CKD Flashcards
(48 cards)
define CKD
Impaired renal function for >3 months based on abnormal structure/function, or GFR <60ml/min for >3 months with/out evidence of kidney damage.
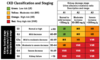
outline stages of CKD
- note that for stages 1 and 2 evidence of kidney damage is needed! E.g. proteinuria, or abnormalities on scanning
- stages 3-5 are defined by GFR alone
- stages 1-3 are common, whereas 4-5 are not

staging : G and A
starting dialysis
- there is an argument to leave it for as long as possible
- most patient need ≤8.8 ml/min
management of CKD in GP
- commonly co exists with eg heart failure and diabetes - screen high risk groups
- urinalysis
- proteinuria must be quantified - spot urine sample
- increases the risk of progression to CKD
- referal
- identify and treat CV risk factors

which GN typically progresses to CKD
IgA nephropathy - 25% in 10-30 years
causes
- Diabetes: type 2>1
- Glomerulonephritis: commonly IgA nephropathy
- Unknown
- Hypertension or renal vascular disease
- Artery walls are thickened and narrowed, meaning less blood and oxygen gets to the kidneys. Ischaemic injury and glomerulosclerosis – diminished ability to filter blood.*
- Falling GFR activates RAAS, causing further hypertension.*
- Vicious cycle.*
- Renal artery stenosis
- Ischaemia/hypertensive nephrosclerosis
- Microangiopathic e.g. HUS/TTP
- Polycystic kidneys
- Pyelonephritis and reflux nephropathy
- Small vessel vasculitis
- Tubulointerstitial:
- Nephritis – uveitis
- ADPKD
- Reflux nephropathy
- Post-renal (obstructive)
risk of CKD after AKI
- After AKI some tubules are lost, meaning that the other nephrons hyperfilter in order to take up the efforts of the lost nephrons. This compensation means the creatinine returns to normal but as the remaining nephrons are working harder they burn out quicker
- Therefore, there is a risk of CKD developing or progressing, and patients must be informed of this after AKI
- Patients must be monitored for the development or progression of CKD after AKI episode for 2-3 years, even if the serum creatinine has returned to baseline
first line management of a person with kidney damage presenting with loin to groin pain
insert a catheter - may relieve obstruction if it is below bladder level
screening
important, all high risk patients are screened
test criteria
minimum of 2 samples at lest 90 days apart
eGFR
- estimates GFR
- MDRD4 equation: takes into account serum creatinine, sex, age and ethnicity
- correction factor for women and black race
muscle masse effects on creatinine measuremente of GFR
- Over-estimates GFR is muscle mass is low
- Under-estimates if muscle mass high
- Only valid if serum creatinine is stable
how does pregnancy effect GFR
it tends to increase during pregnancy
cystatin C
- protein that can be used to estimate GFR
- useful when a previous kidney function test was inconclusive or needs confirmed, or in overweight, elderly of muscly patients
eGFR 3a, eGFR cystatin C >60ml/min and no other evidence of kidney disease - CKD?
no
define accelerated progression of CKD
- Sustained decrease in GFR ≥25% and a change in GFR category within 12 months OR
- Sustained decrease in GFR of 15ml/min/1.73m2 per year
risk factors for CKD progression
- CVD
- PROTEINURIA – more likely to progress
- YOUNGER – longer to progress
- AKI
- Hypertension
- Diabetes
- Smoking
- African, Afro-Caribbean or Asian family origin
- Chronic use of NSAIDs
- Untreated urinary outflow tact obstruction
what are the 4 principles of management
- Slow progression
- Reduce CV risk
- Identify and treat complications of CKD
- Prepare for RRT
- slow progession
control BP and reduce proteinuria
- BP: aim for <140/90 mmHg, or <130/80mmHg in those who also have DM/ACR>70
- ACEi
- reduce proteinuria and BP
- good glycaemic control in DM
- stop smoking
what is expected when initially commencing an ACEi
- reduce filtration pressure - small fall in GFR and rise in creatinine
- fine if GFR decrease <25% and serum creatinine increase <25%
- watch out for hyperkalaemia
- reduce CV risk
BP, proteinuria, smoking, statins
- offer atorvastatin 20mg
symptoms of advanced uraemia
- Yellow tinge
- Involuntary muscle twitching
- Encephalopathic: flapping tremor and confusion
- Pericardial rub or haemorrhagic pericardial effusion (pericarditis)
- Kussmaul breathing due to metabolic acidosis
- The kidney normally excretes H+ ions
- increased anion gap
- bleeding
- uremic frost
why does uraemia cause bleeding
- Uremia acts as an antiplatelet, less clot formation, meaning patients bleed and bruise more easily
