Neck/Head/Thorax/Spine/Abdomen Flashcards
Sternocleidomastoid
ACTION
Bilateral: - flex head against resistance -neck flexion -extension at the A-O joint (posterior fibers only) -accessory muscle of respiration
Unilateral: -ipsilateral sidebend with contralateral rotation of the face
PROXIMAL: Sternal head: manubriu, Clavicular head: upper medial 1/3 clavicle DISTAL: to lateral surface of mastoid process & lateral 1/2 superior nuchal line
INNERVATION: CN XI (motor); C2, C3 ventral rami (sensory)

Anterior, Middle, Posterior Scalenes
ACTION
- Ipsilateral sidebending of cervical vertebra
- Reverse action: elevate first and second rib during inspiration
PROXIMAL
Anterior: transverse process CV3-CV6
Middle: post tubercles transverse process CV5-CV7
Posterior: post tubercles transverse process CV5-CV7
DISTAL
Anterior: 1st rib
Middle: sup surface 1st rib
Posterior: 2nd rib
INNERVATION
Anterior : C4-C6 ventral rami
Middle : ventral rami C3-C8
Posterior : ventral rami C7, C8

Levator Scapulae
ACTION
- Elevates scapula
- downward rotation of scapula with pec minor ms
PROXIMAL
-Posterior tubercles transverse processes of from CV1-CV4
DISTAL
-To medial border of scapula at & above the spine
INNERVATION
-C3-4 ventral rami; C5 ventral rami from dorsal scapular n.

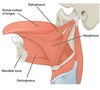
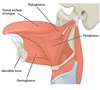
Platysma
ACTION: depresses mandible and tenses skin of inferior face and neck
-Superficial to investing layer of fascia
INNERVATION: CN VII

Investing layer of fascia
Surrounds:
- trapezius
- sternocleidomastoid
- acts as roof to anterior triangle of neck

Pretracheal Fascia
Surrounds:
- thyroid gland
- infrahyoid (aka strap) muscles
- trachea
- esophagus (located deep to the trachea)

Prevertebral Fascia
Surrounds:

Prevertebral muscles, longus colli, longus capitus, Scaleni Musculature, Anterior Scalene, Middle Scalene, Posterior Scalene, Levator scapulae, Phrenic nerve, Deep muscles of the back
*Forms the floor of the posterior triangle
AKA: Fascial Carpet/ Floor
*prolonged laterally by forming the axillary sheath which invests the brachial plexus & vessels
Carotid Sheath
Surrounds:
- common carotid & int carotid artery
- internal jugular vein
- vagus nerve (CN X)
- sometimes ansa cervicalis (part of cervical plexus innervating strap muscles)
–> At times may lie superficial to carotid sheath
Anterior Triangle Borders
- roof- investing fascia & platysma
- superior- inferior border of the mandible
- anterior- median line of the neck
- posterior- anterior border of SCM
- Floor-prevertebral fascia

Anterior Triangle Contents
- muscular triangle: infrahyoid muscles, thyroid & parathyroid glands
- carotid triangle:common carotid a., internal jugular v., portions of last 3 cranial nerves
- digastric triangle: submandibular gland, facial artery, internal carotid a., internal jugular v., CN IX, CN X
Strap Muscles
Innervated by: ansa cervicalis of cervical plexus

- Sternohyoid
- Sternothyroid
- Thyrohyoid
- Omohyoid
Posterior Triangle Borders
- roof- fascia & platysma
- anterior- posterior border of SCM
- posterior- anterior border of trapezius muscle
- inferior- superficial aspect middle 1/3 of clavicle
- floor- prevertebral fascia

Posterior Triangle Contents
- transverse cervical a.
- CN XI
- upper trunk of brachial plexus
- subclavian a.
- dorsal scapular n.
- long thoracic n.
- n. to subclavius
- suprascapular a. & n.
Branches off of the subclavian A.
- Vertebral
- Internal thoracic
- Thyrocervical trunk which gives rise to 3 arteries: inferior thyroid, suprascapular, transverse cervical
- Costocervical trunk
- Dorsal scapular
Cervical Plexus
- formed by branches of ventral rami C1-4
- Supplies:
Nuchal (neck) muscles
diaphragm muscle
infrahyoid (strap) musculature
skin of head/neck/chest
-superficial branches (sensory only):
lesser occipital n. - C2
great auricular n. - C2,3
transverse cervical n. - C2,3
supraclavicular n. - C3,4
-Deep branches include:
Motor to prevertebral ms. - ventral rami C1-4
Motor to levator scapula and ant, middle, post scaleni
Motor to infrahyoid muscles via ansa cervicalis – ventral rami C1-3
Motor & sensory to diaphragm via the phrenic n. - C3-5 ventral rami
Sensory to SCM & trapezius- ventral rami C2,3 (NOT MOTOR, ARE SENSORY) (pain & proprioception)

Ansa Cervicalis
- that supplies the infrahyoid muscles (strap ms.)
- C1-3 ventral rami
- consists of two loops (aka roots)
- innervates: sternohyoid, sternothyroid, omohyoid, thyrohyoid
- innervation thyrohyoid: C1 ventral ramus however rides along with the hypoglossal nerve
Infrahyoid muscles
aka strap muscles
- anchor hyoid bone to sternum, clavicle & scapula
- action-depress hyoid bone & floor of mouth; elevate or depress larynx
- innervated by ansa cervicalis
- {thyrohyoid specifically C1 via CN XII}

Suprahyoid musucles
- digastric
- geniohyoid
- stylohyoid
- mylohyoid

Digastric
ACTION: depress mandible; elevates hyoid during swallowing
ATTACHMENT: Anterior and posterior bellies, from the digastric fossa of the mandible and the mastoid notch of the temporal bone to the intermediate tendon to body and greater horn of hyoid bone
INNERVATION: CN V/anterior belly,CN VII/posterior belly
**suprahyoid ms**

Geniohyoid

ACTION: depress mandible; elevates hyoid
ATTACHMENT: from the inferior mental spine of the mandible to the body of the hyoid
INNERVATION: C1 via CN XII
**suprahyoid ms**

Stylohyoid
ACTION: draws hyoid posteriorly & elevates it
ATTACHMENT: superior to post belly digastric, from the styloid process of the temporal bone to the body of they hyoid, superior!!!
INNERVATION: CN VII
**suprahyoid ms**

Mylohyoid

ACTION: elevates hyoid and floor of mouth
ATTACHMENT: mylohyoid line of the mandible and the mylohyoid raphe on the body of the hyoid one. , makes up floor of mouth
INNERVATION: CN V3 = mandibular br. of trigeminal n.
**suprahyoid ms*

External Carotid Artery Branches
- superior thyroid a.
- ascending pharyngeal a.
- lingual a.
- facial a.
- occipital a.
- posterior auricular a.
- superficial temporal a.
- maxillary (gives rise to meningeal a.)

Cranial Nerve VII (Facial Nerve)
PATH: cellbodies originate in pons and medulla–>through internal acoustic meatus and facial canal–> exits stylomastoid foramen
RESPONSIBILITIES:
- Motor supply to the muscles of facial expression
- (Bell’s Palsy-paralysis of muscles of facial expression; no apparent etiology/idiopathic; suspect edema 2’ infection)
- Motor: stylohyoid and posterior belly of digastric ms.
- Parasympathetic innervation (motor): secretion of tears (lacrimal gland) and saliva (sublingual and submandibular salivary glands)
- Special sensory: taste to anterior 2/3 of tongue and palate
To Zanzibar By Motor Car
- temporal
- zygomatic
- buccal
- mandibular
- cervical
*Most frequently paralyzed cranial nerve containing motor fibers*
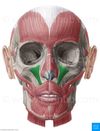
Muscles of Facial Expression
- Obicularis Occuli
- Occipitofrontalis
- Corrugator Supercilli
- Procerus
- Nasalis
- LLSAN
- Levator Labii Superioris
- Zygomaticus Minor and Major
- Levator Anguli Oris
- Buccinator
- Mentalis
- Depressor Labii inferioris
- Depressor anguli oris
- Orbicularis oris
- Platysma
Orbicularis Oculi
ACTION: Closes eyelids
INNERVATION: CN VII

Occipitofrontalis
ACTION: raises eyebrows & wrinkles skin of forehead; protracts (pulls back) scalp
INNERVATION: CN VII

Corrugator supercilli
ACTION: draws eyebrows medially & down
INNERVATION: CN VII

Procerus
ACTION: depresses medial eyebrow; makes transverse wrinkle in forehead
INNERVATION: CN VII

Nasalis
ACTION: widens nasal aperture during deep inspiration
INNERVATION: CN VII

Levator labii superioris alaeque nasi (LLSAN)
ACTION: everts upper lip and dilates nostrils
INNERVATION: CN VII

Levator labii superioris
ACTION: elevates & everts upper lip
INNERVATION: CN VII
Zygomaticus minor and major
ACTION: elevate upper lip; retract buccal angle, smile!
INNERVATION: CN VII

Levator Anguli Oris
ACTION: raise the buccal angle , one layer deep to levator labii and zygomaticus
INNERVATION: CN VII

Buccinator
ACTION: compress the cheeks against the teeth(eccentric) &/or expelling air when cheeks distended (concentric)
*Deep*
INNERVATION: CN VII

Mentalis
ACTION: wrinkles the chin skin
INNERVATION: CN VII

Depressor Labii Inferioris
ACTION:depresses the lower lip; assist in lower lip eversion
INNERVATION: CN VII

Depressor anguli oris
ACTION: depresses the buccal angle laterally
INNERVATION: CN VII

Orbicularis Oris
ACTION: closes/purses/protrudes the lips, different from obicularis occuli
INNERVATION: CN VII

CN VII Impairments
- If the lesion is near the origin of the nerve or its pathway distally it results in:
- Ipsilateral paralysis of facial & scalp muscles: unable to close the eye; angle of the mouth droops: forehead does not wrinkle
- Loss of taste to anterior 2/3 tongue and palate
- Impairments in secretion of tears and saliva
**Most frequently paralyzed cranial nerve containing motor fibers**
Bell’s Palsy-paralysis of muscles of facial expression; no apparent etiology/idiopathic; suspect edema 2’ infection
Cranial Nerve V (Trigeminal)
PATH: Pons and semilunar (aka trigeminal) ganglion
BRANCHES:
- V1-ophthalmic-primarily sensory
- V2-maxillary-primarily sensory
- V3-mandibular-sensory and motor
RESPONSIBILITIES:
- sensation to face, anterior half of scalp, teeth, mouth, nasal cavity
- motor supply to muscles of mastication
Opthalmic Nerve (V1 of CN V)
PATH: exits cranial vault through superior orbital fissure
BRANCHES:
-lacrimal n.-innervates lacrimal gland (sensory)–>
sensory to conjunctiva(whites of eyes) & skin of upper lid
-frontal n.-divides into supraorbital & supratrochlear ns.->
Supplies sensation forehead, scalp, upper lid, frontal sinus
-Nasociliary n.-major branches = long & short ciliary nerves- will only see on prosection
Contains: sympathetic fibers (not V1 fibers, just take a lil ride) to dilator pupillae; catches a ride with short ciliary nerves
- afferent fibers (sensory) from cornea, skin of eyelid & nose, lacrimal sac, & sinuses
- responsible for the sensory portion of the corneal reflex
- (CN VII responsible for the blink of the eye or the motor response… what muscle?)
- Infratrochlear n.
- Ethmoidal n.
Horner’s syndrome
**Issue with Opthalmic branch of CN V**
-combination of drooping of the eyelid (ptosis) (from paralysis of smooth (tarsal ms (symph) that interdigitate with the levator palpebrae superioris) and constriction of the pulpil (miosis)
-sometimes accompanied by decreased sweating (anhidrosis) of the face on the same side
- redness of the conjunctiva (white of eye) of the eye
- Apparent enophthalmos [posterior displacement of the eyeball within the orbit due to changes in the volume of the orbit (bone) relative to its contents (the eyeball and orbital fat), or loss of function of the orbitalis muscle.]
- indicates problem with the sympathetic nervous system, Medical imaging and response to particular eye drops may be required to identify the location of the problem and the underlying cause.
Maxillary Nerve (V2 of CN V)
PATH: exits foramen rotundum to inferior orbital fissure
BRANCHES:
-infraorbital n.
-meningeal n.
-alveolar ns.
-zygomatic n.- divides into zygomaticotemporal and zygomaticofacial ns.
-Sensory only: supplies skin of face over maxilla, upper lip, maxillary teeth, nose mucosa, maxillary sinus, and palate
Mandibular Nerve (V3 of CN V)
PATH: exits cranial vault through foramen ovale - to temporal fossa
RESPONSIBILITIES: sensation to skin over mandible, teeth/gums of mandible; skin of temporal region; general sensation to ant 2/3 tongue and oral mucosa ; TMJ & motor supply to ms. of mastication—not taste! Just general sensation
- Anterior branch - chiefly motor to mastication:
- Posterior branch- chiefly sensory
branches include auriculotemporal n, buccal n, lingual n (general tongue sensation), & inferior alveolar n. (ends as mental n.)
Trigeminal Neuralgia (Tic Douloureux)
- aka: Tic Douloureux
- Idiopathic trigeminal neuropathy(dysesthesia) (usually sensory in nature)
- Excruciating pain usually along V2 and V3 distribution, chronic pain along V2, V3 until this irritation subsides, can be disabling
- Cause Unknown: ? Vasculature anomaly that compresses CN V maybe
- Treatment: nerve block if long term and chronic; medication, some surgical interventions
Muscles of Mastication
- Masseter
- Temporal
- Medial pterygoid
- Lateral pterygoid
*innervated by CN V (trigeminal), V3 mandibular branch
Masseter
ACTION: powerful elevator of mandible
PROXIMAL: arises from inferior border & med surface of zygomatic arch
-Arch includes zygomatic bone & temporal bone
DISTAL: to the angle and lateral aspect of ramus of mandible
INNERVATION: mandibular branch of CN V (V3)

Temporalis Muscle
ACTION:
- anterior fibers-elevation of mandible (to close mouth & teeth)
- posterior fibers-retract mandible
PROXIMAL: arises from floor temporal fossa & deep temporal fascia
DISTAL: to medial surface, apex, anterior & posterior borders of coronoid process of mandible, & anterior border of ramus of mandible
INNERVATION: mandibular branch of CN V (V3)

Lateral Pterygoid (2 heads)
ACTION: chief protractor; depresses mandible
-Pulls whole articular disc forward, pulling condyle forward which protracts and depresses
PROXIMAL:
- upper-infratemporal surface & crest of greater wing of sphenoid
- lower-lat surface of lat pterygoid plate
DISTAL: ant aspect mandibular neck, articular capsule & TMJ disc
INNERVATION: mandibular branch of CN V (V3)

Medial Pterygoid (2 heads)
ACTION: elevate mandible; protraction of mandible
PROXIMAL: med surface of the lateral pterygoid plate & palatine bone & tuberosity of maxilla
DISTAL: medial surface of mandibular angle
INNERVATION: mandibular branch of CN V (V3)

Movements of Mandible
Elevation: temporalis, masseter, med pterygoid
Depression: lat pterygoid, digastric
Protraction: (protrusion/mandible comes forward)
Lat pterygoid: (prime mover) & med pterygoid
Retraction: (mandible comes backward)
Temporalis: (post fibers)
Lateral Movements
- Ipsilateral:* temporalis & masseter (pull)
- Contralateral:* med & lat pterygoid (push)
- Meaning to move your jaw to your right*: contract R temporalis, R masseter, L medial and L lateral pterygoid

Intratemporal Fossa
§Irregularly shaped deep space located:
- Inferior to the zygomatic arch
- deep to the ramus of the mandible and
- posterior to the maxilla bone
Contents
- Temporalis ms. (Inferior aspect)
- Med and Lat Pterygoid mm.
- Maxillary a. (coming off of external carotid artery) & venous plexus
- Nerves: mandibular, inferior alveolar, lingual, buccal, chroda tympani and otic ganglions
*took out zygomatic arch in this picture*

Temperomandibular Joint (TMJ)
- Diarthrodial (synovial) joint- has joint capsule,
- With synovial fluid that bathes and takes care of itself
- articulation between:
- articular tubercle & mandibular fossa of
temporal bone (in pink)
- & mandibular condyle of mandible (grey)
- complex- bc of articular disc, disc divides joint into 2 separate compartments
- Protraction and retraction occur in the superior compartment
- Elevation and depression occur in the inferior compartment
- To depress mandible: the head of the mandible and articular disc must move anteriorly on the articular surface until the head lies inferior to the articular tubercle
- Loose joint capsule
- Shape- classified differently depending on reference: modified hinge (Moore & Dalley) or bicondylar
Innervation: V3

TMJ Ligaments
•Lateral temporomandibular lig: Thickening of the joint capsule, Prevents posterior dislocation of the jt with the postglenoid tubercle
- Sphenomandibular lig: Connects the lingula of mandible to the cranium via the spine of the sphenoid bone
- Stylomandibular lig: Connects the mandible to the cranium via the styloid process of the temporal bone

TMJ Pathology
Dislocation:
- Posterior: not common
- Anterior (excessive contraction of lat ptyergoids while opening mouth); mandible stays depressed and unable to close mouth
- Clicking: delayed movement of the disc; may indicate tear of disc
Innervation: V3

Extraocular Muscles
Levator palpebrae superioris-elevates upper eyelid
- CN III (oculomotor)
Orbicularis occuli -closes eyelid
-CN VII
Medial Rectus-adduction of eyeball (towards nose)
-CN III (oculomotor)
Lateral Rectus-abduction of eyeball (towards ear)
-CN VI (abducens)
Superior Rectus-elevate eyeball not lid!, adducts (simultaneously), med rotates(intorsion) eyeball
-CN III
Inferior Rectus-depress, adducts, lat rotates(extorsion) eyeball
-CN III
Superior Oblique-depress, abducts, med rotates eyeball (down & out)
-CN IV (trochlear n.)
Inferior Oblique-elevate, abducts, lat rotates eyeball (up & out)
-CN III (oculomotor n.)
LR6 SO4 The rest are 3!
*No one muscle rotates extorsion/intorsion-always combo with other movements*

Levator Palpebrae Superioris
ACTION: elevates upper eyelid
PROXIMAL: Inferior aspect of lesser wing of sphenoid bone
DISTAL:Superior tarsal plate and skin of upper eyelid
INNERVATION: CN III

Medial Rectus
ACTION: adduction of eyeball (towards nose)
INNERVATION: CN III (oculomotor)

Lateral Rectus
ACTION: abduction of eyeball (towards ear)
INNERVATION: CN VI (abducens)

Superior Rectus
ACTION: elevate eyeball not lid!, adducts (simultaneously), med rotates(intorsion) eyeball
INNERVATION:CN III
Inferior Rectus
ACTION: depress, adducts, lat rotates(extorsion) eyeball
INNERVATION: CN III

Superior Oblique
ACTION: depress, abducts, med rotates eyeball (down & out)
INNERVATION: CN IV (trochlear n.)
**Trochlea changes line of pull of superior oblique- so when it tightens, it flips the eyeball down- down bc pulls towards the trochlea

Inferior Oblique
ACTION: elevate, abducts, lat rotates eyeball (up & out)
INNERVATION: CN III (oculomotor n.)

Lesion of CN VI
- Denervation of lateral rectus ms.
- gaze directed medially
Lesion of CN IV
- Denervation of superior oblique muscle
- cannot depress the eye when eye adducted (eg during convergence when reading or going down stairs; double vision) when going downstairs or looking down at book
LEsion of CN III
- Denervation of: levator palpebrae superioris, superior rectus, inferior rectus, medial rectus, inferior oblique
- gaze directed down & laterally b/c only muscles left innervated (LR & SO) produce down and out
Ptosis of the eyelid (droopy eyelid bc levator palpaebrae superioris denervated) & consistent dilated pupil
- CN III responsible for parasymph fibers to sphincter of pupil
- Pupillary reflex lost- sympa fibers dilate pupil, hooked ride with nasocilliary ns (branch of V)
- CN III constricts pupil so if that’s impaired then reflex would be lost
Genioglossus
ACTION: (bilateral) tongue protrusion or protraction (principal muscle); curls the tongue in a circle: unilateral action causes deviation to opposite side
–R genioglossus contraction causes tongue to go to left (b/c the muscle pushes the tongue out to left)
INNERVATION: CN XII

Hyoglossus
ACTION: depresses tongue
Innervation: CN XII
Styloglossus
ACTION: tongue retraction
INNERVATION: CN XII
CN XII Lesions
-CN XII Paralysis-when asked to stick tongue out in midline…deviates to paralyzed side
*(First think of the action: One genioglossus ms. working alone pushes the tongue to the opposite side)
-R XII lesion: when you ask the patient to stick out their tongue, it deviates to the right (b/c the left genioglossus is working alone)

Thorax
- Lodges the heart & lungs
- Skeletal framework comprised of:
- thoracic vertebrae
- intervertebral discs
- ribs
- costal cartilage
- sternum
- Superior thoracic aperture (thoracic inlet)
- Inferior thoracic aperture (thoracic outlet)

Ribs
- 12 paired ribs which protect thoracic & abdominal contents
- increase in length from 1-7; decrease in length 8-12
- 1-7 true ribs connected to sternum by costal cartilage
- 8, 9, 10 join costal cartilage above
- 11, 12 “floating ribs” do not connect to sternum or costal cartilage; but are attached at the costovertebral joints of course!
- Identify: head, neck, tubercle, body, angle of rib
- TV1: articulates with rib 1 superiorly and rib 2 inferiorly

Thoracic Outlet Syndrome
*This area is referred to as the thoracic inlet, but clinically, its referred to as thoracic outlet syndrome, UM OK Y THO?

- signs & symptoms in the head, neck, & arm due to neural or arterial compression in the neck (scalenus anticus syndrome, cervical rib etc.)
- TOS: garbage bucket term for involvement of nerves, arterial & venous supply to UE that results in pain, numbness, tingling, weakness in arm chest, neck
- Causes: anatomical variations, physical trauma, tumors, poor posture, repetitive arm movements, sports.
Abdomen
- Abdominal cavity lies between the thorax & pelvis
- contains most of the digestive system & part of the urogenital system
Anterolateral Abdominal Wall
- 2 recti abdomini anteriorly
- Laterally: external oblique, internal oblique, transversus abdominus ms. (superficial to deep)
- each separated by a layer of fascia
- fascia covering the abdominal wall=Ext Oblique fascia

Thoracoabdominal Nerves
- T7-T11 intercostal nerves (Intercostal nerve underneath each rib [ventral ramus in thoracic region]) change their name as they leave the rib space and turn into thoracoabdominal ns.
- Innervate muscles of the lateral and anterior abdominal wall
- Provide Sensation-via cutaneous branches that pierce the Anterior Rectus sheath & lateral wall
- are ventral rami with both motor and sensory responsibilities
**12th ventral ramus below the last rib, cant be intercostal n, is a T12 ventral ramus**

External Intercostals
ACTION: *Still controversial however evidence suggests it elevates the rib
PROXIMAL:From lower margins of ribs 1-11; fibers pass down & forwards
DISTAL:
To upper margins of rib below
N.B. Extend from tubercles of the rib (post); at costal cartilage become membranous and continues as membranous until the costochondral junction (ant)
INNERVATION: Corresponding intercostal ns.

Internal Intercostals
ACTION:Depress the rib; generally considered to be a muscle of expiration
PROXIMAL: From lower margins of the ribs & costal cartilages & floor of costal groove; pass down and back
DISTAL: To the upper margins of subadjacent ribs & costal cartilages
N.B. Extend from sternum ant, to angle of the rib laterally & continue as internal intercostal membrane posteriorly
INNERVATION: Corresponding intercostal n.
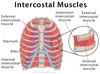
Innermost Intercostals
ACTION: Depress the rib; generally considered to be a muscle of expiration
PROXIMAL: From internal aspects of adjoining rib, May be absent at high levels
DISTAL: Fibers run in the same direction as internal intercostal muscles but not the full length of the rib (~middle 1/3)
INNERVATION: Corresponding intercostal ns.

External Oblique
ACTION:
- All abdominal muscle together-increase intra-abdominal pressure, hence resist downward pressure of the diaphragm during straining & coughing;
- R sidebending with R IO;trunk flexion & L rotation with R EO & L IO
PROXIMAL: From external surface of the lower 8 ribs
DISTAL:To external lip of the iliac crest, pubic tubercle, and linea alba
*hands in a pocket!
INNERVATION: Thoracoabdominal nn.(T7-T11) &subcostal ns.

Internal Oblique
ACTION:
- All abdominal muscle together-increase intra-abdominal pressure, hence resist downward pressure of the diaphragm during straining & coughing;
- R sidebending with R IO; trunk flexion & L rotation with R EO & L IO
PROXIMAL: From thoracolumbar fascia, iliac crest (intermediate line), lateral 1/2 of inguinal ligament
DISTAL: Up towards the lower 3 ribs & costal margins, linea alba and down toward the pubis via conjoint tendon
*Reverse hands in a pocket!
INNERVATION: Lower 2-3 thoracoabdominal ns (T7-11)., subcostal n., & (L1 ventral ramus)

Transverse Abdominus
ACTION: All abdominal muscle together-increase intra-abdominal pressure, hence resist downward pressure of the diaphragm during straining & coughing;
PROXIMAL: From fascia iliaca, iliac crest (internal lip), thoracolumbar fascia, & inner surfaces of lower 6 costal cartilages. Lateral 1/3 of inguinal ligament
DISTAL: To aponeurosis that contribute to rectus sheath & pubis via conjoint tendon
*Horizontal fibers!
INNERVATION: Thoracoabdominal ns (T7-11). &subcostal n., & L1 ventral ramus

Rectus Abdominus
ACTION:
- All abdominal muscle together-increase intra-abdominal pressure, hence resist downward pressure of the diaphragm during straining & coughing;
- Flex the lumbar vertebral column if pelvis fixed; if thorax is fixed, they flex lumbar vertebral column & draw pelvis up
PROXIMAL: From xiphoid process of sternum & costal cartilages 5-7
DISTAL: To pubic crest & symphysis
INNERVATION: Thoracoabdominal ns. (T7-11 &subcostal n.

Pelvis

Diaphragm
ACTION: Primary muscle of inspiration
-During contraction the diaphragm descends & draws central tendon down; volume of thorax is increased & intrathoracic pressure decreased
PROXIMAL:
- Sternal-from post aspect of xiphoid process
- Costal-from inner surfaces of lower 6 costal cartilages & lower 4 ribs
- Lumbar-from bodies of upper lumbar vertebrae and fibrous arches (med &lat arcuate ligaments)
DISTAL: To central tendon of diaphragm
INNERVATION: Phrenic n. (C3,4,5, keep the diaphragm alive!)

Linea Semi Lunaris
curved vertical line at the lateral edge of the recti

Rectus Sheath
Anterior rectus sheath (above arcuate line) comprised of:
- aponeurosis of E.O.
- 1/2 aponeurosis of I.O.
Posterior rectus sheath (above arcuate line) comprised of:
- 1/2 aponeurosis of I.O.
- Aponeurosis of T.A.
*Deepest structure but not part of Rectus sheath=transversalis fascia followed by peritoneum
arcuate line (linea semicircularis)- a horizontal line on post rectus sheath which demarcates a point where all of the aponeuroses (EO, IO, TA) pass anterior to rectus abdominus ms.

Linea alba
vertical midline structure between recti, stretching from xiphoid process to pubic symphysis

Anterior rectus sheath
- above arcuate line, comprised of:
- aponeurosis of E.O.
- 1/2 aponeurosis of I.O.
Posterior Rectus Sheath
Above arcuate line, comprised of:
- 1/2 aponeurosis of I.O.
- Aponeurosis of T.A.

Transversalis fascia
- Deepest structure but not part of Rectus sheath
- followed by peritoneum

Arcuate Line
AKA linea semicircularis: a horizontal line on post rectus sheath which demarcates a point where all of the aponeuroses (EO, IO, TA) pass anterior to rectus abdominus ms.

Abdominal Muscles Actions (Together)
- All abdominal muscle together-increase intra-abdominal pressure; resist downward pressure of the diaphragm during straining (bowel movement) & coughing
- Important during respiration (especially forced expiration), defecation, micturition (urinating), parturition (giving birth) & vomiting
- Recti aided by obliqui-flex the lumbar vertebral column if pelvis fixed; if thorax is fixed, they flex lumbar vertebral column & draw pelvis up
- Right E.O. & Right I.O. create Right sidebending
- Left I.O. & Right E.O create trunk flexion with rotation to the left
–You rotate toward your IO side
Azygos System
- drains venous flow from the thoracic wall (intercostal veins)
- intercostal veins on right lead to azygos vein on R
- intercostal veins on the left lead to accessory hemiazygos (superiorly) & hemiazygos veins (inferiorly)
- accessory hemiazygos & hemiazygos crosses over spinal column to dump into the azygos vein (~TV7-8)
- Azygos vein dumps into superior vena cava

VAN Complex
- intercostal vein, artery, nerve travel between the innermost and internal intercostal ms.
- run inferior to its corresponding rib
Relationship:
-intercostal vein most superior
- intercostal artery in the middle
- intercostal nerve inferior

Inguinal Canal
- oblique passage, 3-5 cm through abdominal wall
- Transmits in males-spermatic cord; females-round ligament of the uterus
- also contains ilioinguinal n. in female and male
- (L1 ventral ramus)
- Ant Wall of canal=aponeurosis of E.O. & ms. of I.O
- Post Wall of canal=aponeurosis of T.A. & transversalis fascia
**Runs parallel with inguinal ligament: 2 layers that make wall in front-aponeurosis of EO and IO
Conjoint tendon: IO and TA aponeuroses merge into joint tendon
*Floor-inguinal ligament & lacunar ligament

Deep Inguinal Ring
- slitlike opening in transversalis fascia found just above midinguinal point
- spermatic cord & round ligament of the uterus traverse the deep inguinal ring

Superficial Inguinal Ring
- triangular opening (variable size) in E.O. aponeurosis
- spermatic cord, round ligament of uterus & ilio-inguinal nerve (enters superifical, not deep) emerge through superficial inguinal ring to travel to the scrotum or labia

Indirect Inguinal Hernia
- abdominal contents (parietal peritoneum and small bowel exit the superficial ring) enter inguinal canal through deep ring and extend through the superficial ring
- more common than direct; more common in males
- usually contributed to a congenital defect
DANGERS: bowel contents which could cut off blood flow moving in and creating ischemic and necrotic tissueà can lead to sepsis bc fecal contents can end up in peritoneum

Direct Inguinal Hernia
- abdominal contents (parietal peritoneum and small bowel exit the superficial ring) enter inguinal canal directly through abdominal wall; contents protrude toward and may enter superficial ring, but rarely extend to scrotum
- Usually males > 40
DANGERS: bowel contents which could cut off blood flow moving in and creating ischemic and necrotic tissueà can lead to sepsis bc fecal contents can end up in peritoneum

ANS (autonomic nervous system)
- anatomically part of CNS (brain &spinal cord) & PNS (CNs &spinal nerves)
- function is generally involuntary & unconscious for control of homeostatic function of the body
- can be excitatory or inhibitory in nature
- controls activities of cardiac ms, lungs, smooth ms (insides of arteries, vasoconstriction), glands(saliva,tears,enzymes to break food down), viscera (involuntary structures)
ANS Sensory Responsibilities
- returns sensory information to brain: visceral (gut) sensation, baroreceptor/chemoreceptor information
- Cramping pain during menstruation or gas pain bc of intestinal virus
- someone with heart attack, decreased blood flow so crushing pain in left arm or jaw (radiating)
ANS Motor Responsibilities
-requires 2 neurons (preganglionic (ganglion=cell bodies outside CNS system) nerve & postganglionic nerve) to transmit a nerve impulse from the CNS to an end organ (versus a single neuron in the peripheral voluntary system to skeletal muscle)
- preganglionic cell bodies arise in the CNS
- postganglionic cell bodies arise in ganglia outside CNS
Preganglionic Nerve Fibers
-Preganglionic (myelinated-fatty fibers that help impulses travel faster, white) fiber synapses with postganglionic (unmyelinated-grey) fibers near the end organ
Postganglionic Nerve Fibers
- (unmyelinated-grey) fibers near the end organ
Sympathetic Nerves
Innervate: lung (bronchodilation-fight or flight), heart (contract faster), blood vessel walls, erector pilae(goosebumps), sweat glands, viscera, dilator pupillae(can see better)
-Usually a short preganglionic fiber & long postganglionic fiber
- mediates response to stress; mobilizes the body’s resources for action in emergency
- ↑HR, ↑bp, ↑contractility of heart, vasoconstriction, bronchodilation, sweating, ejaculation, dilates pupil
- Ejaculation is sympathetic, but erection is parasympathetic (vasodilation)
Parasympathetic
Innervate: glands in head (salivary for digestion), sphincter pupillae, blood vessels, heart (slow down), lungs (bronchoconstriction), digestive tract, bladder, bowel
- Parasympathetic system-responsible for maintenance of resting function, “rest & digest”
- erection is parasympathetic (vasodilation)
*Usually a long preganglionic fiber and a short postganglionic fiber
- function-homeostasis; ↓HR, ↓bp, ↓ contractility of heart, vasodilatation, bronchoconstriction, promotes digestion, empty bladder & bowel, constricts pupil
- acts to conserve resources
- Cranio-sacral outflow
- Cell bodies originate in Cranial nerves and sacral portion of cord
- CN 3, 7, 9, 10
- Sacral segments S2, 3, 4 keeps the penis off the floor, vasodilation too
- usually long pregangs & short postgangs (bc end up near target organ)
Sympathetic Motor System
- cell bodies originate in IMLG (intermediolateral grey) of spinal cord levels-T1 down through and including L1,2
- pathway-IMLG (intermediolateralgrey) >ventral root>spinal nerve>ventral rami>white rami communicante >sympathetic chain
3 choices
- synapse at that level in sympathetic chain & leave via gray rami
- synapse in a nearby level in sympathetic chain & leave via gray rami
- pass through sympathetic chain (without synapsing) as splanchnic n. (picks up 2nd order ganglion) & synapse near the target organ to get to guts

Sympathetic Chain (Trunk)
- a series of paired ganglia (paravertebral) on both sides
- runs from C1-S4; paired ganglia unite to form ganglion impart at sacral level
- lies lateral to vertebral column, on heads of ribs
- 22-23 pairs of sympathetic ganglia
- T1 ganglion blends with lower C ganglion=“stellate ganglion” (star)

Splanchnic Nerves
- Thoracic splanchnic nerves
- Destination: abdominopelvic cavity (to the celiac, aorticorenal superior and inferior mesenteric, intermesenteric, hypogastric plexi)
- still preganglionic sympathetic fibers
- Greater Splanchnic Ns.-T5-9 or 10
- Lesser Splanchnic Ns.-T10, T11
- Least Splanchnic Ns.-T12
- Lumbar splanchnic nerves-T5-T12 supplement the thoracic splanchnic ns Lumbar ganglions; still preganglionic
- arise from lumbar symph ganglia

CN III
-controls smooth ms that constricts pupil & accommodation of lens (gets thicker, thinner depending on distance you need to see)
CN VII
-secretion of tears & saliva
CN IX
-secretion of saliva
CN X
- cardiac, bronchi, esophagus, smooth muscle & glands of trachea, movements & glandular secretion of thoracic & proximal half of abdominal viscera (head, neck, thorax, halfway into abdomen)
- Note branches to the larynx: (may see in lab/often misid for CN XII)
- Superior laryngeal nerve with its branches: external laryngeal n. , internal laryngeal n.
- Inferior laryngeal nerve with its recurrent laryngeal branch
S2,S3, S4
-distal half of abdominal viscera via pelvic splanchnic (viscera) ns; also promotes digestion
Acetycholine (Ach)
- secreted by both systems preganglionic neurons (cholinergic), when get to
- secreted by most all parasymph postganglionic fibers
Noradrenaline
-secreted by most all symph postganglionic fibers(end organ), the neurotransmitter is different
Control of ANS
- descending signals from hypothalamus to cranial nerves (3,7,9,10) & spinal nuclei &
- solitary nucleus in brain stem (mostly medulla)
lHypothalamus & solitary nucleus receive afferent input from receptors in heart, major blood vessels, lungs, viscera etc.
llocal reflexes provide for regulation of most homeostatic function
- Afferent = sensory, receive this from ANS the ones circled in red
- your heart hurts bc you’ve had ischemia bc heart attack, gas pain, menstrual cramps
- how high is your BP and HR? all being influenced by hypothalamus and spinal nucleiàallow for quick response in terms of HR and BP

Carotid Sinus Reflex
*Local reflex- nothing going on upstairs!
- Carotid sinus-dilation of proximal part of internal carotid artery; (innervated by CN IX & X, provide sensory info about pressure); a baroreceptor that reacts to changes in bp
- increase in BP sensed by baroreceptors; afferent(sensory) fibers carry information to solitary nucleus through vagus n.
RESPONSE
- causes ↑ output of parasymph fibers which act on the heart to ↓HR
- causes ↓ in symph output to ↓ their action on the heart & sm ms. of blood vessels (vasodilation)
Autonomic Dysreflexia
- loss of supraspinal control (hypothalamus & solitary nucleus) of Symph nervous system and sacral segments (parasym) of the cord found in patients with cervical and high thoracic spinal cord lesions (usually above T5-T6)
- an acute, critical, life-threatening problem; can lead to seizures, stroke or even death
- AD is an uninhibited mass autonomic reflex response to a noxious stimulus (ingrown toe nail below the level of the lesion)
- Noxious afferent stimulus from below the level of the injury initiates a reflex action of the ANS (symph) of vasoconstriction of arterioles and arteries from the thoracolumbar sympathetic nerves
- Brain detects HTN via baroreceptors in neck (CN IX & X)
- The body’s normal compensatory mechanism (decrease of symph outflow which causes passive vasodilatation) cannot pass from higher centers through the level of the lesion; however the message to slow the heart can travel thru the vagus nerve and causes bradycardia (bc vagus nerve is outside of the spinal cord)
- However……the normal symph response to continued bradycardia results in an increase in blood pressure (>200/100 & as high as 300/180)
- Creates a vicious cycle
Signs and Symptoms of AD
Signs & Symptoms
- Pounding headache (b/c of ↑ bp)
- Paroxysmal HTN (> 200/100)
- Flushing above the level of the lesion (vasodilation)
- Pallor below the level of the lesion (vasoconstriction)
- Goose bumps-below the level of the lesion (symph)
- Cold, clammy skin below level of lesion (symph)
- Sweating above the level of the lesion – trying to dissipate some of energy above level of lesion
- Slow Pulse (< 60 bpm) (parasymp)
- Nasal Congestion (parasymp)
Causes of AD
Bladder related-most common
- UTI
- Urinary Retention-somebody with spinal cord injury, don’t realize it
- Blocked Catheter-has UTI, mucous pluck or blood clot, if urine cant get past blockage in catheter, urine backs up into bladder which could cause infection
- Overfilled Collection Bag
- Non-Compliance w/ intermittent catheterization if not could lead to urinary retention
- Bowel related
- Constipation
- Hemorrhoids
- Anal Fissure
- Infection (appendicitis)
- Tight Clothing
Skin Disorder
- Skin lesion or pressure sore
- Ingrown toenail
- Burn
Sexual Activity
- Over stimulation
- Menstrual cramps
- Labor & Delivery
Treatment of AD
Alleviate Noxious Stimuli if possible
- Check for kinks in catheter
- Drain Urine bag
- Straight catheterization
- Disimpact Stool digitally if stool softener doesn’t work
- Someones wheelchair wheel could be sitting in catheter
- Sit Patient up to create orthostatic hypotension on purpose
- Frequent bp checks-if color doesn’t look right
Treatment of High Risk AD Patients
- Individuals w/ recurrent episodes should have atropine(vasodilator) at bedside
- No longer than 3 days between BM(bowel movement)
Immediate/Emergent Care
- Nitroglycerine or Nitropaste: vasodilator
- Procardia: calcium channel blocker; vasodilates
- Hydralazine: quick vasodilator
- Clonidine: quick sympa output
- Chronic (recurrent episode prevention)
- Minipress or Clonidine on daily basis: alpha adrenerigic blocker; vasodilates
ANS Tests For Dysfunction
Blood Pressure (orthostatic hypotension test)
+ test if SBP dropped > 20 mm Hg or DBP dropped > 10 mm Hg
Normal variation approximately 10 mm Hg acceptable for SBP
Heart Rate (from supine to upright)
-Normal response is tachycardia in first 15 secs followed by bradycardia for the next 15 secs (if ratio < 1.04 = abnormal response)
Heart Rate Variation (during deep breathing)
- Normal response to deep breathing is variation in HR (HR slows during expiration)
- Healthy individuals have bigger variations in HR as a reaction to deep breathing vs. patients w/ impairment of parsymph NS
- Specific tests w/ ECG measure R-R interval & establish a ratio
Normal Responde to Exercise
- Gradual & linear increase in HR (proportional to exercise intensity)
- Gradual & linear increase in SBP (proportional to exercise intensity)
- Slight increase, decrease, or no change in DBP
- Increase in SV (2° increase in venous return)
- Increase in Cardiac Output
- Increase in O2 consumption
Abnormal Cardiovascular Responses during Exercise (MS pts)
Hallmark study by Senaratne et al. (1984) with significantly impaired group; showed SBP & HR response to exercise were significantly attenuated in > 50% of subjects with MS
Subjects demonstrated < 10 bpm increase in HR and < 8mmHG increase in SBP
AD Treatment Recommendations
- To determine if your patients has cardiovascular autonomic dysfunction, assess their BP response to postural change
- Measure BP lying supine after 5 minutes, and then standing after 3 minutes
- If BP drops 20/10 mm Hg or greater-considered an abnormal response
- Use the Borg scale of Perceived Exertion in addition to BP & HR responses to exercise with patients who you suspect may have ANS dysfunction
- Unclear if disability level is correlated with autonomic dysfunction, hence assess CV responses in all individuals with regardless of functional status
Borg Scale
- Rating of Perceived Exertion (RPE)
- 6 (very,very light) –> 20 (very, very hard)
Posterior Abdominal Wall
Comprised of:
- Lumbar vetebrae, sacrum, Ilium
- Posterior aspect of diaphragm, psoas major, iliacus & quadratus lumborum muscles

Posterior Abdominal Wall Arteries

Quadratus Lumborum Muscle
ACTION: fixes 12th rib during inspiration
- with pelvis fixed, creates ipsilateral sidebending of vertebral column
- bilateral axn-may assist in lumbar extension
- Ipsilateral elevation of pelvis (hip hiker)
PROXIMAL: from the medial 1/2 of inferior border of rib 12 and tips of lumbar transverse processes
DISTAL: to iliolumbar ligament and internal lip of iliac crest
INNERATION: ventral rami T12, L1-4

Iliolumbar Ligament
- attaches from: LV4-5 transverse processes to iliac crest
- stabilizes spine

Psoas Major
ACTION: flexes the hip jt; sidebending of vertebral column if LE fixed; flexes the trunk if pelvis fixed
PROXIMAL: From transverse processes of all Lumbar Vertebrae; lateral aspect of bodies of TV12 & Lumbar Vertebrae and discs in between
DISTAL: To lesser trochanter of the femur
INNERVATION: L2-L4 ventral rami

Psoas Minor
ACTION: assists in hip flexion and hip stabilization
PROXIMAL: From Lateral aspect of TV12-LV1 and discs in between
DISTAL: To pectineal line and iliopectineal eminence
INNERVATION: L1 & L2 ventral ramus

Lumbar Ventral Rami
- Lumbar ventral rami descend laterally in the psoas major muscle
- L1,2,3 and most of L4 form the Lumbar Plexus
- part of L4 and all of L5 form the lumbosacral trunk which joins the sacral plexus
- L1 also receives a branch from T12 ventral rami (subcostal n.)

Lumbar Plexus
Muscular Branches include:
- (T12), L1,L2,L3,L4 supply the following:
- quadratus lumborum (T12-L4)
- psoas minor (L1, L2)
- psoas major (L2,3,4) &
- ilacus (L2,3)
-Sensory Branches include:
- Iliohypogastric N. (L1)
- arises from upper border of psoas major, crosses the quadratus lumborum
- travels between the transversus abdominus and Int Oblique ms.
- gives off lateral cutaneous branch-supplies posterolateral gluteal skin
- gives off anterior cutaneous branch-supplies suprapubic region

Iliacus
ACTION: acts with the psoas major to flex thigh at the hip; stabilizes hip joint; (reverse action is….)
PROXIMAL: From the iliac crest, iliac fossa, ala of sacrum and anterior SI ligaments
DISTAL: To the tendon of the psoas major, lesser trochanter, and femur just distal to it
INNERVATION: Femoral Nerve (L2, L3)

Ilioinguinal Nerve (L1)
- arises from lateral border of psoas major caudal to iliohypogastric n., crosses the quadratus lumborum ms.
- Often runs parallel to the border of iliac crest
- pierces the Int Oblique ms. & emerges with spermatic cord from superficial inguinal ring
- supplies the proximomedial skin of thigh

Genitofemoral Nerve (L1-L2)
- ascends obliquely forward through psoas major ms. emerging near its medial border
- divides variably above the inguinal ligament into genital & femoral branches
- genital branch-supplies cremaster & scrotal skin
- femoral branch-supplies skin to upper part of femoral triangle

Lateral Femoral Cut Nerve (L2-L3)
- emerges from lateral border of psoas major, crosses iliacus obliquely
- passes deep to the inguinal ligament and divides into ant & post branches
- anterior branch-supplies skin of anterior and lateral thigh to the knee
- posterior branch-supplies skin lateral surface from greater trochanter to mid-thigh

Obturator Nerve (L2, 3, 4)
Motor and Sensory responsibilities:

- descends in the psoas major, emerges on its medial border at the pelvic brim
- descends forward on pelvic wall
- near obturator foramen divides into ant & post branches; goes thru obturator foramen
- ant branch-innervates: hip joint, add longus, gracilis, usually add brevis, sometimes pectineus (when not innerv by femoral n.); skin medial thigh
- post branch innervates: obturator externus, adductor portion of add magnus
- Sensation: medial aspect thigh
Femoral Nerve (L2,L3,L4)
- descends through psoas major, emerges on its lateral border; gives off motor branches to iliacus (in the abdomen) and pectineus (from medial side of N. near inguinal ligament)
- passes deep to the inguinal ligament into thigh
- splits into ant and post divisions
- ant division- medial & intermediate cutaneous femoral nerves, motor branch to sartorius
- posterior division-saphenous nerve and motor supply to quadriceps femoris; sensory to knee joint

LS Trunk and Sacral Ventral Rami
- LS Trunk=part of L4 ventral ramus and all of L5 ventral ramus joined together
- LS trunk joins with sacral plexus
- L4,5 joins with sacral ventral rami S1,2,3 to form sciatic nerve
- S2,3,4 ventral rami joins to form pudendal n.

Structures to identify in post abd wall
- medial & lateral arcuate ligament
- median arcuate ligament
- R & L crura of the diaphragm
- Hiatus in the diaphragm-aortic, esophageal, vena caval
- iliolumbar ligament-LV4-5 transverse process to iliac crest

Arteries of Post abd wall

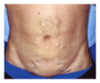
Caput Medusa
•engorged paraumbilical veins as alternate means of venous return to heart from LE
- appearance of distended and engorged paraumbilical veins which are seen radiating from the umbilicus across the abdomen to join systemic veins. The name caput medusae (Latin for “head of Medusa”) originates from the apparent similarity to Medusa’s hair once Minerva had turned it into snakes.
- Blockage may be inferior vena cava or from portal hypertension
*could lead to severe ascites!!
Mechanism of Refered Pain
- Error in perception by the brain as to the source of the painful stimulus
- An inability of brain to interpret a summation of noxious stimuli from various sources
- Pain from neural inflammation
- Pain from tendinopathy?
- Pain from bursitis?
- Pain for skin lesion?
- Visceral pain?
Referred pain from L5 injury
- pain felt in L5 dermatome may be arising from:
- L4-5 facet joint
- L5 disc
- muscles innervated by L5
- visceral structures innervated by L5
- joint capsule supplied by L5
Referred Visceral Pain
-Heart (C8-T4) on Left: thought to originate when visceral sensory nerve endings in the myocardium are irritated and then ascends up the sympathetic trunk and enter the spinal cord through the dorsal roots of the upper four Thoracic nerves (T1-T4) and therefore the pain is felt in the sensory dermatomes supplied by these spinal nerves.
-inferior MI, it’s assumed that the afferents enter the spinal cord through T7, T8, T9 spinal roots thereby given referred pain the epigastric dermatomes.
Since both the heart and the thoracic esophagus have similar visceral afferents, we should not be surprised that MI pain and pain from esophagitis may give rise to similar pain syndromes.
- Lungs (T2-5)
- Esophagus (T4-5)
- Liver (T6-9) right
- Ovaries & fallopian tubes (T11-L1)
- Kidneys (T10-T11)
- Colon (T8-L2)
- Bladder(T11-L3)
- Rectum, ovaries, prostate (S2-5)

Pelvic Diaphragm
*Aka Pelvic floor
- Composed of 2 levator ani muscles and 2 (ischio) coccygeus muscles
- Supports abdominal viscera
- Separates the pelvic cavity from the perineum
- Penetrated by the rectum, urethra and vagina
- We need pelvic diaphragm to keep organs (coughing,sneezing, bowel movements) held in place, keep it strong and intact

Levator Ani
Comprised of 3 muscles:

- puborectalis
- pubococcygues
- iliococcygeus
ACTIONS:supports pelvic viscera, resists the thrusts of increased intra-abdominal pressure (coughing, lifting heavy objects)
INNERVATION: the perineal branches of the S3 and S4 ventral rami
*essentially form pelvic diaphragm
Ischiococcygeus
–forms pelvic diaphragm with levator ani muscles
ACTIONS-supports coccyx, pulls it anteriorly; assists levator ani muscles.
INNERVATION- branches of S4 and S5 ventral rami

Lumbosacral plexus
- Descending portion of L4 ventral ramus unites with L5 ventral ramus to form the lumbosacral trunk
- Lumbosacral trunk passes ant. to ala of sacrum and joins the ventral rami of S1,S2,S3,S4 to form sacral plexus

Sciatic nerve branch of lumbosacral plexus
- ventral rami L4-S3
- tibial and common peroneal portions- supplies post. thigh muscles, lower leg (shank) and foot

Pudendal Nerve of lumbosacral
- ventral rami S2-S4
- Exits grtr sciactic foramen; reenters through lssr sciatic foramen
- Branches: inferior anal n; perineal n., dorsal n of the penis/clitoris (nice to know)
- Supplies the external urethral sphincter, anal sphincter and partial supply of levator ani; sensation to external genitalia

Superior gluteal nerve of lumbosacral
- Ventral rami L4, L5, S1
- supplies gluteus medius and gluteus minimus mm (above piriformis)

Inferior Gluteal nerve of lumbosacral
- ventral rami L5,S1,S2- supplies gluteus maximus ms. (below piriformis)

Nerve to piriformis
- ventral rami S1, S2
- innervates piriformis

N. to Obturator internus & Superior Gemellus
-N. to Obturator internus & Superior Gemellus- L5, S1, S2

N. to quadratus femoris & Inferior Gemellus
-N. to quadratus femoris & Inferior Gemellus- L4,L5, S1

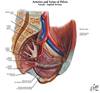
Arteries of the Pelvis
-Internal iliac a.- terminal branch of the common iliac a. (external iliac is other terminal branch)
Branches of internal iliac a. to identify:
–Iliolumbar a.- ascends laterally and supplies iliacus, psoas major, quadratus lumborum mm.
–Superior gluteal a.- largest branch; runs between the lumbosacral trunk (L4,5) and S1. Supplies piriformis, obt. internus, and gluteal mm.
–Lateral sacral a.-pass medially, ant. to sacral ventral rami giving off spinal branches through the sacral foramina
- -Obturator a.*-runs on lat wall of pelvis with obturator N. and V. through obturator foramen
- Inferior gluteal a.: largest branch of ant. trunk, supplies buttock and post thigh. Often runs between S1 & S2 (although Netter has it between S4 and S5 in this slide & S2, S3 in atlas)
- Internal pudendal a. (usually closer to the ischial spine than inferior gluteal a.)
Bony Pelvis
Comprised of:
- Ilium, ischium & pubis-become fused & meet at the acetabulum
- Sacrum
- Coccyx
- Comprised of 2 sacroiliac joints, a pubic symphysis and sacrococcygeal joint
- Acetabulum ( all 3 bones contribute)-socket for head of femur
- Acetabular notch
- Pubic tubercle
- Body of the Pubis
- Superior ramus of pubis
- Inferior ramus of the Pubis

Bony Pelvic landmarks
- ASIS
- AIIS
- PSIS
- PIIS
- Iliac Crest
- Iliac Fossa
- Auricular surface of the ilium articilates with sacrum
- Greater Sciatic Notch
- Ischial Spine
- Lesser Sciatic Notch
- Ischial Tuberosity
- Body of ischium
- Obturator Foramen

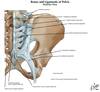
Pelvic Ligaments

Sacrum and Coccyx
- Ala of the Sacrum
- Sacral Canal (top)
- Body of SV1
- Auricular Surface (lateral view)
- Sacral Promontory
- Sacral Foramina
- Cornu of the Sacrum (post view only) and Coccyx
- Transverse Process of the Coccyx
- Tip of Coccyx

Posterior Sacrum and Coccyx
Lateral &
Median sacral crest & sacral & coccygeal cornu

Sacroiliac Joint
- Part synovial, part fibrous joint
- Irregular planar Joint by shape
- Articulation between auricular surface of the ilium and lateral aspect of sacral segments
- Sacroiliac Ligaments: Anterior, Posterior and Interosseus
- Accessory Ligaments- sacrospinous Lig., sacrotuberous Lig , iliolumbar Lig.

Ant SI lig, sacropinous & sacrotuberous ligaments

post SI ligaments, sacrospinous & sacrotuberous ligaments
Pubic Symphisis
- Cartilaginous Joint
- Articulation between the superior rami of the right and left pubic bones
- Hyaline cartilage on articular surfaces
- Fibrocartilage interpubic disc
- Jt. also strengthened by fibers of the rectus abd. m. and ext. oblique m. (both attach here)

Sacrococcygeal Joint
- Cartilaginous jt.
- Articulation between the apex of the sacrum and the base of the coccyx
- Sacrococcygeal ligaments (ventral, dorsal, lateral)
- Fibrocartilaginous intervertebral disc
- Can fracture or dislocate your coccyx=falling on your butt (ice skating)
- Painful when bear down to go to the bathroom, sitting (get them a donut so coccyx is elevated and they have some air between where they’re sitting and coccyx, bc painful when bone rubs against bone)

Pelvic Brim
Formed by:
- superior margin of the pubic symphysis,
- pubic crest: medial to pubic tubercle
Pectin pubis (pectineal line)
- arcuate line of the ilium
- ant. border of the ala of the sacrum
- promontory of the sacrum.
*this circle= brim

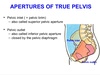
Superior pelvic aperture or pelvic inlet
- formed by the pelvic brim
- separates true (deep-bladder,uterus,rectum) and false pelvis
- Where things enter

Inferior Pelvic Aparture
- pelvic outlet (mickey mouse hole)where things exit
- bounded posteriorly by the sacrum and coccyx, anteriorly by the pubic symphysis, laterally by ischial tuberosities
- closed by the pelvic diaphragm
Pelvis Major
-Aka False pelvis-up near ilium
–Found in Abdominal cavity
–Lies between the iliac fossae superior to the pelvic brim
–Bounded anteriorly by the abdominal wall, laterally by the iliac fossae, and posteriorly by L5 and S1 vertebrae
–True pelvis is down where mickey mouse ears are

Pelvis Minor
AKA True pelvis-mickey mouse
- Lies inferior to the superior pelvic aperture and limited inferiorly by the inferior pelvic aperture
- Pelvic cavity containing pelvic viscera
- Bounded posteriorly by the sacrum and the coccyx, anteriorly by the pubic symphysis, body of pubis and pubic rami, and laterally by the ilium and ischium

Male pelvis vs Female Pelvis
uThicker, heavier structure
- More prominent bone markings
- Round obturator foramen
- Larger acetabulum
- Heart Shaped superior pelvic aperture
- Smaller inferior pelvic aperture-bc don’t need to deliver bb
- Narrow pelvis major
- Deep pelvis minor

Female Pelvis
- Thinner structure
- Less prominent bone markings
- Oval obturator foramen
- Small acetabulum
- Oval or round superior pelvic aperture
- Larger inferior pelvic aperture
- Shallow pelvis major
- Wide and shallow pelvis minor

Obturator Foramen
- Formed by the bodies and rami of the pubis and ischium
- Nearly closed by an obturator membrane
- Obturator N., A., and V. leave pelvis through the obturator foramen through the obturator canal

Greater Sciatic Foramen
Formed by:
- anteriorly & superiorly by the greater sciatic notch
- inf. by the sacrospinous ligament, and
- post. by the sacrotuberous ligament
- Acts as exit from inner pelvis for vessels and nerves (e.g. pudendal n.)
- Split into superior and inferior foramina by the piriformis muscle

Lesser Sciatic Foramen
Formed by:
- anteriorly by the lesser sciatic notch,
- Superiorly by the ischial spine and sacrospinous -ligament
- post. by the sacrotuberous lig.
Transmits:
- Obturator internus tendon,
- N. to obturator internus ms.
- Int. pudendal a. and v., and pudendal n.
Vertebral Column pattern
Cervical: lordosis
Thoracic: kyphosis
Lumbar: lordosis

Where does the spinal cord end?
- LV1-2
- Note cauda equine (horses’ tail) are ventral and dorsal roots only.
- Just bc have fracture in lumbar region, theres a disconnect where cord ends and where vertebral bodies are
- No motor, no sensory below that level will be working

Vertebrae
- body-function is support
- vertebral arch-function is protective
- vertebral foramen-houses spinal cord
- intervertebral foramina-houses spinal nerves & vessels-nerve exits and bifurcate into a dorsal or ventral ramus
- viewed from lateral
- When talking about someone with pinched nerve, are usually talking about something at the level of intervertebral foramina (maybe have tumor)
- Vertebral Arch composed of 2 lamina & 2 pedicles
- vertebral notches -superior (s) and inferior (i) vertebral notches which form the intervertebral foramen
- 7 projections from the arch
l2 transverse processes (t)
l1 spinous process (s)
(contd)

Superior and Inferior articulating processes and jt
*some of the 7 projections coming off of vertebral arch
- 2 superior articulating processes (sap)
- 2 inferior articulating processes
- together the articulating processes make a small synovial jt. bc has jt capsule (zygoapophyseal jt or facet jt)

Intervertebral Foramen
Formed by:
- Inf vertebral notch above &
•Sup vertebral notch below
- spinal nerve travels thru, but once gets thru the hole is ventral and dorsal ramus

Cervical Vertebare
•7 cervical vertebrae
- small broad body
- vertebral foramen-large & triangular
- spinous process-short & bifid
- sup aspect (body)-slightly concave
- inf aspect (body)-slightly convex
- sup articulating process facing post & upwards at 45’
- inf articulating facet facing forward and downward
- Transverse foramen-vertebral artery goes thru here
- transverse processes have foramen that transmit vertebral arteries, sympathetic nerves & venous plexus

Cervical Facet jt orientation
45 degs from horizontal

Anterior view of vertebrae
Uncus-prevents posterior translation of the vertebra
Intervertebral disc would be located at the blue arrow.
Superior aspect-concavity
Inferior aspect-convexity
*to stabilize the column more and with processes on side that lift up even further is so don’t get a dislocation easily

CV2-CV7 movements
- flexion/extension-greatest; 105’
- followed by rotation; 45’ (unilat)
- then sidebending; 35’(unilat)
CV1 (atlas) movement
- no body-occupied by dens of CV2
- articulates with occiput
- has no true spinous process
- has lateral masses (see x), skull sits on them
- movements-between occiput & atlas (O-A Jt.)
- flexion/extension-15’ (5’flex/10’ ext)
- sidebending-5’ (unilat)
- rotation-0’
- movement is primarily gliding or chin tuck-occiput is rolling on those masses like that (flexion and extension basically)

CV2 (axis) movements
- pivot upon which the atlas & head rotates
- distinguished by the dens; held in place by alar ligament & transverse ligament
- has a body
- transverse processes are small
- Movements between CV1 and CV2 (A-A jt)
–rotation-40-45’
•½ of cervical rotation occurs between CV1 and CV2
–flexion/extension- 5’ flex/10’ ext
–sidebending-0’
–rotation is greatest due to horizontally directed articular processes between CV1 and CV2

Ligamentous support of between C1 and C2
- Alar ligament=anterior
- Transverse ligament=posterior to alar lig
-rupture of transverse ligament in cervical spine of atlas is destabilizing injury that can occur in isolation or
with atlantoaxial subluxation or an atlas fracture;
- potential for CV1 to dislocate, what’ll happen in CV2 slides back or forward—compromises size of vertebral foramen which compromises pressure on cord
- transverse ligament is primary restraint to anterior translation of atlas in relation to the lower cervical spine;
- transverse lig can fail in midsubstance or avulsion of bone can occur;
- it has been estimated that a force of about 85 kg is required to rupture the transverse ligament;

Clinical presentation for ligamental problems
- Clinical Presentation:
- pt can give history of flexion injury and has neck pain, occasionally w/ associated head injury;
- diffuse motor loss may occur if the pyramidal tract is involved
May also occur in folks who have severe rheumatoid arthritis where there may be some ligamentous damage along with joint damage.
*halo vest-screw pins right into skull so cant move head at all (2 in front, 2 behind), keeps the spine stable for 6-8 weeks until the bone or ligament heels
- common to see after accident or if someone has joint destruction in this region, potentially RA (ligament erroded here)
- need to clean pins on a daily basis, so don’t get infection in bone-osteomyelitis-dura is right on the other side! If that travels, could end up with a meningitis!!! Or dural inflammation

