Medicine Specialties C - ONCOLOGICAL EMERGENCIES - Cord compression, S.V.C.O, Hypercalcaemia, Pericardial tamponade, Neutropenic sepsis, P.E COPY Flashcards
Oncological emergencies * Spinal cord compression * Superior vena cava obstruction * Hypercalcaemia * Pericardial tamponade * PE What are the presenting symptoms of spinal cord compression?
Signs and ysmptoms * BACK PAIN * Nocturnal pain usually worse and pain with straining * Limb weakness and difficulty walking * Sensory loss or bladder / bowel dysfunction
What is the classical type of back pain associated with SCC? * Radiating down the back of both legs * Intermittent * Radiating around the rib cage * Boring through the chest wall, from the back to the front
Back pain that radiates around the rib cage
What are the sensory changes that can occur due to cord compression? (touched more in neuro notes) What is the change in bladder and bowel symptoms?
Sensory changes can affect DCML tract and/or spinothalamic tract Resulting in loss of one or all of: * Proprioception * Light touch * Vibration /deep touch * Pain and temperature perception affected also
What is the cause of malignant cord compression?
The majority of malignant cord compression is due to vertebral body collapse/compression iminging the spinal cord Rarely however it can occur due to direct extension of a tumour into the vertebral column
What is the urgent management of spinal cord compression?
Urgent managemnt of cord compression is STEROIDS and SCAN Dexamethasone and MRI
What is the usual treatment options carried out after steroids have been administered?
Radiotherapy is the commonest and the mainstay of treatment Decompression surgery is considered but has some restrictions
When may surgery be tried in malignant cord compression?
Surgery should be considered in any patient with * Single vertebral involvemnt * No evidence of widespread mets * Radio resistant primary * Previous RT to sit * Unkown primary to get tissue
SUPEIOR VENA CAVA OBSTRUCTION What are the causes of SVCO as an oncological emergency?
Due to extrinsic compression from a tumour - most common or due to venous thrombosis in the SVC obstructing the vein - consider if current or past central venous access
What are the symptoms/signs of suprerior vena cava obstruction?
Reduced venous return from the head neck and upper limbs causes swelling of face neck, one or both arms (one arm suggest more distal) Headache Lethargy Shortness of breath Distended neck, chest wall and abdominal veins
What are the initial investigations carried out to diagnosis SVCO?
CXR - is there mass Venogram - is there a mass CT Chest
What are the treatment options if it is a clot causing the SVCO?
If there is a clot causing the SVCO Can thrombolyse eg alteplase or Anti-coagulate - LMWH
If the treatment of the SVCO is due to extrinsic compression due to a tumour, what is the treatment option?
Give O2 if needed Give dexamethasone to reduce inflammation Stenting provides the most rapid relief of symptoms but the underlying tumour must be treated Radiotherapy or chemotherapy (specific cancers are sensitive eg SCLC) depending on the sensitivy of the underlying cancer
MALIGNANCY ASSOCIATED HYPERCALCAEMIA What causes the malignancy assoicated hypercalcaemia in cancer patients? - affects up to a quarter of all cancer patients (what tumours are most common with local bone destruction)
Causes * PTHrP (parathyroid hormone related protein) - produced by the tumour - increases osteoclast activity causing increased calcium * Local bone destruction due to an invading tumour - especially lung, breast and myeloma * Tumour production of vit D analogues eg producing calcitriol
What are the symptoms of hypercalacemia?
* Stones - renal/biliary calculi * Bones - bone pain due to bone resorption * Groans - abdo pain, contipation, nausea * Thrones - polydipsia / polyuria * Psychiatric overtones - confusion, depression, anxiety, reduced GCS * Also cardiac arrhythmia
Which investigations should be carried out in a patient with suspected malignant hypercalcaemia?
Measure calcium levels Measure urea & electrolytes - looking for dehydration Measure phosphate - low in hyperparathyroidism
What is the treatment of malignant hypercalcaemia?
Initial treatment is rehydration (aggressive rehydration) IV biphosphonates (prevent bone resoprtion) Calcitonin can be given - more rapid but short term effect
How does calcitonin work? Where is it produced?
Calcitonin is a hormone that is produced in humans by the parafollicular cells (aka C-cells) of the thyroid gland. Calcitonin is involved in helping to regulate levels of calcium and phosphate in the blood, opposing PTH’s action. Reduces calcium reabsorption in kidney and absorption from gut. Decreases bone resorption.

If levels of caclitonin are raised in the blood, what cancer might this make you think of?
Medullary thyroid cancer is a form of thyroid carcinoma which originates from the parafollicular cells (C cells), which produce the hormone calcitonin.
CARDIAC TAMPONADE aka PERICARDIAL TAMPONADE How does a pericardial tamponade develop?
Pericardial effusion develops increasing intrapericardial pressure - this compresses the ventricle reducing cardiac output and collapsing the right atrium increasing venous back pressure Eventually the heart pumping stops
What are the causes of cardiac tamponade?
Malignancy Trauma Infection eg TB Post-MI Coonnective tissue disease Increased urea (Uraemia)
What are thee symptoms of pericardial tamponade?
Primarily shortness of breath Fatigue Palpitations Stmptoms of pericarditis (chest pain improved by sitting forward)
What are the signs of pericardial tamponade? (eg. Beck’s triad and signs on inspiration eg Kaussmaul sign, pulsus paradoxus)
* Beck’s triad * Increased JVP * Decreased blood pressure * Muffled heart sounds Kaussmaul sign - Increased JVP on inspiration Pulsus paradoxus - pulse fades on inspiration (venous return drops when intra-thoracic pressure raised)
What investigations are carried out to diagnose pericardial tamponade? What is seen?
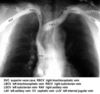
CXR - enlargement of cardiac silhouette - globular heart ECG - reduced complex size, also electrical alternans Echocardiogram - may be diagnostic - rim of pericardial fluid
Image shows the globular heart as seen on CXR Describe the ECG changes seen in pericardial tamponade?

Electrical alternans is an electrocardiographic phenomenon of alternation of QRS complex amplitude or axis between beats and a possible wandering base-line. It is seen in cardiac tamponade and severe pericardial effusion.


