GU Eval & Congenital Anomalies Flashcards
What would the indications for a renal eval be?
UTI’s – urinary tract infection
–
Increased BUN and or Creatinine
–
Hematuria
–
Mass seen on X-ray
–
Flank Pain, CVA tenderness
–
Decreased urine output – Oliguria
–
Azotemia - ↑ levels of nitrogen in the blood
Transducer frequency used for kideny US (adult, ped, newborn)
types.
3-5 Mhz. (adult)
–
4-5 Mhz. (peds)
–
6-8 Mhz. (newborn)
–
Vector
–
Sector
–
Curved Linear
•
Rib artifacts
What is renal ultrasound able to demonstrate?
The acoustic properties of a mass, delineate an abnormal lie of the kidney resulting from extrarenal mass, or determine whether hydronephrosis is secondary to renal stones
Patient postion Rt vs Lt
Right
–
Supine or Lt. lateral oblique or decubitus
•
Using liver as acoustic window
•
Imaging through muscles
–
posterior approach
•
Left
–
Supine or Rt. lateral oblique or decubitus
•
Spleen may be used as a window, generally upper pole only
•
Imaging through muscles
–
posterior approach
What are the Renal contours when imaged?
Smooth outer contours surrounded by reflected echoes of Perirenal fat. Renal parenchyma surrounds the fatty central renal sinus which contains the calyces infundibula pelvis vessels and lymphatics
US Appearance (adults vs infants)
ADULTS
Cortex; homogeneous, slightly less than liver echogenicity
•
Medulla-Pyramids; hypoechoic compared to cortex
•
Sinus; echogenic secondary to fat and fibrous tissue
INFANTS
Cortex; more echogenic than in adults
•
Medulla-Pyramids; more prominent than adults and often mistaken for cysts
•
Sinus; not well developed and almost absent – lack of adipose tissue
Why is the renal sinus imaged as an area of intense echoes with variable contours?
Because of the fat interface
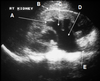
WHAT positon was this Td for this rt kidney?

long
What does dehydration do to the kidney?
Causes the infundibula and Renal pelvis to be collapsed making them indistinguishable from the echo dense renal sinus fat
what are the arrows pointing to?


What can you see if the bladder is hydrated?
The extrarenal pelvis medial to the kidney on transverse scans
how thick is the parenchyma? how about in the cortex?
Parenchymal thickness 1.5 cm or >
–
Even thickness throughout
–
Thin areas of cortex (< 1.5cm is pathologic)
What window is used to image the right kidney?
The liver
is the cortex or sinus more echogenic?
cortex
What window do you use to see the left kidney?
The liver or spleen
how much can a kidney move during inspiration?
~2.5 cm
What should the renal cortical echo amplitude be compared to with regards to amplitude and depth to set appropriate TGC and sensitivity?
Liver parenchymal echo amplitude
what poles does the kidney have?
superior and inferior.
What two parts of the kidney make up the renal Parenchyma?
The renal sinus to the outer renal surface
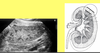
how can you tell this is a pediatric kidney?

the prominence of the medullary pyramids and the lack of prominence of the renal sinus as compared to the adult kidneys. (adult below)

What are the columns number Bertin?
The band of cortical tissue separating the hypo echoing medullary pyramids from the echogenic cortex
what can you see?

What normal structure could be confused for a renal artery and transverse?
The inferior vina cava. both will be tubular in transverse
what do you see?


What shape typically are renal pyramids?
Triangular
what is different about this kidney?

lack of sinus fat. prominence of medullary pyramids. *it’s an infants kidney

What vessels lie at the base of the pyramids?
The arcuate vessels
what do you see on this infant kidney


Why is it important for a sonographer to recognize variants?
So they do not suspect an abnormality when it is really a normal variation
what is this variant that is not uncommon and can be seen in some adults?

persistent fetal lobulation
What is a column Of Bertin made of ?
It is a prominent invagination of the cortex located at varying depths within the medullary substance of the kidneys
what do you see here?

Column of Bertin
–
A variant, not uncommon
–
Prominent cortex between the pyramids/Medulla. It is a normal variant. Can be found in either kidney.
–
Important to differentiate from a mass.
what is this variant that is typically seen in the lt kidney?

dromedary hump

Upper Tract Protocol (long, trans and extras)
Renal Longitudinal
Measure in longest plane – both sup. to inf. and ant. to post.
Medial aspect
Lateral aspect
–
Renal Transverse
Superior pole
Mid with measure – both med. to lat. and ant. to post.
Inferior pole
Additional images may be needed
Poles in longitudinal, if kidney is too long
Pathologies
protocol lower tracts (bladder, jets…)
Bladder Longitudinal
•
Mid line
–
Bladder Transverse
•
Mid way between dome and bladder neck
–
Additional images may be needed
•
Large bladder
•
Uretic Jets – Checking for urine flow into bladder
•
Pathologies
what is this showing you?
where to measure length. lateral, medial
what are anterior windows generally obstructed by when taking a long image of a kidney?
bowel and gas. henceforth many renal images are taken from lateral acoustic windows.

what do you do if you can’t get the poles in their entirety?
take additional images

what planes and parts of the kidney are these images taken in?

trans –> superior, middle, inferior

what planes are these images taken in?

transverse
what is this?

bladder

what are these?

lt and right uretic jets (image of the bladder)

what plane is this image taken from?
long rt kidney

Of the congenital anamoies:
Bilateral ______ is not compatible with life
–
Unilateral _______ is often an incidental finding. Pt. will have a large single kidney.
agenesis or hypoplasia
this congenital anomaly is Rare; Complete duplication of the kidney and ureter. Often duplication is within the pelvis.
supernumerary kidney
what congenital anomaly are these examples of?
Renal Ectopia – Kidney fails to rise into the normal expected location during development
–
Crossed renal ectopia – Condition where both kidneys are located on the same side.
–
Crossed fused ectopia – Condition where the kidneys are positioned on the same side and are fused together
malposition
what congenital anomay has –
Fusion of the upper poles or the lowers poles of the kidney. Most frequently occurs in the lower poles.

horseshoe kidney

what congenital anomaly is this?

horseshoe kidney
what is a collection system duplication (congenital anomaly)?

Dual collecting system
Two separate renal pelvi, one for upper pole and one for inferior pole
–
Two ureters coming from one kidney
May be the full ureter, and enter separately in the bladder
May be a incomplete ureter, and enter into the other ureter on the way to the bladder
*Important for sonographer to image in the renal pelvis to insure there is true duplication. It is easy to miss or to incorrectly diagnose as duplicated when it is not. Because of the way we image the collecting system. Sonographer must make sure the is two distinct collection systems, separated by cortex in the area of the hilum.
what do we see here?

eg of false positive duplication of the rt kidney (duplication of collecting system)

why does urine reflect color doppler?
why does blood reflect color doppler?
what about sterile water?
b/c of the salts and particulate matter within it.
RBC’s
? maybe just be show hypoechoic space?
____ is often associated w/ a duplicated collecting system
ureterocele

what does this image show?

extrarenal pelvis w/ NO dliation of collecting system
what congenital anomaliy does this image show?

peripelvic cysts
no dilation of collecting system, no communication of cysts. *cysts form in the renal sinus
What is the difference between crossed ectopia, crossed fused ectopia and an ectopic kidney?
what do these represent?
Crossed ectopia - same side of body
•
Crossed fused ectopic – same side of body, fused together
•
Ectopic Kidney – Kidney not located in the normal position. Often in pelvis
congenital anomalies

what is this an anomaly of? what is it?
what can happen in this site?

bladder anomaly
Diverticulum – pouch like projection from the bladder wall.
potential site for urinary stasis leading to stone formation or infections

what is exstrophy?

a bladder anomaly in which –
Failure of closer in anterior bladder wall of the urogenital sinus and genital tubercle.
Urogenital sinus
Genital tubercle

what is hypospadia?
Urethral opening on ventral side of penis

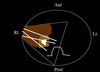
what vessels are used for anastomeses in the arterial, venous and ureter systems with regards to a renal transplant?
where do the native kidneys go?
Arterial – MRA to IIA or EIA, usually and end to end anastomosis.
–
Venous – MRV to EIV, usually end to side anastomosis.
–
Ureter – Implanted into the bladder, not into a ureter.
•
Location: annotate on the images
Rt. lower quad
Lt. lower quad
•
Native Kidneys – Typically left in place

these images represent the potential ways the kidney/vessles relationship can be due to patient’s pelvic anatomy.
what plane are these images taken from?
what quadrant of the body does this represent?

transverse
RLQ (renal transplant)
what would you evaluate in a pt shortly after a renal tranplant?
what about post biopsy?
in an older tranplant?
Decrease / Suboptimal function – Check for fluid collections, extrinsic compression
Pain, fever – Increasing pain
Drainage – Drainage does not decrease
POST – HematomA, AV fistula
OLDER - increasing labs and/or hematuria
if this image was taken in the RLQ is the dot medial or lateral to the kidney?
What about if it was taken in the LLQ?

medial
lateral
what is this?

subscapular hematoma w/i the true capsule of the kidney

what is going on w/ this 3 yr post renal transplant kidney?

A large stone can be seen in the superior / mid portion of the transplant. Did you notice the small amount of fluid in the upper pole of the collecting system demonstrated on the prior images?

where has this retroperitoneal hemorrhage taken place?
how can the sonographer tell the size fo the mass when there is not a clear image?

within Gerota’a fascia
by palpating the mass and increasing the depth to the full extent of the mass.

what are sonographers often asked to rule out in the event of a retroperitoneal hemorrhage?
a ruptured AAA.
in this eg The US was done prior to the CT. US was asked to r/o a ruptured AAA. After mass of identified the sonographer was able to see an AAA at the level of the umbilicus.

what is this? what do you need to be careful to not mistake it for?

–
Artificial Urinary Sphincter for bladder
•
Balloon reservoir can be seen adjacent to the bladder in pt. with this type of device

where are penile implants seen?
As with the artificial sphincter the balloon reservoir will be seen adjacent to urinary bladder

what do standard images of the kidneys include?
long w/ measurements
tran mid w/ measurement
trans inferior
the echogenicity of the renal pyramids are ___ compared to the renal echogenicity of the renal cortex?
slightly less
the cortical echogenicity of newborns kidneys are ofen ___ than adults?
more echogenic
Renal cortical thickness is an important to parameter to evaluate during a renal US exam. The normal cortical thickness is a minimum of ___.
1.5 cm
what anatomy are the arrows pointing to?
what is the location of the asterisk in relation to the poles of the kidney?
what is the echogenic area inferior to the asterisk and posterior to the arrows termed?

medulla or pyramid
superior pole
renal sinus

This patient has a condition known as hydronephrosis. The anechoic area in the center of the kidney is a dilatation of what?

renal collecting system
where is the renal hilum found?
on the medial border of the kidney
what is the echogenic area found w/i the kidney?
the renal sinus
what is the standard UIHC protocol for long images of teh kidneys 3 views?
a. Longitudinal with measurement
b. Longitudinal lateral
c. Longitudinal medial
what is the standard UIHC protocol for trans images of the kidneys 3 views?
a. Transverse of superior pole
b. Transverse mid with measurement
c. Transverse of inferior pole
A condition in which there is a dilatation of the urinary collecting system of a kidney is termed what?
what is an intrinsic and extrinsic cause for this?
hydronephrosis
Intrinsic: renal stone, blood clot
Extrinsic: pregnancy, ovarian cyst, uterine fibroids, pelvic tumors
if you can’t view the kidney from an anterior approach b/c the acoustic window is blocked by bowel or stomach, what else could you try?
Lateral approach, typically intercostal or posterior approach
The cortex of the kidney is measured from the true capsule to the cortico-medullary junction. Select an area where you would measure the cortical thickness.

name the areas

a. true capsule
b. column of Bertin
c. cortex
d. pyramid or medulla
e. minor calyx
f. major calyx
g. cortico-medullary junction
h. ureter
i. renal pelvis
j. hilum

name these areas

a. pyramid or medulla
b. sinus
c. column of Bertin
d. pyramid or medulla
e. rib shadows

name these

a. minor calyx
b. true capsule
c. major calyx
d. renal pelvis
e. ureter
what is notable about the echogenicity of this kidney?

Cortex is more echogenic than the liver/spleen
what can you say abou tthe cortical thickness of this kidney?

Cortex appears too thin
What is this an image of?
What plane was this image acquired in?
What can you tell about this patient?

urinary bladder
long
female patient, uterus seen posterior to bladder
what is this an image of?
what plane was it taken in?

urinary bladder
transverse
what is this an image of?
what can you say about this pt based on the image?

urinary bladder w/ lt ureteral jet. lt ureter is not totally obstructed. some uring is making it into the bladder
What is this an image of?
Can you identify the bladder wall?
Is the bladder wall thin?
What are some possible causes for this appearance of the bladder?

urinary w/ debris
yes - see image below
no. bladder wall appears thick
urinary infection of blood in bladder (causes of debris)

what can you say abou tthis kidney?

very echogenic
what does this image show?
can u identify where the transplanted kidney is located?

perfusion of the kidneys
LLQ
how many anatomoses are there for a kidney transplant? what are they?
3
The transplant renal artery to either the Native CIA, IIA or EIA
The transplant renal vein to either the Native CIV, IIV or EIV
The transplant ureter to the native bladder
name the 4 reasons why a renal transplant may be requested.
↑’ing Lab values
Pain
Fever
poor urine OP (output)
post bx (biopsy) to check for hematoma of AV fistula
Name the anatomic variant which characteristically appears as a prominent bulge on the superolateral border of the left kidney.
Dromedary hump
Name the anatomic variant which characteristically appears as a mass within the normal kidney. It consists of normal tissue but can displace the pyramids and calyces.
Hypertrophied column of Bertin
name each of these anatomic variables.

Column of Bertin - (appears as a mass within the normal kidney. It consists of normal tissue but can displace the pyramids and calyces.)
Dromedary hump (prominent bulge on the superolateral border of the left kidney.)

Lines a-c represent the standard protocol planes for the longitudinal images. How would letter c be annotated (labeled) on the US image?
how about letter b?
which kidney is shown in the drawing?
how do you know?

medial longitudinal
lateral long
rt kidney
the renal hilum is medial

what approach was used to image this kidney?
anterolateral
what is contained in the prominent hump of the normal variant on the lateral askpect of the lt kidney aka the dromedary hump?
renal parenchyma
__ is found b/t the renal pyramids?
cortex
There will most likely be some size discrepancy between the two kidneys within a patient. How much size discrepancy is allow before the Radiologist will call a potential problem?
5-10cm
what type of kidneys have lumpy countour, hypoechoic renal pyrmaids and echoegenic renal cortex as compared to the adult renal echogenicity?
newborn kidney
what are the columns of bertin made of?
bands of cortical tissue. It is a prominent invagination of the cortex located at varying depths within the medullary substance of the kidneys
what could the column of bertin be difficult to differentiate from?
avascular neoplasm
when are the columns of bertin more exaggerated?
when a person has complete or partial duplication
how would a column of bertin affect the renal sinus on US?
it produces a lateral indentation of the renal sinus, a clear definition from the renal sinus or a max dimension that does not exceed 3 cm.
what is a dromedary hump?
what is believed to cause this?
bulge of corcical tissue on the lateral surface (usaually lt) of the kidney caused by splinci impression onto the superolateral kidney.
fetal lobulations are frequently seen in kids (up to 5 yyrs) and may be persistent in up to 51% of adults. what are they?
surface of the kidneys are indented in b/t the clyces giving the kidneys a slightly lobulated appearance
what is hydronephrosis?
what can it be associated with?
water inside the kidney causing distension or dilation
a duplex collecting system upper pole as well as upper and lower pole calyces.
how can you distinguish b/t complete and incomplete dulplex collecting systems on US?
in a complete duplex collecting system you will see 2 ureteral jets entering the bladder on the same side. the duplex kidney is usually enlarged w/ smooth margins and the renal sinus appears as 2 echogenic regions separated bya cleft of moderately echogenic tissue similar to normal renal parenchyma (in long)
what is a ureterocele
a cystlike enlargement of the lower end of the ureter caused by congeintal or acquired stenosis of the distal end of the ureter. usually small and asymptomotic otherwise cause obstruction and infection of upper urinary system. if lg may cause bladder outlet obstruction. cobra head ppearance in US
how does a US demonstrate urine entering the bladder and where?
flashes of doppler color entereing at the lateral posterior border fo the bladder coursing superior and medial.
what is renal compensatory hypertrophy?
where the functioning kidney enlarges to make up for the absence of a kidney or a thailure of akidney to form aka renal agenisis.
why might you see renal compensatory hypertrophy/
in cases of renal agenesis (solitary kidney)
hydronephrosis
Unilateral hydronephrosis Hydronephrosis; Chronic hydronephrosis; Acute hydronephrosis; Urinary obstruction Last reviewed: April 16, 2012. Unilateral hydronephrosis is swelling of one kidney due to a backup of urine. See also: Bilateral hydronephrosis Causes, incidence, and risk factors Hydronephrosis (kidney swelling) is a condition that occurs with a disease. It is not a disease itself. Conditions that are often associated with unilateral hydronephrosis include: Acute unilateral obstructive uropathy Blockage of a ureter due to scarring, tumor, urinary stones Chronic unilateral obstructive uropathy Vesicoureteric reflux (backflow of urine from bladder to kidney) Nephrolithiasis (kidney stones) Hydronephrosis that occurs without a known cause during pregnancy Unilateral hydronephrosis occurs in approximately 1 in 100 people. Symptoms Flank pain Abdominal mass Nausea and vomiting Urinary tract infection Fever Painful urination (dysuria) Increased urinary frequency Increased urinary urgency Note: Sometimes unilateral hydronephrosis does not have symptoms. Signs and tests
