women
What are the 2 stimulant laxatives? MOA?
- Diphenylmethanes (bisacodyl)
- Anthraquinones
- MOA: predominantly act on LARGE BOWEL
1. INC permeability of intestinal mucosa
2. Act on tight junctions to INC back-diffusion of water and electrolytes
3. INC propulsive contractility of colon by stimulating colonic mucosal myenteric plexus: food matter travels through the colon faster, allowing less absorption
4. Stimulate PG synthesis, and INC intestinal secretions - MOST POTENT class of laxatives
What are the class, characteristics, and AE’s for diphenylmethans (bisacodyl)?
- CLASS: stimulant laxatives
- CHARACTERISTICS: prodrug converted by enteric bacteria into deacetyl active form
1. Administered in enteric-coated tablets so it doesn’t dissolve until it gets to intestine
2. Taken at night, like all laxatives, and produces effects in the morning - AE’s: OD can cause excessive fluid and electrolyte loss, intestinal enterocyte damage leading to colonic inflammatory response
1. Need to ensure pt. has high enough fluid intake
What are the class, characteristics, and AE’s for anthraquinones?
- CLASS: stimulant laxatives
- CHARACTERISTICS: natural derivatives of Lilliaceae plants (senna, cascara); more gentle than synthetic drugs -> acts by promoting colonic motility
- AE’s: may cause melanotic (dark) pigmentation of colonic mucosa and abnormal urine coloration, at least for the first couple of days
What are the 3 types of saline/osmotic laxatives? MOA?
- Mg-containing
- Phosphate-containing
- Non-digestible sugars/alcohols: lactulose, glycerin, and PEG electrolyte solution (GOLYTELY)
- MOA: contain Mg cations or other non-absorbable molecules, and exert osmotic effect that retains water in lumen of GI tract
1. Largest class, and each has a different use
2. REMEMBER: absorption in colon is iso-osmotic; ions not normally absorbed by the gut
Class, MOA, and examples of Mg-containing laxatives?
- Saline/osmotic laxatives
- MOA: produce laxation by osmotic effect + release of CCK, which INC intestinal motility and secretion
- Mg sulfate: epsom salt (poor man’s laxative)
- Mg hydroxide: type of thing dr. prescribes; take at night (pts after surgery)
- Mg citrate: cathartic (4-8oz dose)
Phosphate-containing laxatives?
- Saline/osmotic laxatives
- Given as enema (fleet) or oral sodium phosphate tablets
- Enemas traditionally used in severe constipation, or in prep for lower colonic exams
- Now have oral tablets, which are used in prep for colonoscopy, providing complete evacuation of the bowel (take 32 tablets overnight)
Lactulose class, characteristics, and MOA?
- CLASS: saline/osmotic laxatives
- CHARACTERISTICS: semi-synthetic disaccharide that is not absorbed, and has osmotic laxative effect + diarrhea that discharges ammonium ions
1. Metabolized by enteric bacteria to organic acids like lactic, formic, and acetic acid - MOA: fecal acidifier used in mgmt of symptoms of liver failure (portal systemic encephalopathy)
1. Acidification of stool traps ammonia in non-toxic ammonium form (ammonia detoxification is important func of liver, which converts it to urea)
2. Retards non-ionic diffusion of ammonia from colon to blood b/c NH3 is in ammonium form, which is non-diffusable - REMEMBER: the sources of ammonia are proteins and enteric bacteria, and it diffuses freely -> pts with liver failure can get lethargic, and even go into coma
Glycerin class and characteristics?
- CLASS: saline/osmotic laxatives
- CHARACTERISTICS: osmotic and lubricant effects
1. Suppository
Polyethylene glycol electrolyte solution class and characteristics?
- CLASS: saline/osmotic laxatives
- CHARACTERISTICS: dissolved into 4L and ingested for colonoscopy, where complete evacuation is needed
1. Collapsed, plastic gallon they have to fill with water, and drink overnight - Aka, GOLYTELY
What are the 2 miscellaneous laxatives?
- Mineral oil: mixture of hydrocarbons that penetrates and softens stool
- Castor oil: an emulsion that irritates mucosa and produces a cathartic effect
1. INC mucous secretion
What laxatives are used in the mgmt of IBS?
- IBS: bloating and constipation of unknown etiology; 10:1 female
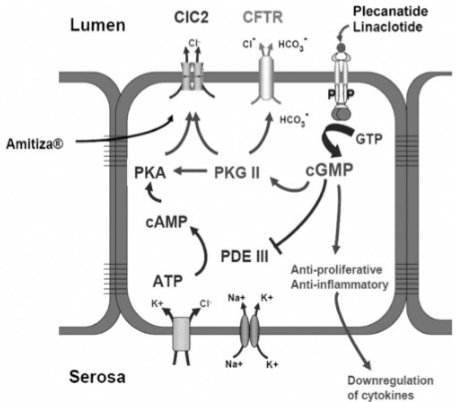
- 2 drugs currently approved: target Cl- channel (Lubiprostone) or GC system (Linaclotide)
1. LUBIPROSTONE: acts directly on Cl- channels, activating them in protein kinase A-independent fashion -> INC intestinal fluid secretion, motility, and alleviates the symptoms associated with chronic idiopathic constipation
2. LINACLOTIDE: peptide agonist of guanylate cyclase 2C that acts on intestinal cells to indirectly activate the Cl- channel
Why is laxative abuse a problem?
- Overuse leads to thorough constipation that requires several days to accumulate bulk
- Lag in defecation interpreted as continued constipation, so pts take more laxatives, leading to a vicious cycle
- If continued, the bowel becomes unresponsive
1. Colon damage + psych effect -> need to INC fiber in diet to repair GI tract, and overcome constipation
What are the 3 groups of anti-diarrheals?
- Absorb/adsorbers: pull in water, bacteria, viruses, or toxin
- Opiates
- Anti-cholinergics
-
Johnson - Physiology95
-
Gupta - Pathology148
-
Sweatman - GI System Pharm23
-
Ray - Gastroparesis35
-
Jackson - Gastric Neoplasia44
-
Jackson - Colon Polyps to Cancer66
-
Cross - ID73
-
Howden - GERD27
-
Howden: PUD30
-
Howden - IBD33
-
Marino - Pathophys of Diarrhea44
-
Tombazzi - Carcinoid, GIST, Lymphoma36
-
Tombazzi - Vascular GI Disorders61
-
Bahouth - Diarrhea and Constipation28
-
Sweatman - Drugs for HCV/HBV32
-
Waters - Liver169
-
Sweatman - Tx for C. diff11
-
Bilal - Constipation/Megacolon39
-
Sweatman - Salivary Flow17
-
Howden - Acid-Suppressing Drugs32
-
Ryan/Nair - Hepatitis69
-
Ray - Malabsorption49
-
Tombazzi - Gallbladder56
-
Marino - Pancreas73
-
Sweatman - GI Cancer18
