MCQ Flashcards
What is true about the sesamoids?
the tibial sesamoid is larger
Blood supply - medial plantar artery and plantar arch
Sesamoid complex transmits 50% of the body weight
What are the surgical options for a burst fracture?
Anterior decompression with stabilization
Retropulsion with need for decompression
corpectomy with strut grafting
Posterior decompression with fusion
Instrumentation with distraction, get indirect decompression of the canal
Posterior fusion
Progressive kyphotic deformity
Compare two incision distal biceps
both can get PIN
same HO
better flexion with two incision
less LABCN with two incision
What are approapriate antibiotics for open wounds
- Gustilo 1
- cefazolin
- clinda if allergy
- Gustilo 2/3
- cefazolin
- gentamycin
- Farm wounds - penicillin or flagyl
- Freshwater (A hydrophilia)
- cipro or ceftazidime
- Salt water (vibrio)
- Doxycycline
- ceftaxidime or cipro
What is true about NF2?
- less common
- bilateral acoustic neuroma
- no scoliosis
What are the indications for treatment of a pediatric proxiaml humerus fracture?

- Neer-Horowitz classification
- type I is minimally displaced (< 5mm)
- type II is displaced less than 1/3 of the shaft width
- type III is displaced greater than 1/3 and less than 2/3 the shaft width
- type IV is displaced greater than 2/3 the shaft width
-
> 6 with the following displacement
- >50% displaced
- > 45 deg angulated
- open
- dysvascular
Sites of compression of the ulnar nerve at the cubital tunnel
Arcade of struthers
Medial intermuscular septum
Medial epicondyle
Osborne’s ligament
Between heads of FCU (fasica)
Aponeurosis of FDS
What structure causes retrograde ejaculation in the anterior approach to the lumbar spine?
Superior hypogastric plexus
What are the releases for a valgus knee?
osteophytes
Capsule
IT (extension)
popliteus (flexion)
LCL
What is your approach to factor replacement in a hemophiliac
- 2 hours pre op infuse with clotting factor calculated to attain 100% activity of normal
- Then maintained on continuous infusion of factor to maintain levels at >60% throughout the procedure
- Thereafter, levels are checked every 1 or 2 days.
- A 60% level is maintained by continuous infusion until the patient is discharged.
- Home infusion of bolus doses is used to maintain levels of 30% to 60% for at least 2 weeks postoperatively.
- If vigorous physical therapy is needed the patient is infused to a 30% level just before therapy
-
Complications
- hemarthorosis at 4-7 days if it occurs
- infection slightly higher
- risk of stiffness so no concern for instability
Complications of talar neck fractures
- Subtalar OA
- AVN
- malunion
- In that order, no matter the Hawkins classification, but the risk of each one will go up with subsequent grade
- Nonunion is a very low risk
What is the incidence of bilateral slip in a SCFE?
General population - 20%
Renal osteodystrophy - 80%
What injury pattern has the lowest rate of ligament injury and meniscal injury in a tibial plateau fracture?
Meniscal = lateral split (1)
ligament = depression (3)

Which dwarfism does not have an ustable c-spine?
achondroplasia
What is the most common cause of heel pain in the pediatric population?
Sever’s
Acceptable alignment of a humeral shaft fracture
< 20° anterior angulation
< 30° varus/valgus angulation
< 3 cm shortening
What is true about the genetics and etiology of achondroplasia?
-
FGFR3 point mutation G380R
- AD
-
80% are spontaneous
- associated with higher paternal age
- Leads to abnormal chondroid production in the proliferative zone
- short long bones
- endosteal ossification
- proximal > distal (?why)
- Spine
- narrow interpedicular distance (L1-5)
- narrow foramen magnum
- mortality, apnea, UMN
- screen all with MRI who have positive sleep study
- thoracolumbar kyphosis
- brace when young
- usually will resolve
- lumbosarcral hyperlordosis
- spinal stensosis
- narrow pedicles
- hyperplastic discs
- MSK
- genu varum
- rhizomelic shortening
- trident hand
What structures are released during plantar fascial release
- divide supericial fascia of the abductor hallucis
- fascia between abductor hallucis and plantar quadratus is released
- releases the nerve between the two
- a portion of the plantar fascia is incised
- medial heel spur is resected if present
Treatment of unstable PIP fracture-dislocations
-
Extension block pinning (transarticular)
- reducible joint with tenuous stability
- flex the joint slightly and pin the proximal phalax
-
CRPP
- reducible joint with tenous stability
- larger fragment ammenable to pinning
- not superior to extension pinning
-
Dynamic distraction and Ex-fix
- unstable pilon or > 50% (B type fracture)
- off-loads the joint and permits early ROM
-
Volar Plate arthroplasty
- augmented with button
- proected with k-wire
-
Hemihamate reconstruction arthroplasty (more for volar fractures)
- section of hamate if measured and transplated
- B type fractures can use hemiH or dynamic ex-fix; no studies to compare the two
- 2 week extension splint then ROMAT
- no long term studies
- easier to do in a more chronic situation where you can’t do a DynEx

What is the most common complication of a talar neck fracture?
subtalar OA
What are the indications for epiphyseodesis in congential scoliosis
- Age <5 years
- Site of anomaly in lumbar as opposed to thoracic spine
- A curve of five segments or less
- A progressive curve <40°
- Anomalies consisting of hemivertebrae instead of unsegmented bars
- Absence of excessive kyphosis
- Absence of neurological deficits, including syrinx, diastomatomyelia and tethered spinal cord
What are the MRI characteristics and treatment of an ABC?
- MRI - cystic, fluid-fluid levels showing blood and solid components
- curettage and grafting with cryotherapy
Approach to adolescent bunions
- best to wait until skeletal maturity to operate
- can not perform metatarsal osteotomies if physis is open (cuneiform osteotomy OK)
- surgery indicated in symptomatic patients with an IMA > 10° and HVA of > 20°
- severe deformity with a DMAA > 20 perform a double MT osteotomy
- technique
- soft tissue procedure alone not successful
- similar to adults if physis is closed (except in severe deformity)
What is the most sensitive test to detect OM?
MRI
What is the best treatment for a 20 yo female with JRA and trashed TN, CC and TC joints?
triple arthrodesis
What is the nonopertive treatment of spondylolisthesis?
Asx - non-op, full contact
Sx low grade - PT for pelvic tilt, core strength and hamstring stretches (know the risks and monitor)
Acute - TLSO, better than activity mod alone
What are the sensitivity/specificity/PPV/NPV
-
sensitivity = (true positive) / (true positive + false negative)
- proportion of individuals who truly have a designated disorder who are so identified by test
-
specificity = (true negative) / (true negative + false positive)
- proportion of individuals who are truly free of a designated disorder who are so identified by test
-
PPV = (True positive) / (True + False positives)
- proportion of individuals with a positive test who have the disease
-
NPV = (true negative) / (true + false negatives)
- proportion of individuals with a negative test who are free of the disease
What is the typical presentation of a glomus tumor
- Small red-blue nodule on gross histology
- typically in the nailbed
- can occur in other places
- riding or discoloration of the nailbed
- 20-40 yo
- F>M in subungual region only
- Triad
- paroxysmal pain
- cold intolerance
- localized tenderness
- XR
- may not be helpful
- scalloped osteolystic defect with sclerotic border
- MRI
- diagnostic
What are indications for surgery of a clavicle fracture?
unstable Group II fxs (Type IIA, Type IIB, Type V)
open fxs
displaced fracture with skin tenting
subclavian artery or vein injury
floating shoulder (clavicle and scapula neck fx)
symptomatic nonunion
posteriorly displaced Group III fxs
displaced Group I (middle third) with >2cm shortening

What is the effect of overstuffing a radial head arthroplasty
- increased load
- limit mobility
Anatomy of the blood supply to the hand
-
Superficial arch
- deep to palmar fascia
- distal to the to the deep arch
- at the level of a line drawn across the palm parallel to the distal edge of the fully abducted thumb
- predominant supply is ulnar artery
- 1st branch
- is the deep branch that provides the minor supply to the deep palmar arch
- 2nd branch
- is the ulnar digital artery of the little finger
- 3rd, 4th, 5th, and 6th branches
- are the common palmar digital arteries
- 1st branch
- Location compared to nerves
- in the palm, the digital arteries are volar to the digital nerves
- in the digits, the digital arteries are dorsal to the digital nerves
- in the digits, the neurovascular bundle is volar to Cleland’s ligament (ceiling, grayson = ground)
-
Deep Arach
- deep to the flexor tendons (FDS, FDP)
- proximal to the superficial arch
- at the level of the base of the metacarpals
- predominant supply is the deep branch of the radial artery
- princeps pollicis
- runs between 1st dorsal interosseus and adductor pollicis
- branch to the radial side of the index finger
- the proper digital artery to the radial side of the IF arises directly from the deep arch
- branches to the 3 common digital arteries in the 2nd, 3rd, and 4th web spaces
- princeps pollicis
- The deep arch is complete (branches to all digits) in 97% of individuals

What are the 5 mechanisms of wear in TJA
-
Adhesive wear
- most important in osteolytic process
- microscopically PE sticks to prosthesis and debris gets pulled off
-
abrasive wear
- cheese grater effect of prosthesis scraping off particles
-
third body wear
- particles in joint space cause abrasion and wear
-
volumetric wear
- main determinant of number of particles created
- directly related to square of the radius of the head
- volumetric wear more or less creates a cylinder
- V=3.14rsquaredw
- V is volumetric wear, r is the radius of head, w is linear head wear
- head size is most important factor in predicting particles generated
-
Linear wear
- is measured by the distance the prosthesis has penetrated into the liner
What is the treatment for the different stages of PTTI?
Grade 1 - debridment and tendon augmentation
Grade 2 - FDL transfer, medial calcaneal osteotomy, TAL, +/-cotton, +/-evans
Grade 3 - Double or Triple Arthrodesis (ST + TN +/- CC)
Grade 4 - Triple with deltoid recon if ankle is flexible
TTC if ankle valgus is fixed
Most common presentation of discitis in peds
> 9 back pain
3-9 abdo pain**
< 3 limp, posivite log roll
What is ture about NOF?
cortical
metaphyseal/diaphyseal
1-3cm
bubbly - not loculated
Eccentric
What is Morquio syndrome?
Mucopolysacharidosis
accumulation of keratn sulfate
presents at 18-24 months, proportionate dwarfism
normal intellegence, waddling gait, genu valgum, thoracic kyphosis, corneal clouding
XR - thick skull, wide ribs, vertebral beaking, coxa vera, unossified femoral head
*** Flex - ex views for C1-C2 instability

Complications associated with CTR
- inadequate release (most common)
- motor branch disection
- hypertrophic scar
-
pillar pain - pain over trapeizium and hamate prominence
- can result from division of the palmar cuteanous branch
- some sources quote this as more common
- adhesions
- laceration superificial palmar arch
- hematoma
- recurrence
What is the treatment for chronic achilles tear?
Type 1: gap < 2cm = end-to-end repair
Type 2: gap 2 to 5 cm = V-Y lengthening +/- tendon transfer
Type 3: gap >5cm = (FHL) tendon transfer alone +/- V-Y advancement
What are the common causes of wear in a metal on poly hip?
Mode 1 - bearing surface (adhesive, abrasive; MOST COMMON)
Mode 2 - bear on non-bearing; neck on poly
Mode 3 - 3rd body wear (poly, debris)
Mode 4 - non-bearing with non-bearing; backside wear (trunionosis)
What are the primary and secondary lesions associated with swan neck deformity
-
Primary
- trauma
- generalized ligament laxity
- rheumatoid arthritis
-
Secondary
-
mallet injury
- leads to transfer of DIP extension force into PIP extension forcee
-
mallet injury
- FDS rupture
- leads to unopposed PIP extension with an intact FDP
- intrinsic contracture
- tethering of the lateral (collateral) bands by the transverse retinacular ligament as a result of PIP hyperextension.
- if the lateral (collateral) bands are tethered, excursion is restricted and the extension force is not transmitted to the terminal tendon, and is instead transmitted to the PIP joint
- MCP joint volar subluxation
- caused by rhuematoid arthritis

Brachial plexus palsy: preganglionic vs postganglionic
-
preganglionic
- avulsion proximal to dorsal root ganglion
- involves CNS which does not regenerate – little potential recovery of motor function (poor prognosis)
- lesions suggesting preganglionic injury:
- Horner’s syndrome
- disruption of sympathetic chain
- winged scapula medially
- loss of serratus anterior (long thoracic nerve),rhomboids (dorsal scapular nerve)
- presents with motor deficits (flail arm)
- sensory deficits
- absence of a Tinel sign or tenderness to percussion in the neck
- normal histamine test (C8-T1 sympathetic ganglion)
- intact triple response (redness, wheal, flare)
- elevated hemidiaphragm (phrenic nerve
- rhomboid paralysis (dorsal scapular nerve)
- supraspinatus/infraspinatus (suprascapular nerve)
- latissimus dorsi (thoracodorsal)
-
evaluation
- EMG may show loss of innervation to cervical paraspinals
- Horner’s syndrome
-
postganglionic
- involve PNS, capable of regeneration (better prognosis)
- presentation
- presents with motor deficit (flail arm)
- sensory deficits
- evaluation
- EMG shows maintained innervation to cervical paraspinals
- abnormal histamine test
- only redness and wheal, but NO flare
What is true about the use of BMP-2 in open tibia fractures?
BEST
decreased need secondary intervention or subsequant bone grafting
increased healing rate
decreased infection in grade III only
Why do you not get lunate AVN with volar dislocation?
radioscaphoid ligament - ligament of testut is intact in all 4 stages of dislocation
What is true about anterior subcutaneous transposition and simple decompression for the ulnar nerve?
same functional outcome with higher infection rates with transposition (conchrane review from 2012)
Intrinsic tendon thumb insertions

What is the most common reason for sudden death in an RA patient?
basilar invagination
what is the treatment for schermans kyphosis
< 60 - observe
60-80 and risser < 3 - milwakee brace
>75 in skeletally mature - PSF
What additional tests and consults are required for Congenital scoliosis
- Cardiac
- cardiology consult
- echocardiogram
- Renal: common to have kidney issues
- renal ultrasound (at minimum)
- Neurologic
- spine MRI
- syrinx
- tethering
- neurosurg referral
- spine MRI
What are the surgical priorities of tendon transfers?
- elbow flexion (musculocutaneous n.)
- shoulder stabilization (suprascapular n.)
- brachiothoracic pinch (pectoral n.)
- sensation C6-7 (lateral cord)
- wrist extension and finger flexion (lateral and posterior cords)
What is the most common level of hip dislocation in myelomeningocele?
L3
What is an important consideration for myelomeningocele?
Latex allergy
What is the true regarding the treatment of OCD of the knee
- Stable lesions in a skeletally immature patient should not be treated surgically
- Unstable lesions should be treated
- reduce pain
- reduce OA - this is only theoretical
- Should be give PT
- Nothing to show that OATS or ACI are any better than microfracture
- microfracture should be first line of treatment
-
Outcomes of microfracture
- Age
- Duration of symptoms
- Lesion size
- Body mass index
- Preoperative activity level >4 (Tegner)
- Previous surgery (microfracture)
- Repair cartilage volume >66%
- MRI results of defect fill
What is your management for an anterior SC dislocation?
- > 3 weeks = leave it
-
< 3 weeks
- closed reduction under anesthesia
- figure 8 brace if acceptable
- leave it if unable to reduce
-
chronic and painful
- medial clavicle resection
What is the most important determining factor in AVN associated with pedicatric femoral neck fracture?
Age 3-8 (after 8 have the ligamentum teres; after 14 have metaphyseal flow)
-
Dalbet classification
-
Type I
- Transphyseal (IA, without dislocation of epiphysis from acetabulum; IB, with dislocation of epiphysis)
- 90-100% AVN
-
Type II
- Transcervical 40-50%
- 50% AVN
- 15% nonunion
-
Type III
- Cervicotrochanteric (or basicervical) 30-35%
- 25% AVN
- 15-20% nonunion
-
Type IV
- Intertrochanteric
- 10% ANV
- 5% Nonunion
-
Type I
What are the common principles for tendon transfers?
- donor must be expendable and of similar excursion and power
- one tendon transfer performs one function
- synergistic transfers rehabilitate more easily
- it is optimal to have a straight line of pull
- one grade of motor strength is lost following transfer
- only cross one joint
- Other concepts
- appropriate excursion
- 3 cm excursion - wrist flexors, wrist extensors
5 cm excursion - EDC, FPL, EPL
7 cm excursion - FDS, FDP
- 3 cm excursion - wrist flexors, wrist extensors
- appropriate tensioning
- appropriate excursion
What is true about the pathology of RA
- RF is an IgM antibody associated with RA a number of other autoimmune disorders
- attackes IgG
- monoclonal cells are the primary mediator of tissue destruction
- present in 1-2% of the general population
- prognostic value more than diagnostic value
-
Diagnositc criteria
- morning stiffness and swelling
- subcutaneous nodules
- positive laboratory tests
- anti-CCP is the most sensitive
- radiographic findings
What are indications for total patellectomy
- failed ORIF
- infection
- tumor
- PF OA
- 47% of the strength of the quads is lost
- should reinforce with VMO over the defect (shown to have better outcomes)
What are indications to perform corrective valgus osteotomy for coxa vara?
-
Hilgenreiner’s physeal angle > 60
- <45 unlikely to progress
- >60 will likely progress
- Neck-shaft angle < 110
- trendelenberg
- pain
- evidence of progression with serial exams
Important considerations - may need to transfer aductor tubercle to increase tension, monitor for LLD

What is the pathoanatomy of a SLAC wrist?
- chronic SL ligament injury creates a DISI deformity
- scaphoid is flexed and lunate is extended as scapholunate ligament no longer restrains this articulation
- scapholunate angle > 70 degrees
- lunate extended > 10 degrees past neutral
- Resulting forces
- abnormal distribution of forces across midcarpal and radiocarpal joints
- malalignment of concentric joint surfaces
- initially affects the radioscaphoid joint and progresses to capitolunate joint

What is the incidence of neuraxial abnormalities with juvinille scoliosis?
- Children 3-10 yo
-
high incidence of neural axis abnormalities (18-25%)
-
syringomyelia
- cyst or tubular cavity within spinal cord (due to increase CSF from tumor, arnold chiari..etc, need to drain it and treat underlying cause)
- can be seen in a scoliotic curve without rotation
- can manifest as an asymmetric umbilicus reflex
-
Arnold-Chiari syndrome
- cerebellar tonsil are elongated and protruding through the opening of the base of the skull and blocking CSF flow)
- tethered cord
- dysraphism
- spinal cord tumor
-
syringomyelia
What is the enneking tumour grading system?

Principles of medical ethics
- Respect for autonomy - the patient has the right to refuse or choose their treatment
- Beneficence - a practitioner should act in the best interest of the patient
- Non-maleficence - “first, do no harm”
- Justice - concerns the distribution of scarce health resources, and the decision of who gets what treatment (fairness and equality)
- Respect for persons - the patient (and the person treating the patient) have the right to be treated with dignity.
- Truthfulness and honesty - the concept of informed consent has increased in importance since the historical events of the Doctors’ Trial of the Nuremberg trials and Tuskegee syphilis experiment.
What are the features of Marfan?
Fibrillin Gene
Ortho - arachnodactyly, scoliosis, protrusio, laxity, dislocations, pes planovalgus
Non-ortho - aortic root dilations, aortic disection, mitral valve prolapse, pectus excavatum, pneumothorax, dural exctasia, meningocele
What are the sites of compression of the ulnar nerve in the cubital tunnel?
*Arcade of struthers
*Aponeurosis of FCU
*MCL and osborne’s ligament
medial head of triceps
intermuscular septum
medial epicondyle
anconeus epitrochleris
What is the watson classification for SLAC wrist?
-
Stage I SLAC wrist - scaphoid and syloid
- PA radiograph shows radial styloid beaking, sclerosis and joint space narrowing between scaphoid and radial styloid
-
Stage II SLAC wrist - scaphoid and entire DR
- PA radiograph shows sclerosis and joint space narrowing between scaphoid and the entire scaphoid fossa of distal radius
-
Stage III SLAC wrist - capitate and lunate
- PA radiograph shows sclerosis and joint space narrowing between the lunate and capitate, and the capitate will eventually migrate proximally into the space created by the scapholunate dissociation

What is the best test to examine osteoid osteoma?
CT - better than MRI to look for the nidus
What are the risk factors of hip AVN?

Diagnosis? Blocks to reduction? Treatment?

- Dorsal IP dislocation
-
late deformity
- swan neck - due to volar plate injury
- flexion deformity - resolves with PT
-
Blocks to reduction
- volar plate
- If open injury - FDP dislocation
-
Treatment
- buddy tape for 3-6 weeks if reducible
-
open to get reduction
- dorsal approach between central slip and lateral bands
Diagnosis? Imaging? Treatment?

Pediatric Odontoid fracture
-
Mechanism of injury
- high velocity flexion
- anterior displacement through the synchondrosis
-
Acutely
- Usally seen on lateral
- Can get CT to assess
- Flex-ex views if appropriate
- MRI - static if chronic to assess cord
- Then can do dynamic MRI to assess stability of the fragment
-
Treatment
- Reduction with Halo or Minerva for 3 months
- Acute
- Confirm reduction with XR
- Confirm healing with fle-ex views
- Usually heals with NO issues
- Reduction with Halo or Minerva for 3 months
-
Posterior C1/2 fusion (chronic)
- If no decompression necessary
- Brooks/Gallie - if young
- C1/2 lateral mass screws if older
-
Posterior Occiput-C2 fusion (unstable os odontoidium)
- For chornic injuries that you need to decompress posteriorly
- Otherwise hard to get your bone graft in
Cross-link in pedicle screw construct improves what stiffness?
- lateral Bending
- then torsion
What is this pathology? What is the appropriate treatment?

-
Vaughan-Jackson syndrome (RA)
- describes the rupture of the hand digital extensor tendons which occur from the ulnar side of the wrist first then moves radially
-
pathoanatomy
- results when DRUJ instability results in dorsal prominence of the ulnar head which results in an attritional rupture of the extensor tendons
- EDM is the first extensor ruptured.
-
treatment
- EIP to EDC transfer and distal ulna resection
What are the prognostic factors associated with OCD?
- Age - younger age better prognosis
- Lesion size less than 4cm2 show better prognosis
- Activity level- High impact athletes have worse prognosis though still improved
- Increased body weight- worse prognosis
- Patello-femoral lesions worse
- Better fill of defect on MRI correlated to better clinical results
What is the diagnosis and treatment for nec fasc?
- pain out of proportion
- systemic
- bullae
- Fascial edema from infection occludes arterial flow
- promotes spread of infection
- dishwater pus
- Nectrotic skin follows
- Most commonly GAS
- diabetic, HIV and malignancy at higher risk (but 50% in healthy patients)
What is often associated with CVT?
myelomeningocele
tethered cord
arthrogryposis
What is the measurement of the Kaplan - Meier survivorship curve?
number failed divided by the number still being followed
Medical treatment of spasticity in CP
- Benzodiazepine
- works systemically to reduce spasms and anxeity
- used with caution due to effects of sedation
- Bacolfen
- works centrally to decrease GABA receptors
- works to inhibit Ca influx from pre-synapic vessels
- drug of choice for spinal cord pathology in adults
- Dantrolene
- works peripherally on the muscles to decrease the release of Ca from the sarcoplasmic reticulum
- Botox - not given centrally
- injected into the muscle
- works locally to block release of Ach from pre-synaptic vessels
- Tizanidine - new with less sedation than some of the older medications
What is true about the stability of SI screws
- 2 screws have higher load to failure
- anterior plate with 2 screws is not as stable as native pelvis
What are the risk factors of progression for a congential scoliosis?
Rib Phase 1 (>2 will progress)
RVAD/Mheta < 20 (90% will resolve spont)
Cobb < 25
Double major curves progress

What artery supplies the lateral arm flap
posterior radial collateral artery
What position should you fuse the ankle?
neutral dorsiflexion
5 valgus
10 ER
Charnley cemented THA in 40-45 yo, survival at 10 years?
89%
Boney landmarks for the anterior cervical spine
Hard palate-arch of the atlas
Lower border of the mandible-C2-3
Hyoid bone-C3
Thyroid cartilage-C4-5
Cricoid cartilage-C6
Carotid tubercle-C6
What is the mechanism of botox?
blocks ACTH from release at the pre-synapic vesicles
What are the charactersitics of proteus syndrome
- skin overgrowth and boney deformation
- genetic mosacism
- often get overgrowth (hemihypertrophy)
- megalospondylodysplasia
- at risk of developing tumors
What is the nonoperative indication for pec major tears?
Partial ruptures
Proximal tears ( in the muscle or musculotendonous junction)
Sedentary patient
What is the treatment algorythm for a bennet fracture?
<1mm = cast
> 1mm and large = screw
> 1mm and small = k-wire (wagner pinning)
(one=oblique ligament, one=counter tendons)

What is the most common complication of a monteggia fracture?
PIN
Usually will resolve will closed reduction
Chronic nerve palsy is very rare, pateients complain of weakened power grip due to inability to extend wrist (can treat initially with PT to maintain ROM and then with tendon transfers)
Presentation and treatment of ACL ganglion cyst
- Presents with pain with flexion, especially deep flexion
- after activity
- mechanical symptoms
- Able to make diagnosis from MRI
- Classification
- anterior to ACL
- between ACL and PCL
- posteior to PCL
- Treatment
- arthroscopic vs image guided aspiration
- both have good outcomes with limited reported recurrence

What are the characteristics of Pasteurella
- genus of Gram-negative, aerobic but facultatively anaerobic bacteria
- occur in domestic pet bites (dog and cat)
- it is not difficult to isolate
- treatment
- tetanus, I&D
- clavulin, cipro/flouroquinolone, septra
In a hypoplastic thumb, what is an indication for pollicization of the 1st digit with thumb amputation?

unstable CMC joint

What are the important considerations when treating an adult brachial plexus injury?
Patient Selection
Timing of surgery
Prioritization of restoration
What is the Neer-Holwitz classification for pediatric proximal humerus fracture?
type I : < 5mm
type II : type III : > 1/3 and type IV : > 2/3 the shaft width
What are the treatment options for SLAC wrist by stage?
- Stage 1 - radial syloidectomy and scaphoid stabilitzation
-
Stage 2 - proximal row carpectomry
- CI if there is severe capitate OA
-
Stage 3 - four corner fusion
- no evidence to show superior to proximal row carpectomy
-
Wrist Fusion
- option for pancarl OA
- good pain control and return of grip with loss of motion
What are the indications and contraindications for doing a TLIF?
-
Indications
- spondylolisthesis (low grade)
- degenerative scoliosis
- severe instability
- pseudarthrosis
- recurrent disk herniation
- painful degenerative disk disease
-
Contraindications
- epidural fibrosis
- active infection
- conjoined nerve roots
- restrict access to the disk space
- severe disk space collapse
- severe ankylosis
- osteoporosis
What is the classification of muchopolysaccaroidosis
-
Hurler
- most severe
- α-L-iduronidase
- Dermatan sulfate, heparan sulfate
-
Hunter
- Iduronate-2-sulfatase
- Dermatan sulfate, heparan sulfate
-
San Filipino
- most common
- Heparan sulfate, chondroitin sulfate
-
Morqouio
- Keratan sulfate, chondroitin sulfate
What is the best way to access cross sectional invovlement of tarsal coalition?
CT scan
What are the common complications associated with ankle arthroscopy?
-
Synovial cutaneous fistula
- avoid by immobilization to allow portal skin healing and closure
- Neurovascular injury from portal placement
- Anterolateral portal
- risks dorsal intermediate cutaneous branch of superficial peroneal nerve
- most common neurovascular injury
- Anteromedial portal
- risks saphenous nerve and vein
- Anterocentral portal
- risks dorsalis pedis artery
- Posterolateral portal
- risks sural nerve and small saphenous vein
- Posteromedial portal
- risks posterior tibial artery
Compare osteoporosis and osteomalaceia
-
Osteoporosis
- reduced bone mass
- Type 1 - postmenopausal
- trabecular
- distal radius, VB (and IT hip)
- reduced Vit D and intake
- Type 2 - elderly
- trabecular>cortical
- hip/pelvis (femoral neck)
- reduced Ca intake
- pain at fracture
- Labs
- Ca, ALP and urinary Ca are normal
- Tetracycline labelling - normal
- Osetopenia - 1-2.5 SD below 25 yo
- Osteoporosis - >2.5 SD below 25yo
-
Osteomalacia
- reduce bone mineralization
- generalized bone pain
- appedicular fractures, deformity and looser zones
- Labs
- will be altered based on etiology (rickets, hyperparathyroid, hypophosphatasia)
- abnormal tetracycline labelling
Use of aprotinin to reduce blood loss in hip and spine surgery
Trasylol, or aprotinin; Historic drug used to prevent blood loss by inhibiting fibrinolysis. Was taken off the market in 2008 due to complications including death
What are the important techniques when applying halo?
-
Movement Restriction
- More motion below C2
- Controversial - most motion at C2/3 and least at C7/T1
- Some say allows 70% of flexion
-
Contraindications
- absolute
- cranial fracture
- infection
- severe soft-tissue injury at the proposed pin sites
- relative
- severe chest trauma
- obesity, advanced age
- recent evidence demonstrates an unacceptably high mortality rate in patients aged 79 years and older (21%)
- barrel-shaped chest
- absolute
-
Indications for CT
- possible fracture
- child
-
Adults
- total of 4 pins
- 2 posterior pins
- 1 cm above the pinna
- 2 anterior pins
- lateral 1/3 of the eyebrow
- this is anterior/medial to temporalis fossa
- this is lateral to supraorbital nerve
- 2 posterior pins
- tighten to 4-8 inch-pounds of torque
- (not foot pounds..)
- have patient return on day 2 to tighten again
- total of 4 pins
-
Pediatrics
- more pins, less torque
- total of 6-8 pins
- lower torque (2-4 in-lbs or “finger-tight”)
*

What is the most common nerve injury in THA? What is the recovery?
- Sciatic (Peroneal division)
- most often damaged by retractors
- 70% of people will have subclinical findings
- Risk factors
- Women
- DDH
- Revsion surgery
- Do to the large size of the nerve and the proximal from the end organ recovery is rare
- Treatment is supportive
- Prevention is the best stragtegy
What is the harrington technique described for acetabular deficit
antiprotrusio cage with screws
liner secured PMMA
3 rods to reconstruct posterior column of the acetabulum

If you have a normal ESR/CRP do you need to get further imaging?
No
What is the vancouver classification and associated treatments
-
A; L (lesser), G (greater)
- Occurs in trochanteric region
- Commonly associated with osteolysis and often requires treatment that addresses the osteolysis
- Often will require ORIF with claw plate if adequate bone stalk
-
B1
- Fx around stem or just below it with a well fixed stem
- Often unreconized B2 - make sure you assess the XR adequatly
- ORIF using cerclage cables and locking plates
-
B2
- Fx around stem or just below it, loose stem, but good proximal bone stock
- Revision of the femoral component to a long porous-coated cementless stems (fluted, tapered)and fixation of the fracture fragment. Revision of the acetabular component if indicated.
- Bypass # - 1.5cm
- May need ETO to get the component out, fix with circlage wires
-
B3
- Fx around stem or just below with proximal bone that is poor quality or severely comminuted
- Femoral component revision with proximal femoral allograftn (young) or proximal femoral replacement (old and low demand)
- Consider the demand of your patient - femoral replacement only for low demand patients
-
C
- Fx occurs well below the prosthesis
- ORIF and with plate
What is the advantage of lateral column lengthening over medial calcaneal slide?
better forefoot adduction
Compare observational and experimental designs for research studies
-
observational
- researchers observe patient groups without allocation of intervention
- may be either prospective or retrospective
- may be descriptive or analytic
-
descriptive
- useful for obtaining background information for more advance studies
- examples
- case reports
- case series
- cross-sectional studies
-
analytic
- explores the association between a given outcome and a potentially related variable
- examples
- case-control
- cohort
- meta-analysis
-
descriptive
-
experimental
- researchers allocate treatment
- allows the evaluation of efficacies of therapeutic interventions
- examples
- double-blinded, prospective, randomized clinical trial is the gold standard for evidence based medicine
What is true about safe tourniqutte use?
- For a given leg circumfrance, a wider cuff means a lower pressure
- ischmeic injury to nerves can occur, thought that muscles are more sensitive than nerves
- > 2 hrs
- 350mmhg - lower
- 250 mmhg - upper
- EMG findings in 70% of patients 5 months later
- slower recovery
- muscles can recover from periodic ‘rest’ during surgery but nerves do not
- Consider the SBP to use the smallest measured pressure
- How to reduce tourniquette damage
- wider cuff
- cool extremity
- 2 cuffs, alternate use
- pad the extremity
- don’t use prep
Most important prognositc factor surrounding this fracture?

PIP subluxation inhibits the gliding arc of the joint and portends a poor clinical outcome (therefore, congruent joint reduction is the most important factor)
articular surface reconstruction is desirable, but not necessary for a good clinical outcome

What is the mangement of SCIWORA?
MRI to rule out hematoma/edema/cord transection or missed ligamentous injury
Immoblization (c-collar) 2-3 weeks
monitor
Extrinsic tendon insertions on the thumb
- EPL control IP flexion

what is true about the prognosis of SCIWORA?
latent presentation can occur
delayed is often more severe
worse at presentation=worse prognosis
MRI - can indicate full transection, hemorhage, edema or nothing (the less injury means better prognosis)
What is a pelligrini-steida lesion
chronic MCL deficiency leads to calcification next to medial femoral epicondyle

What is the stulberg classification?
LCP
I - spherical congruency
II - spherical congruency with <2mm loss and starting to have changes
III - aspherical congruency with > 2mm and changes
IV - aspherical congruency with flat head and abnormal neck; mild OA
V - aspherical incongruency; abormal head with severe OA
What are the treatment of LCP based on stages?
A - Observe, casting
B, B/C - containment in fragmentation phase
Later can do abduction/ext or chiari as salvage procedures
complications of patellar ORIF
- hardware irritation
- hardware migration is rare
- stiffness
- strength
- pain
- not associated with immobilization
- Nonunion
- deep infection
- association with OA is unclear
What are the indications for surgical fixation of a burst fracture?
Burst - anterior and middle column invovlement with retropulsion into the canal
Neurological deficits
Unstable pattern
Posterior injury
Progressive kyphosis
30 kyphosis
>50% height
>50% canal comprimise
****There is no association of retropulsion with neurological comprimise; the retropulesed fragment if not causing neuro deficiet can be left as the fragment will eventually resorb
What cells produce hyalouronic acid?
human synovial cells - special cells in the lining of the synovium
What are blocks to reductions for subtalar dislocations?
Medial - peroneals, EDB, TN capsule
Lateral - FHL, FDL, Tib post
What is the Hawethorne affect?
Patients change their outcome based on the treatment they receive
When can you stop seeing a patient?
When they have a new physician
What’s the most important factor for TKA ROM
pre-op ROM
Describe Odriscoll’s test for PLRI
forearm full supination; supination + extension
flexion + valgus force + axial load = rotatory supination torque on forearm
Characteristics of endcondroma

- A benign chondrogenic lesion caused by an abnormality of chondroblast function in the physis
- chondroblasts escape the physis and proliferate in metaphysis
- 2nd most common benign cartilage lesion (osteochondroma is most common)
-
Age & location
- age range is 10-60 years
- occurs in medullary cavity in diaphysis or metaphysis
-
hand is most common location (60%)
- presentation as pathological fractures common
- other locations include the femur (20%) and proximal humerus (10%)
-
solitary enchondroma
- 1% chance of malignant transformation (chondrosarcoma)
-
Ollier’s disease (multipe enchondromatosis)
- no genetic predisposition has been identified
- multiple enchondromas in long bone diaphysis
- 10-30% chance of malignant transformation into chondrosarcoma
- however associated with high rate of both skeletal and non-skeletal malignancies
- involved bones are dysplastic
-
Maffucci’s syndrome
- no genetic predisposition has been identified
- multiple enchondromas and soft-tissue angiomas
- 100% chance of malignant transformation into chondrosarcoma
- increased risk of visceral malignancies (astrocytoma, GI malignancy)
Stages of fracture healing (MCQ: What cells are present in the inflammatory healing)
-
Inflammation
- Hematoma forms and provides source of hemopoieitic cells capable of secreting growth factors.
-
Osteocytes undergo apoptosis, macrophages, neutrophils and platelets release several cytokines
- this includes PDGF, TNF-Alpha, TGF-Beta, IL-1,6, 10,12
- lack of TNF-Alpha (ie. HIV) results in delay of both enchondral/intramembranous ossification
- Fibroblasts and mesenchymal cells migrate to fracture site and granulation tissue forms around fracture ends
- during fracture healing granulation tissue tolerates the greatest strain before failure
- Osteoblasts and fibroblasts proliferate
- inhibition of COX-2 (ie NSAIDs) causes repression of runx-2/osterix, which are critical for differentiation of osteoblastic cells
-
Repair
-
Primary callus forms within two weeks
- the mechanical enviroment drives differentiation of either osteoblastic (stable enviroment
- <2% strain = osteoblasts = intramembranous
2-10% strain = chondrocytes = enchondral
- <2% strain = osteoblasts = intramembranous
- cartilage production provides provisional stabilization
- Type II collagen (cartilage) is produced early in fracture healing and then followed by type I collagen (bone) expression
- Amount of callus is inversely proportional to extent of immobilization
- the mechanical enviroment drives differentiation of either osteoblastic (stable enviroment
-
Primary callus forms within two weeks
-
Remodeling
- Begins in middle of repair phase and continues long after clinical union
- chondrocytes undergo terminal differentiation
- complex interplay of signaling pathways including, indian hedgehog (Ihh), parathyroid hormone related peptide (PTHrP), FGF and BMP
- type X collagen types is expressed by hypertrophic chondrocytes as the extraarticular matrix undergoes calcification
- proteases degrade the extracellular matrix
- cartilaginous calcification takes place at the junction between the maturing chondrocytes and newly forming bone
- subsequently, chondrocytes become apoptotic and VEGF production leads to new vessel invasion
- newly formed bone (woven bone) is remodeling via organized osteoblastic/osteoclastic activity
-
Shaped through
- Wolff’s law: bone remodels in response to mechanical stress
- piezoelectic charges : bone remodels is response to electric charges: compression side is electronegative and stimulates osteoblast formation, tension side is electropostive and simulates osteoclasts
What are indications for hemi-epiphyseodesis in congential scoliosis?
<5 yo
no kyphosis
<5 segments
hemivertebrae (NOT unsegmented bars)
absence of neurological deficiet
What is the herring classification?
LCP - lateral pillar
A - no involvement
B - > 50% lateral pillar height
B/C - lateral pillar at 50%
C - < 50% lateral pillar height
What occurs in a normally loaded joint
- NO EDGE LOADING
- Functional loads will not result in pain during normal ROM
- Small change in direction of functional loads will not result in sudden shift in the joint
What are the normal and acceptable criteria for a distal radius fracture?
- AP
- Radial height
- 13 mm
- <5 mm shortening
- Radial inclination
- 23 degrees
- change <5°
- Articular stepoff
- congruous
- <2 mm stepoff
- Radial height
- LAT
- Volar tIlt
- 11 degrees
- dorsal angulation <5° or within 20° of contralateral distal radius
- Volar tIlt
What views are required to assess hillsachs
IR view
stryker notch
How do you prevent heel pad migration in a symes amputation?
attach heel pad to anterior tibia
What is true about HIT?
- Immune repsonse to heparin 4-10 days following initiation
- less response to LMWH, but present
- type 1 is not immune mediated
- skin lesions, chills, fever, dyspnea, chest pain
- HIT as likley diagnosis
- timing (4-10 days following start)
- >50% drop in platelets
- presence of DVT with heparin
- start WU if >50% drop in platlets
- functional assay
- immunoassay
- U/S to rule out DVT
- CT PE
- treatment
- stop heparin/LMWH
- don’t use warfarin until platelets normal
- Dabigatron or direct platelet inhibiter a good options
- avoid platelet transfusion
what are the radiographic findings of a VISI?
scaphoid flexion
triquetrum extesion
volar flexion lunate
No LT widening
SL angle <30
break in gilula’s arc with superior migration of triquetrum

What would PRC be an option for?
Stage 2 SNAC
Stage 2 SLAC
Stage IIIb, IV Keinbochs
failed implant
severe trauma to lunate
Options for surgery in congenital scoliosis
-
in situ arthrodesis, anterior/posterior or posterior alone
- indications
- unlateral unsegmented bars with minimal deformity
- As risk for crackshaft and may not prevent progression in children
- indications
-
hemiepiphysiodesis
- indications
- intact growth plates on the concave side of the deformity
- Cannot use in a patient with unsegmented bars
- <5 yrs. with curve <40-50
- mixed results
- indications
-
osteotomy
- osteotomy of bar
- for more severe; rigid deformities
-
hemivertebrectomy
- hemivertebrae with progressive curve causing truncal imbalance and oblique takeoff
- often caused by a lumbosacral hemivertebrae
- <6 yo
- flexible curve > 40 degrees
- Difficulty procedure requiring both anterior and posterior exposure
- hemivertebrae with progressive curve causing truncal imbalance and oblique takeoff
-
spinal column shortening resection
- indications
- deformities that present late and have severe decompensation
- rigid, severe deformities
- pelvic obliquity, fixed
- indications
What are the portals for elbow arthroscopy?
-
Proximal anterolateral
- 2cm proximal, 1cm anterior to lateral epicondyle
- Radial n.
-
Distal anterolateral
- 1 cm anterior and 1-3cm distal to lateral epicondyle
- 1st portal for supine position
- See radial head, medial side of elbow, coronoid, trochlea, brachialis insertion, coronoid fossa
- Radial and lateral antebrachial cutaneous
-
Direct lateral (or midlateral)
- “soft spot” portal (in triangle formed by olecranon, radial head, epicondyle)
- Initial site for joint distension before scope is inserted, viewing posterior compartment (capitellum, radial head, radioulnar articulation)
- relatively safe, lateral antebrachial cutaneous nerve
-
Anteromedial
- 2 cm anterior and 2cm distal to medial epicondyle.
- Place under direct visualization.
- medial antebrachial cutaneous and median
-
Proximal medial (or superomedial)
- 2cm proximal to medial epicondyle, anterior to intermuscular septum
- viewing entire anterior compartment, radial head, capitellum, coronoid, trochlea
- ulnar and median
-
Straight posterior (transtriceps)
- 3cm proximal to olecranon, triceps midline (musculotend. junction)
- Elbow partially extended, good for removing impinging olecranon osteophytes and loose bodies from posteromedial compartment
- posterior antebrachial cutaneous and ulnar nerve
-
Posterolateral
- 2-3 cm proximal to olecranon and just lateral to triceps
- center of anconeus triangle
- Elbow 20-30deg flexion (to relax triceps)
- Best access to posterior compartment, radiocapitellar joint (debridement of OCD capitellum), olecranon fossa and posterior structures
- posterior antebrachial cutaneous and medial brachial cutaneous and ulnar

What are the conditions associated with this pathology?

thumb hypoplasia/radial clubhand
VACTERL
Holt-Oram
thrombocytopenia-absent radius (TAR)
Fanconi anemia
What are the transfers for an MC nerve palsy?
Regain elbow flexion
Stindler’s flexorplasty
latissiumus dorsi/pec major to biceps
What are the findings of hypophosphatasia?
- Low ALP
- High Ca
- Normal PTH
What are the contents of the carotid sheath?
the common carotid artery as well as the internal carotid artery
internal jugular vein
the vagus nerve (CN X)
the deep cervical lymph nodes
What is characteristic of scoliosis associated with neurofibromatosis?
- Idiopathic vs dystrophic
- idiopathic is more common
- overall, idiopathic will become dystrophic in 65%
- younger age=higher risk
- dystropic progress faster
- usually thoracic kyphoscoliosis (type II curve)
- type I curve < 50 deg kyphosis
- short, segmented, sharp curve with distorted ribs
- XR
- short, segemented
- sharp curve
- vertebral scalloping
- rib pencilling (suseptible to dislocation)
- enlarged foramina
- MRI
- dural ectasia
- dumbell lesion
- paraspinal mass
- vertebral scalloping
- TX = bracing ineffective
- early in young children (cobb <20)
- >20 = fusion

What is the strongest construct for a patella fracture
figure of 8 wires with cannulated screws
interfrag screws for comminution
What are the boundaries of hunter’s canal and what are located with-in?
vastus medius, adductor magnus, sartorius
femoral artery, femoral vien, saphenous nerve, nerve to vastus medialis
Etiology of scapulothoracic crepitus
- 43% - osteochondroma
- 30% - idiopathic
- 15% - rib resection
- 12% - soft tissue
What is the definition of incidence?
of people patients who developed the disease in a set period of time
What is the most important alignment to maintain in subtalar fusion?
5 deg valgus
Regarding human bite, how do you treat Eikenella Corodins?
Penecillin
What are acceptable treatments of this lesion?

- >25% deficit
- Infraspinatous sewn into defect (remplissage)
- >40%
- Allograft for young patient
- hemi for older patient

Characteristics of transient osteoporosis
- young, middle age men
- or women in 3rd trimenster
- Presents with rapid development of pain and reduced ROM
- Differential
- regional migratory OP
- AVN
- neoplasia
- usually in the hip; ONLY lower extremity
- thought to be similar to an AVN process that stops
- blood tests will be normal but should be done to rule out other causes
- XR
- will show demineralization over 3-6 weeks
- 2 years to return, but never collapses
- MRI
- will rule out AVN

Compare medial and lateral OCD lesions of the talus
-
medial talar dome
- usually no history of trauma
- more common
- more posterior
- larger and deeper than lateral lesions
-
lateral talar dome
- usually have a traumatic history
- more superficial and smaller
- lower incidence of spontaneous healing
- more anterior
What nerve guides the dissection into the popliteal fossa?
medial sural cutaneous nerve

What is true about THA versus cannulated screws?
No increase mortalilty at 3 years
Better function outcome with THA
Increased risk of complications with THA
Reduced risk of re-operation with THA
What are the sources of compression of the PIN?
Fibrous Bands
Recurrent radial artery - lesh of henry
Tendonous ECRB
Arcade of Frosch (proximal supinator) (MOST)
Distal supinator (least)
What is the pathology of SIADH and what is the treatment
- dilution of plasma from water retention and therefore low NA
- hyponatremia = headache, N/V, confusion
- but do not become volume deplete
- treated with water restriction
-
Must be differentiated from cerebral salt wasting
- loose Na in the urine due to renal insufficiency and become hyponatriemic and hypovolemic
- treat with aggressive fluid resucitaiton
Indications for surgical treament of MCL
commonly ruptured off the femoral insertion
- Failed Non-op
- Excessive > 10o laxity in Full extension (Associated posteromedial injury)
- Associated Cruciate or Meniscal Injuries
- Entrapment of MCL ligament inside compartment
- Stener lesion - can lay over top of pes tendon if comes off the tibia = much less likely to heal
Approach to radial head arthroplasty
-
Approach for Surgery
- kocher will allow you to see LUCL
- EDC split will all you to see more anterior
- Arm held in pronation to protect the PIN, 2.6cm distal to the RC joint
-
indications
- for comminuted fracture with 3 or more fragments
- technique include two type of metal prosthesis, both are in use
- monopolar prosthesis are better at resisting residual instability
- pressfit that acts as a stiff spacer
- risk of loosening
- bipolar prosthesis that is cemented into the neck of the radius
- risk of dislocation
- silicon replacements are no longer used
-
Sizing radial head
- Size the contralateral head pre-op
- Size to original radial head - thickness and cup
-
Trial reduction with visual inspection - most reliable
- Proximally should line up with less sigmoid notch
- Lateral UH joint are opposed
- gapping 0.9mm = 2mm overstuffing
- Flouro
- Medial and lateral UH joint lines (can’t see this until >6mm)
- Look for congruency of the medial UH joint
-
Repair the LCL using the docking technique
- this is one of the most important parts of the technique
-
complications
- overstuffing of joint that leads to capitellar wear problems and malalignment instability
Treatment

-
Nonoperative
- double ring splint
-
indications
- can prevent hyperextension of PIP
-
Volar plate advancement and PIP balancing with central slip tenotomy
-
indications
- progressive deformity
-
technique
- address volar plate laxity with volar plate advancement
- correct PIP joint muscles imbalances with either
- FDS tenodesis indicated with FDS rupture
- spiral oblique retinacular ligament reconstruction
- central slip tenotomy (Fowler)
-
indications
-
DIP Arthrodesis
- Dorsal approach
- Extensor tenodesis with capsulotomy

What is the litchman classification?

How do you prevent and treat recurrent laryngeal nerve injury?
- 2-3%, 9% with re-operation
- can get ENT for second procedure
- use the same side
- likley cause is impingement between ET tube cuff and retractors and continuous compression against the esohpagus
- Presents with post-op hoarsness or vocal cord paralysis
- don’t forget to include esphophageal rupture in your diagnosis
- if you see it, watch over time
- if not improved over 6 weeks than ENT consult to scope patient and inject teflon
What are risk factors for clavicle nonunion?
smoking
advancing age
female
comminution
> 100% displacement
> 2cm shortened
location = lateral 1/3 fractures - medial to CC ligaments are most unstable and have highest risk of nonunion
What is the number needed to treat
the number to prevent one bad outcome
What is hastings classification?
Dorsal PIP dislocation
-
Type I-Stable
- <30%; stable
-
Type II-Tenuous
- 30-50%-if reducible in flexion, dorsally based extension block splint
-
Type III-Unstable
- >50%-ORIF, hamat autograft, or volar plate arthroplasty
- Becomes unstable after 40% because they loose the attachments of the collaterals

Compare TEA and ORIF for distal humerus fractures
- No difference in complication rate
- Negligable data to suggest TEA decreases reoperation
- Main difference is that TEA has improved functional outcomes (Level 1 evidence)
What are the common compliations of halo
-
Loosening (36%)
- pins placed more cranial = more loosening
- just above pinna at equator of head
- 0.5cm above brow
- ring should be closer to head
- pins should engage at 90 deg angle
- metal rings better than graphite ring
- pins placed more cranial = more loosening
-
Infection (20%)
- especially with anterior pin in temporalis fossa because
- treat infection with oral antibiotics if pin not loose
- if infection with loose pin then remove pin
-
Discomfort (18%)
- treat by loosening skin around pin
- Dural puncture (1%)
- Crainal nerve VI palsy

Appropriate measures to deal with scare resources
- Choosing interventions known to be beneficial on the basis of evidence of effectiveness.
- Minimizing the use of marginally beneficial tests, such as the diagnostic zebra-hunt.
- Minimizing the use of marginally beneficial interventions, such as the latest generations of antimicrobials for common infections.
- Seeking the least costly tests or treatments that will accomplish the diagnostic or therapeutic goal.
- Using the natural queue, treating patients in order of appearance unless morally relevant considerations of need and benefit require modification of this approach. - apparently this is flawed
- Ranking patients with whom you have an established patient-doctor relationship ahead of unknown or future patients.
- Supporting rather than opposing reasonable efforts to conserve health care resources.
- Avoiding manipulation of the rules of the health care system to give unfair advantage to your own particular patients.
- Resolving conflicting claims for scarce resources justly, on the basis of morally relevant criteria of need and benefit.
- Employing fair and publicly defensible procedures for resolution of conflicting or competing claims.
- Seeking resolution of unacceptable shortages at the level of hospital management (meso allocation) or through political action at the level of government (macro allocation).
- Informing your patients of the impact of cost constraints on care in a humanistic way, as a matter of respect for persons. Embittered blaming of administrative or governmental systems during discussions with the patient at the point of treatment should be avoided.
- Developing guidelines for individualization in the face of uncertainty in order to promote a reasonable balance between individual choice and systemic cost control.
What is the prognosis of a neonatal brachial plexus injury?
90% resolve by 2 years
Recovery of biceps by 2 months is good prognosis
Clinical findings associated with muchopolysaccharoidosis
- typically none at birth. After a period of normal growth
- coarse facial features
- fullness of skin/brows
- enlarged tongue
- retained epicanthal folds
- short neck
- hydrocephalus
- corneal clouding
- inguinal/umbilical hernias
- hepatosplenomegaly
- otitis media, conductive hearing loss
- chronic resp tract infections
- cardiac d/o, carpal tunnel syn.

What nerve is most at risk with the FCR approach?
palmar cutaneous branch of the median nerve
What it the treatment for traumatic axillary nerve plasy
monitor, most will resolve on their own
EMG at 3 months to assess recovery with operative exploration if no evidence of recovery
NOTE - stabs wounds should be explored eariler, and post-surgical can consider EMG eariler
Diagnosis?

multiple hereditary exostosis (MHE)
- mutations affect the prehypertrophic chondrocytes of the physis
- genetics
- autosomal dominant
- mutations in EXT1, EXT2, and EXT3 genes (tumor suppressor genes)
-
EXT1 mutation have a more severe presentation compared to patients with the EXT2 mutation including
- higher rate of chondrosarcoma
- more exostoses
- more limb malalignment with less forearm and knee range of motion
- more pelvic and flatbone involvement
-
prognosis
- 5%-10% malignant transformation to chondrosarcoma in patients with MHE
- proximal lesions more likely to undergo malignant transformation than distal lesions
- most common location of secondary chondrosarcoma is the pelvis (usually occur as low-grade chondrosarcomas)
When are you most likely to injury superior gluteal nerve?
Glut med split with hardinge
Common tendon transfers for RA?
- EIP to EPL
- EIP to EDC5
- EDC4/5
- EIP to EDC5
- 3/4 side-side
- EDC3/4/5
- 2/3 side-side
- EIP - 4/5 side-side
- EDC2/3/4/5 without EIP
- use FDS
What factor is important to outcome of a PIP fracture-dislocation
- reduced joint is the most important thing
- anatomic reduction is less important
What is CREST syndrome
- Member of the Scleroderma family
- Calcinosis
- Raynaud phenomenon
- Esophageal dysmotility
- Sclerodactyly
- Telangiectasia

What are the pros and cons of using plaster?
-
Pros
- decrease pressure sore
- better ability to conform to limb
-
Cons
- low strength to weight ratio
- poor resistance to water
What is the best predictor of OA in an ankle fracture?
posterior malleolus fracture
What is true about BMP2 in open tibia fractures?
lower need for future bone graft
lower rate subsequent soft tissue
lower infection rate (only in Gustilo 3 pattern)
Indications for exploration of the radial nerve
- Open fracture
- High-velocity gunshot or penetrating injury
- Vascular injury
- Nerve deficit after closed reductiona Distal third (Holstein-Lewis) fractures
Pathology of scapular winging
- Serratus anterior - medial
- long thoracic (C5, 6, 7)
- Trapezius - lateral
- accessory
- Rhomboids - lateral
- dorsal scapular
- Treatment
- trapezium strengthening
- eden lange transfer - lateralize levator scapulae and rhomboids
- scapulothoracic fusion
Indications for delayed closure with VAC or bead pouch
- limited soft tissue viability
- lack of soft tissue coverage
- severe contamination
- Note - bead pouch or abx PMMA can significantly decreased risk of infection with delayed closure
What are the advantages and disadvantages of a single incision technique for distal biceps?
asthetic
less HO
10% improved strength with double
more often LCFN traction injury with single
Prevention of HIV transmission
always double glove
waterproof barriers
instrument tie or staples
pass sharp instruments in a bowl
JAAOS 1996
What are the blocks to a lateral subtalar dislocation?
posterior tibialis tendon
flexor hallucis longus
flexor digitorum longus
Acceptable criteria for distal radius malunion?

Describe the retroperitoneal approach
- Considerations
- transperitoneal has a higher risk of retrograde ejaculation (superior hypogastric plexus)
- if you go from left it’s easier, because easier to mobilize arteries rather than frail vessels
- Common Iliac branch at L4
- Incise the rectus and transversalis
- Find the arcuate line (fasica of the rectus); incise it and use it to retract the peritoneum
- Iliolumbar vessles branch off the internal iliac and need to be ligated for exposure to L4/5
- For exposure to L5/S1 the median sacral artery needs to be identified and ligated
What is the classficiation of thumb hypoplasia?
I - minimal
II - hypoplasia of musculature
IIIA - tendon abnormal, hypoplastic MC, stable CMC
IIIB - tendon abonormal, hypoplastic MC, unstable CMC
IV - floating thumb
V - absent thumb
What is the classification for lesser arc injuries?
Purely ligamentous - Mayfeild
Stage 1 - SL ligament
Stage 2 - space of poirer (lunocapitate lig)
Stage 3 - UTCC/UL
Stage 4 - lunate dislocation (dorsal radiolunate ligament)
What is the treatment of an adult galeazzi fracture?
- Usually operative, requires operative fixation as it requires anatomic fixation of the DRUJ
- volar approach to the radius
- restoration of the radial bow is key
- dorsal approach to the DRUJ
- make sure to examine TFCC if does not reduce with the radius
- typically avulsed off the ulna
- volar approach to the radius
- Treatment of the ulna
-
immobilization in supination (6 weeks)
- indicated if DRUJ stable following ORIF of radius
-
percutaneous pin fixation
- indicated if DRUJ reducible but unstable following ORIF of radius
- cross-pin ulna to radius in supination
- examine the TFCC
- leave pins in place for 4-6 weeks
-
open surgical reduction
- indicated if reduction is blocked
- suspect interposition of ECU Tendon
- Examine and repair TFCC if still unstable
-
open reduction internal fixation
- indicated if a large ulnar styloid fragment exists
- fix styloid and immobilize in supination
-
immobilization in supination (6 weeks)
What are the clinical features of larsen syndrome?
- Genetics - autosomal dominant (AD) and recessive (AR) inheritance patterns
- AD linked to a mutation of the gene encoding filamin B
- AR linked to carbohydrate sulfotransferase 3deficiency
- Normal intellegence
- Multiple dislocations (hyperlaxity)
- clubfoot
-
cervical kyphosis (60%)
- clinical important because often requires fusion for instability
- can present as myelopathy or with UE weakness
- scoliosis
- spatulate thumbs

What are causes of a swan neck finger?
***imbalance of the musculature
FDS tear - overpull of FDP
mallet finger - ext at PIP
intrinsic contracture
MCP volar subluxation

Pathology of this hand and tests

- Intrinsic minus hand (or tight extrinsics)
-
causes
-
ulnar nerve palsy
- cubital tunnel syndrome
- ulnar tunnel syndrome
-
median nerve palsy
- Volkmann’s ischemic contracture
- leprosy (Hansen’s disease)
- failure to splint the hand in an intrinsic-plus posture following a crush injury
- Charcot-Marie-Tooth disease (hereditary motor-sensory neuropathy)
- compartment syndrome of the hand
-
ulnar nerve palsy
-
Pathoanatomy
-
loss of intrinsics
- leads to loss of baseline MCP flexion and loss of IP extension
-
strong extrinsic EDC
- leads to unopposed extension of the MCP joint
- remember the EDC is not a significant extensor of the PIP joint
- most of the MCP extension forces on the terminal insertion of the central slip come from the interosseous muscles
-
strong FDP and FDS
- leads to unopposed flexion of the PIP and DIP
-
loss of intrinsics
-
Tests
- ulnar nerve worse in 4/5
- median nerve worse in 2/3
- if the MCP is flexed, the IP joints will extend
- opposite of bunnels test
What is your cutoff for bunions?
IMA <15, HVA <30 = distal
IMA > 15, HVA > 30 = proximal
hypermobile first ray = lapidus
arthritis or progressive = fusion
congruent with high DMMA (>20) = consider double osteotomy

What is frederichs disease?
aseptic osteonecrosis of the medial clavicle
red joint
ESR/CRP/WBC/Rheum work-up are normal
MRI - necrotic bone islands

Classification of Hallux Rigidus
Cougling and Shurnas
- Changes the arch of use due to dorsal osteophytes, >10 deg of motion is not needed for a normal gait, and in fact push-off improves following fusion in these patients
- Pathology due to increased strain across the MTP joint
-
Grade 0
- Stiffness with normal XR
-
Grade 1
- mild pain at extremes of motion
- mild dorsal osteophyte, normal joint space
-
Grade 2
- moderate pain with range of motion increasingly more constant
- moderate dorsal osteophyte,
-
Grade 3
- significant stiffness, pain at extreme ROM, no pain at mid-range
- severe dorsal osteophyte, >50% joint space narrowing
-
Grade 4
- significant stiffness, pain at extreme ROM, pain at mid-range of motion
- same as grade III

What are the deforming forces on this fracture?

Bennet fracture
Abductor pollicis longus
extensor pollicis longus
adductor pollicis

What are the features of unilateral facet dislocation?
flexion/distraction injury, with rotation
4/5 or 5/6
25% anterior translation (50% is bilateral)
SP don’t line up on AP
bow-tie sign

What structures are present in each of the acetabular quadrants for screw placement - which is safe and which is dangerous?

Other indications for radial head arthroplasty?
-
Indications
- comminuted radial head fracture
- nonunion/maluion
- instabilty (essex-lopraseti)
- rheumatoid or osteoarthritis
- tumour
-
Contraindications
- repariable fracture
- capitellar arthrosis

What is the classification for monteggia fractures?
- BADO
- I - anterior
- Pronation injury
- Reduced with flexion and supination
- II - posterior
- Supnation injury
- Reduced with extension and pronation
- III - lateral
- Direct lateral injury
- Reduced with flexion and supination
- IV - # rad/ulna

What is the treatment of thumb hypoplasia?
I - no treatment
II/IIIA - tendon correction, oppenoneplasty with UCL recon
IIIB - ablation with pollicization OR 2nd toe/toe joint transfer
IV - ablation with pollicization OR 2nd toe transfer
V - pollicization or 2nd toe transfer

What are the foot deformities by myelomeningocele level?

Key points of metatarsus primus varus
-
Adduction deformity of the great toe characterized by
- deformity at metatarsophalangeal joint
- short thick 1st metatarsal
- firm band-like abductor hallucis muscle
-
Associated conditions
- often associated with polydactyly – duplication of the great toe
- Must be differentiated from metatarsus adductus
- Lateral border of the foot is normal
- More rigid than MA
- Early casting is used, associated with hallux valgus
- Severe deformity is indication for osteotomy
What are the bands associated with dupytrens
- pretendinous band
- spiral band
- natatory band/ligament
- causes contracture of the web space lateral and reduces abduction
- lateral digital sheet
- Grayson’s ligament
pulls the NV strucutre central and superficial

Treatment of recurrent posterior shoulder dislocation
- 50% are caused by trauma
- More common to have recurrent subuluxation that wears the posteior gleniod
- May present with recurrence of pain more than instability, but can be quite limited
- Some are traumatic, some are habitual
- habitual will not do well with surgery
- Physical
- sulcus, jerk, posterior stress, load and shift
- Most will benefit from strengthening dynamic stabilizers
- Can benefit from surgery when nonsurgical fails (ideally recurrent, post-traumatic, unilateral)
-
Posterior Bankart lesion
- Arthroscopic or open posterior Bankart repair
-
Excessive capsulolabral laxity
- Arthroscopic or open posterior capsular shift ± rotator interval closure
-
Glenoid erosion
- Posterior glenoid bone grafting
-
Increased glenoid retroversion >20
- Posterior opening wedge glenoid osteotomy
-
Posterior Bankart lesion
-
Complications
- recurrence
- subscapular nerve injury
- if you split the IS more than 1.5cm medially
- stiffness from overtightening
- may be associated with future OA

What are the types of nerve injury?

Classification and treatment for this fracture?

HASTINGS
-
Type I-Stable
- <30%-treat with dorsally based extension block splint
-
Type II-Tenuous
- 30-50%-if reducible in flexion, dorsally based extension block splint
-
Type III-Unstable
- >50%-ORIF if possible, hamat autograft/dynamic ex-fix, or volar plate arthroplasty
-
Comminuted type C
- Dynamic distraction external fixation
-
Chronic
- fusion

What is fredrichs disease?
AVN of the medial clavicle
atraumatic dislocation
often occurs in females
medial bowing of the clavicle

Anatomy of the Spinal Column
-
Descending Tracts (motor)
-
lateral corticospinal tract (LCT)
- UMN are in the lateral portion of the white matter
- They synapse with anterior horn cells (ventral) in the grey matter, and more central portion of the spinal cord
-
ventral corticospinal tract
- Rubriospinal
- smaller, less axons
- voluntary muscle control
- primarily flexion (decorticate)
- extra-pyramidal
- vestibulospinal
- extension
- extrapyramidal
- postural
- Rubriospinal
-
lateral corticospinal tract (LCT)
-
Ascending tracts (sensory)
- Synapse with the doral root ganglion and enter via the posterior horn of the grey matter (doral)
-
dorsal columns
- deep touch
- vibration
- proprioception
-
lateral spinothalamic tract (LST)
- pain
- temperature
-
ventral spinothalamic tract (VST)
- light touch

What is the treatment for swan neck deformity
-
Double ring splint
- can try this first always
-
volar plate advancement and PIP balancing with central slip tenotomy
- indications
- progressive deformity
- technique
- address volar plate laxity with volar plate advancement
- correct PIP joint muscles imbalances with either
- FDS tenodesis indicated with FDS rupture
- spiral oblique retinacular ligament reconstruction
- central slip tenotomy (Fowler)
- indications
-
DIP Arthrodesis
- Dorsal approach
- Extensor tenodesis with capsulotomy

What is the classification for clavicle fractures?
Group 1 - middle, most common
Group 2 - distal (Neer)
1 - lateral (non-op)
2a - medial (sux)
2b - medial with conoid (sx)
3 - intra-articular
4- physeal
5 - comminuted
Group 3 - proximal (anterior, posterior)

Windswept hand deformity characteristics?
**Occurs in distal arthrogryposis
- Flexion, adduction of thumb (thumb in palm)
- narrowing first web space
- flexion/ulnar deviation of fingers

What is the veiw of choice for traumatic SC dislocation
obtain serendipity views ( beam at 40 cephalic tilt)
anterior dislocation - affected clavicle above contralateral clavicle
posterior dislocation - affected clavicle below contralateral clavicle

What are the 5 ligaments of the interosseous membrane of the forearm
central band is key portion of IOM to be reconstructed
accessory band
distal oblique bundle
proximal oblique cord
dorsal oblique accessory cord

What is the jupiter modification of monteggia fractures
- A - intra-articular coronoid
- B - extra-articular coronoid
- C - extra-articular shaft
- D - intra-articular comminuted

What is an appropriate technique for valgus intertroch osteotomy
- indicated in patients after femoral neck nonunion
- verticle fracture (Pawel C)
- can be done even in presence of AVN, as long as not severely collapsed, but may want to consider MRI preop
- Plan your osteotomy for the fracture to be 30 deg from horizontal
- choose appropriate blade plate
- First K-wire for blade goes into the head at your planned site
- second K-wire at the osteotomy should be 2 cm distal to this
- Try not to medialize the canal
- decreases offset, reduces abductor strength
- increase joint reaction force

Etiology and Pathoanatomy

Swan Neck Deformity
-
Characterized by
- hyperextension of PIP
- flexion of DIP
-
Caused by
- lax volar plate
- imbalance of muscles forces on PIP (extension force > flexion force)
-
Injuries include
- MCP joint volar subluxation (rheumatoid arthritis)
- mallet finger
- FDS laceration
- intrinsic contracture
-
Primary lesion is lax volar plate that allows hyperextension of PIP
- trauma
- RA
- Hyperlaxity
-
Secondary lesion is imbalance of forces on the PIP joint (PIP extension forces that is greater than the PIP flexion force)
-
mallet injury
- leads to transfer of DIP extension force into PIP extension forces
-
FDS rupture
- leads to unopposed PIP extension with an intact FDP
-
intrinsic contracture
- tethering of the lateral (collateral) bands by the transverse retinacular ligament as a result of PIP hyperextension.
- if the lateral (collateral) bands are tethered, excursion is restricted and the extension force is not transmitted to the terminal tendon, and is instead transmitted to the PIP joint
-
MCP joint volar subluxation
- caused by rhuematoid arthritis
-
mallet injury

Describe powers ratio
Basion to Posterior C1 / Opisthion to Anterior C1
(CD/BA)

Sites of entrapment of this nerve

ULNAR CLAW HAND
-
Associated conditions
- cubitus varus or valgus deformities
- medial epicondylitis
- burns
- elbow contracture release
-
most common
- between the two heads of FCU/aponeurosis (most common site)
- within arcade of Struthers (hiatus in medial intermuscular septum)
- between Osborne’s ligament and MCL
- less common
- medial head of triceps
- medial intermuscular septum
- medial epicondyle
- fascial bands within FCU
- anconeus epitrochlearis (anomalous muscle from the medial olecranon to the medial epicondyle)
- aponeurosis of FDS proximal edge

Classification of this injury

Jersey Finger
- Refers to an avulsion injury of FDP from insertion at base of distal phalanx
- a Zone I flexor tendon injury
- FDP muscle belly in maximal contraction during forceful DIP extension
-
Ring finger involved in 75% of cases
- during grip ring fingertip is 5 mm more prominent than other digits in ~90% of patients
- Weaker insertion point
- Least independent movement
- __Proximal to A5 there is a dual vascualr supply, treatment will depend on whether one or both are disrupted
- Vinculum Longus Profundus (VLP)
- Vinculum Longus Superficialis (VSP)
-
Leddy Packer Classification
-
Type I
- FDP tendon retracted to palm
- Leads to disruption of the vascular supply
- Prompt surgical treatment within 7 to 10 days
-
Type II
- FDP retracts to level of PIP joint
- VLP intact
- Attempt to repair within several weeks for optimal outcome
-
Type III
- Large avulsion fracture limits retraction to the level of the DIP joint (A4)
- All blood supply intact
- Attempt to repair within several weeks for optimal outcome
-
Type IV
- Osseous fragment incarcerated in A4 and simultaneous avulsion of the tendon from the fracture fragment (“Double avulsion” with subsequent retraction of the tendon usually into palm)
- If tendon separated from fracture fragment, first fix fracture via ORIF then reattach tendon as for Type I/II injuries
-
Type V
- boney avulsion with comminution
-
Type I

Cervical kyphosis associated with larsen syndrome; what is the treatment?
posteior stabilization with halo for 3 months; prevents neurological deficit
early recognition is the key

What are the zones of articular cartilage
-
Superficial zone (tangential zone)
- Type II collagen orientation is parallel to joint
- Has flattened chondrocytes, condensed collagen fibers, and sparse proteoglycans
- only zone where articular cartilage progenitor cells have been found
-
Intermediate zone
- Type II collagen has an oblique or random organization
- Is the thickest layer with round chondrocytes, and abundant proteoglycan content
-
Deep layer (basal layer)
- Type II collagen is perpendicular to joint and crosses tidemark; has the highest concentration of proteoglycans
- Round chondrocytes arranged in columns
-
Tidemark
- Is deep to the basal layer and separates the true articular cartilage from the deeper cartilage that is a remnant of the cartilage anlage, which participated in endochondral ossification during longitudinal growth in childhood.
- The tidemark divides
- the superficial uncalcified cartilage from the deeper calcified cartilage
- division between nutritional sources for the chondrocytes
- The tidemark is found only in joints
- Most prominently in the adult and nongrowing joint
- Subchondral Bone

What are injury patterns suggestive of PM of PL rotatory instability of the elbow?

What is the reduction maneuver for a bennet fracture?
-
Forces on fracture
- Volar oblique ligament
- Abductor pollicis longus (PIN) - base
- Extensor pollicis longus (PIN) - base
- Adductor pollicis (Ulnar) - shaft
-
Reduction maneuver
- Traction
- Abduction
- Extension
- Pronation

What are the restraints to the shoulder
-
SGHL
- restraint to inferior translation at 0° degrees of abduction (neutral rotation)
-
MGHL
- resist anterior and posterior translation in the midrange of abduction (~45°) in ER
-
IGHL
-
posterior band IGHL
- most important restraint to posterior subluxation at 90° flexion, abduction and IR
- tightness leads to internal impingement and increased shear forces on superior labrum (linked to SLAP lesions)
-
anterior band IGHL
- primary restraint to anterior/inferior translation 90° abduction and maximum ER (late cocking phase of throwing)
- anchors into anterior labrum
- forms weak link that predisposes to Bankart lesions
- primary restraint to anterior/inferior translation 90° abduction and maximum ER (late cocking phase of throwing)
-
superior band IGHL
- most important static stabilizer about the joint
- 100% increased strain on superior band of IGHL in presence of a SLAP lesion
-
posterior band IGHL
-
Coracohumeral ligament (CHL)
- limits posterior translation with shoulder in flexion, adduction and internal rotation
- limits inferior translation and external rotation at adducted position

Camptodactyly - pathology and treatment options
-
Pathology - usually sporatic
- abnormal lumbrical insertion/origin
- abnormal (adherent, hypoplastic) FDS insertion
- other less common causes include
- abnormal central slip
- abnormal extensor hood
- abnormal volar plate
- skin, subcutaneous tissue, or dermis contracture
-
Non-operative treatment is favoured
- most will respond to passive splinting
-
FDS tenotomy +/- FDS transfer
- reserved for cases of progressive deformity leading to functional impairment
- technique
- must address all abnormal anatomy
- passive (correctable) deformities
- FDS tenotomy, or
- FDS transfer to radial lateral band if full active PIP extension can be achieved with MCP flexion
-
osteotomy vs. arthrodesis
- severe fixed deformities

What is the characteristic pattern of this injury?

lumbar burst fracture
- centripital disruption of the vertebral body
- anterior wedging
- laminar fractures abut the spinous process
- increased interpedicular distance
- retropulsion of the superior endplate
Pathology of this hand and tests

- intrinsic plus
-
causes
- trauma
- rheumatoid arthritis (secondary to distal joint malalignment)
-
pathology
- spastic intrinsics
- lead to flexion of the MCP and extension of the IP joints
-
weak EDC
- fails to provide balancing extension force of MCP
-
weak FDS & FDP
- fails to provide balancing flexion force on PIP and DIP
- spastic intrinsics
-
Bunnell test - for intrinsic
- diff between intrinsic and extrinsic
- test is positive when there is less PIP flexion with MCP extension than when the MCP is flexed

What are the indications pin the other side?

endocrinopathy
<10 with open triradiate
lack of ability to follow-up
What are the soft tissues disrupted with PIP dislocation and what are the blocks to reduction.
- Collaterals may also be disrupted
-
Dorsal
- Volar plate - loose the static restraint
-
Volar
- lateral bands/central slip

The third is refered to as a pilon fracture
Hypovolemic shock, ATP depleted. What happens intracellular?
Increased sodium, decreased potassium, increased water
Cellular level – O2 demand > O2 supply – cellular hypoxia

What is condensing osteitis
- sclerosis and englargement of the medial clavicle
- women, 30-40, unilateral
- most respond to NSAIDS

Associated conditions with this deformity

-
Note that these are not mutally exclusive and you should always screen for all of them; see baby below with thumb hypoplasia, fanconi’s anemia; also has several features of VACTERL
- CBC
- echo
- Renal U/S
- full head-toe exam
- These patients should be treated with a team based approach - invovle genetics, pediatrics and all necessary specialties
-
TAR
- autosomal recessive condition with thrombocytopenia and absent radius
- thrombocytopenia fluctuants over time
- exaccerbated by infection, stress
- presents in first week of life
- purpura, petechiae
- intracranial hemmorhage - fatigues, lethary, difficulty feeding
- low platlets, normal chormosomes
- Basic first aid, platelet transfusion
- different in that thumb is typically present
-
Fanconi’s anemia
- autosomal recessive condition with aplastic anemia
- can get hemmorhage, infection, neoplasia
- Work-up
- CBC - pancytopenia or complete aplasia
- Diagnosis - Fanconi screen and chromosomal breakage test to screen
- treatment is bone marrow transplant
-
Holt-Oram syndrome
- autosomal dominant condition characterized by cardiac defects
- ASD most common
- diagnoses with blood test and genetics
- autosomal dominant condition characterized by cardiac defects
-
VACTERL Syndrome
- vertebral anomalies
- anal atresia
- cardiac abnormalities
- tracheoesophageal fistula
- renal agenesis
- limb defects
-
VATER Syndrome
- vertebral anomalies, anal atresia, tracheoesophageal fistula, esophageal atresia, renal agenesis)

What are the important clinic aspects of multiple enchondromas (not MHE)
-
Ollier’s disease (multipe enchondromatosis)
- no genetic predisposition has been identified
- multiple enchondromas in long bone diaphysis
- 10-30% chance of malignant transformation into chondrosarcoma
- however associated with high rate of both skeletal and non-skeletal malignancies
- involved bones are dysplastic
-
Maffucci’s syndrome
- no genetic predisposition has been identified
- multiple enchondromas and soft-tissue angiomas
- 100% chance of malignant transformation into chondrosarcoma
- increased risk of visceral malignancies (astrocytoma, GI malignancy)

What are the associated mobility for myelomeningocele levels?

What is ture about congenital hallux varus?
Atavastic great toe
short, thick, first MT
associated with polydactyly
Often need to syndactylize to second toe to control deformity
MT osteotomy +/- lengthening
release addutor hallucis

What is the definative treatment for a parosteal osteosarcoma?
- wide resection
- no role for chemo unless there is a high grade component
- 30-40 yo
- surface of bones, usually the distal femur
- less aggressive than periosteal osteosarcoma

What is typical and how do you treat fibrosarcoma?
> 50 yo (worse prog over 40)
pain, swelling, path #
distal femur, proximal tibia
XR - purely lytic wth moth eatten appearance, no evidence of codman’s triangle or osseous matrix
Treat as if osteosarc
Chest XR - rule out lung mets
Local staging with MRI
Chemo - doxyrubicin and cysplatinin
Re-stage
Limb salvage surgery
Chemo

What is sternoclavicular hyperostosis and what is associated with it?
SAPHO
pustulitic arthro-arthritis
soft tissue ossification between the clavicles
palmoplantar pustolosis and severe acne
Males 40-50, severe pain and redness over SC joint
often bilateral

What is the most common location for compression of the suprascapular nerve?
- suprascapular notch apparently more common
- due to confinement and limited mobility
- nerves to supraspinatous are adhered to periosteium
- leads to more functional deficiet
- Other site is spinoglenoid notch
- IS is more compenstated by deltoid
- Etiology
- cysts
- transverse scapular ligament
- fracture callus
- Can be associated with
- RC tear, AC OA, adhesive capsulitis, GH OA, parsonage turner syndrome
- XR - stryker notch view
- EMG/NCS will confirm pathology of location of the entrapment
- Get MRI and treat pathology
- trace the nerve
- look for mass occupying lesions
- compare SS and IS atrophy

Diagnosis? Classification? Indications/Options for surgery?

Radial Head Fracture
- Physical
-
check ROM
- 30-130 flex-ex
- 45-45 sup-pro
- check the pin
-
check ROM
-
Imaging
- can get a greenspan view to help assess
- 45 deg oblique center over the RC joint
- CT
- can get a greenspan view to help assess
-
Classification - Mason Allen
- Type 1 - nondisplaced
- Type II - partial head fx
- Type III - complete head
- Type IV - radial head fx with elbow dislocatoin
-
short period of immobilization followed by early ROM
- Nondisplaced, stable (30-130)
- no mechanical block
- complications
- nonunion
- new studies have shown a higher rate of nonunion in nonoperative managmeent than previously expected
- nonunion
-
ORIF
-
Indications
- Simple fracture
- Mechanical block
- technique
- plate in safe zone
- countersink screws in articular surface
-
Indications
-
Fragment Excision (partial excision)
- indicated if fragment
- Cannot be a part of the PRUJ
- complications
- even small fragment excision may lead to instability
-
radial head replacement
- indications
- for comminuted fracture with 3 or more fragments
- complications
- overstuffing of joint that leads to capitellar wear problems and malalignment instability
- indications
-
radial head resection
-
indications
- older patients with limited demands
- in a delayed setting for continued pain of an isolated radial head fracture
-
contraindications
- forearm ligament injury (identify with radius pull test)
- coronoid fracture
- MCL deficiency
-
complications
- muscle weakness
- wrist pain
- valgus elbow instability
- heterotopic ossification
- arthritis
-
indications

What is the dalbet classification of pediatric femoral neck fractures?
-
Type I Transphyseal (10%)
- IA - without dislocation of epiphysis from acetabulum
- IB, with dislocation of epiphysis
- Risk of ANV = 90-100%
-
Type II Transcervical (40-50%)
- AVN - 50%
- Nonunion - 15%
-
Type III Basicervical (30-35%)
- AVN - 25%
- Nonunion - 15-20%
-
Type IV Intertrochanteric (10-20%)
- AVN - 10%
- 5%

What are the components of proteoglycans?
- makes up 10 to 15% of cartilage
- functions to provide compressive strength and attract water
- produced by chondrocytes
- composed of GAG subunits
- chondroitin sulfate
- keratin sulfate
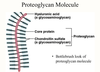
Boundaries and zones of guyons canal?
-
Boundaries of Guyon’s canal
- Floor
- Transverse carpal ligament, hypothenar muscles
- Roof
- Volar carpal ligament
- Ulnar border
- Pisiform and pisohamate ligament, abductor digiti minimi muscle belly
- Radial border
- Hook of hamate
- Floor
-
Zones of Guyon’s canal
- Zone 1
- Proximal to bifurcation of the nerve
- Ganglia and hook of hamate fractures
- Mixed motor and sensory
- Zone 2
- Surrounds deep motor branch
- Ganglia and hook of hamate fractures
- Motor only
- Zone 3
- Surrounds superficial sensory branch
- Ulnar artery thrombosis or aneurysm
- Sensory only
- Zone 1

Diagnosis? Differential? Treatment?

Torticollis
-
Deformity in the SCM
- head tilts towards the affected side and rotates away
-
Pathophysiology
- some studies suggest association with intrauterine compartment syndrome of SCM
- non-SCM causes include
- ophthalmologic
- vestibular
- congenital
- traumatic
- tumors
-
Associated conditions
- Packing disorders
- DDH (5 - 20% association)
- metatarsus adductus
- traumatic delivery
- plagiocephaly (head assymetry)
- congenital atlanto-occipital abnormalities
- Packing disorders
-
Differential
- Rotatory atlanto-axial instability / Grisel’s disease
- Klippel-Feil syndrome
-
Imaging
-
XR/CT
- if no palpable mass
- to rule out AARD/klippel-fiel
- US can show lesion in SCM
-
XR/CT
-
Treatment
-
passive stretching
- condition present for less than 1 year
- limitation less than 30°
- should include lateral head tilt away from the affected side and chin rotation toward the affected side (opposite of the deformity)
- 90% response with-in one year
-
Z plasty lengthening or distal bipolar release of SCM
- > 1 year
- > 30°
-
passive stretching
What diseases have occular associations?
Homocysteinuria has inferior lens dislocation
Marfan’s has superior lens dislocation
Neurofibromatosis has Lisch nodules in the iris.

Iatrogenic causes of this deformity

- overcorrection of 1st IMA
- excessive lateral capsular release with overtightening of medial capsule
- overresection of medial first metatarsal head
- lateral sesamoidectomy
Diagnosis? Blocks to reduction? Treatment?

-
Volar IP dislocation
- always has a central slip rupture
-
late deformity
- Boutinerre - from central slip rupture
-
Blocks to reduction
- one collateral
-
central slip and lateral band
- __button holes between the two
-
Treatment
-
buddy tape for 6-8 weeks if reducible
- if fracture < 40%
- no associated fracture
-
ORIF or CRPP
- >40% articular surface
-
buddy tape for 6-8 weeks if reducible
What is the anatomy of the medial circumflex artery
Comes underneath quads femoris, travels superiorly in front of the ERs, except obturator externus because it is a more antereiror structure

What do you need to consider in the treatment of syndactyly of the hand

-
Timing
-
syndactyly
- perform at ~ 1 year of age
- controversial
-
acrosyndactyly
- perform in neonatal period
- if multiple digits are involved perform procedure in two stages to avoid compromising vasculature
- early surgery allows this
- thumb and index at
- release digits with significant length differences first to avoid growth disturbances
-
syndactyly
-
technique
- zigzag flaps are created during release to avoid longitudinal scarring
- a nailbed can be re-created in complete syndactyly
-
complications
-
Web creep
- most common complication of surgical treatment
- reconstruct web space with local skin flaps
- Nail deformities
- Scar
-
Avascular digit
- __never operate threw both sides of the digit
-
Web creep

Diagnosis? Important Concepts?

- Epiphyseal, benign aggressive
- can get cortial thinning with neocortex and soft tissue invasion
- destruction caused by activation of osteoclasts
- 30-40 yo (ABC is 20)
- Location
- 50% knee
- 10% sacrum
- distal radius
-
Medical treatment
- bisphosphanates
- denosemab
-
extensive curettage and reconstruction (with adjuvant treatment)
- challenge - remove lesion while preserving joint and providing support to subchondral joint
- extensive exterioration (removal of a large cortical window over the lesion) is required
- 10-30% recurrence with curettage alone verses 3% with adjuvant treatment (phenol, hydrogen peroxide, argon beam, etc)
- can fill lesion with bone cement or a_utograft/allograft bone_
-
hand lesion treatment is controversial
- if no cortical breakthrough treat with curettage and cementing
- if significant cortical breakthrough consider intercalary resection (with free fibular graft) vs. amputation

What are the characteristics of carpal synostosis/coalition?
- Blacks > whites
- usually carpometacarpal fusion failure of cavitation 4-8 wks gestation
- usually bilateral
- 90% between lunate-triquetrum

What is true about the blood supply to the humeral head
- LHB can help locate the asecnding branch and localize the tuberosity
- ascending branch is just posterior and lateral to the LHB
- ascending branch of the anterior circumflex is the primary blood supply to the femoral head
- the second supply is the posterior circumflex which wraps around the medial calcar

Pathology of this XR?

VISI - volar intercalated segmental instability
-
LT ligament injury occurs with
- wrist hyperextension or
- extension and radial deviation
-
2 important ligaments tears
-
lunotriquetral (intrinsic)
- volar - strongest
- dorsal - more important rotation
- Dorsal radiocarpal (extrinsic)
- volar long and short radioluntae ligaments - extrinsic that might also tear
-
lunotriquetral (intrinsic)
- scaphoid induces the lunate into further flexion while triquetrum extends
Diagnosis? Classification

Keinboch’s - Litchman Classification
-
Stage I
- No visible changes on xray, changes seen on MRI
- Immobilization
- NSAIDS
- No visible changes on xray, changes seen on MRI
-
Stage II
-
Sclerosis of lunate
- Ulnar negative - ulnar shortening
- Ulnar positive - Radial wedge, STT fusion
- Distal radius core decompression
- Revascularization procedures
-
Sclerosis of lunate
-
Stage IIIA
- Lunate collapse, no scaphoid rotation
- Same as Stage II above
- Lunate collapse, no scaphoid rotation
-
Stage IIIB
- Lunate collapse, fixed scaphoid rotation
- Proximal row carpectomy
- STT fusion
- Lunate collapse, fixed scaphoid rotation
-
Stage IV
- Degenerated adjacent intercarpal joints
- Wrist fusion
- proximal row carpectomy
- limited intercarpal fusion
- Degenerated adjacent intercarpal joints

Classification of syndactyly

-
Simple
- Only soft tissue involvement, no bony connections
-
Complex
- Side to side fusion of adjacent phalanges
-
Complicated
- Accessory phalanges or abnormal bones involved in fusion
- Complete vs. Incomplete
- Complete: syndactyly the skin extends to finger tips
- incomplete: skin does not extend to fingertips
Correlate growth velocity with menarche, apoyphyseal closure and the risser grade
