Lymphomas Flashcards
What is a lymphoma?
A malignancy of lymphoid cells based in lymphoid tissues such as the lymph nodes, spleen, thymus, or MALT. It may involve the marrow and blood secondarily.
B-ALL clinical presentation
Acute Several weeks of fatigue due to anemia Easy bruising due to thrombocytopenia Fever, signs of infection due to neutropenia May have pain in a single long bone, skin involvement
B-ALL workup
Peripheral blood smear: lymphoblasts CBC: anemia, thrombocytopenia, granulocytopenia Bone marrow: lymphoblasts are >20% of marrow cellularity
B-ALL flow cytometry
TdT+ CD19+ CD34+
B-ALL age of peak incidence
3 (FYI this is the time of peak B cell production in the bone marrow)
Does the presence of t(9;22) produce a good or bad prognosis?
Bad
T-ALL peak incidence
15
T-ALL clinical presentation
cough, shortness of breath, superior vena cava
T-ALL clinical presentation
usually presents as a large thymus mass with cough, shortness of breath, superior vena cava syndrome (swelling and redness of face and upper extremities)
T-ALL flow cytometry markers
TdT+ CD 2-8
Are ALLs agressive tumors?
Yup! Treat early, treat fast!
What are B symptoms?
fever night sweats weight loss
Relative to T or NK cells, why are germinal center B cells most likely to give rise to neoplasms?
B cells rely on somatic hypermutation and class switching to function properly. Since their genomes are designed to be able to change, they are also most likely to mutate in a malignant way.
What infections are associated with lymphoid neoplasms?
EBV HHV8 (kaposi sarcoma herpesvirus) HTLV-1 HIV H. pylori
CLL/SLL pathogenesis
Not entirely understood but thought to involve deletions
CLL workup (blood smear, bone marrow, etc)
Blood smear: increased numbers of small round lymphocytes, smudge cells
Bone marrow: aggregates of similar appearing tumor cells
Lymph nodes: diffusely infiltrated by small lymphocytes and patchy collections of larger, mitotically active cells known as proliferation centers.
CBC: lymphocytosis (lymphs > 5000)
CLL clinical presentation
Often asymptomatic
May present with weight loss, fatigue, anorexia, diffuse LAD, or hepatosplenomegaly
CLL flow cytometry
CD 5+
CD 10-
CD 20 +, CD 19+, CD23+
What does this CBC suggest?

CLL
lymphocytosis with everything else fairly normal
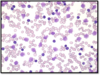
CLL
smudge cells
Does CLL always require treatment?
No, approx. 60% of patients with CLL never require treatment.
High lymphocyte count alone is not an indication to start treatment
What’s the significance of chromosome 17 in CLL?
Chromosome 17 is home to the p53 tumor suppressor gene. This is a common target for chemotherapy so CLL with deletions of this gene cannot be treated effectively with conventional chemo. They have a very poor prognosis.
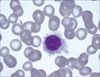
Hairy cell
Hairy cell leukemia
- A tumor of mature B cells expressing CD20 but not CD5 of CD10
- Associated with BRAF mutations
- Often presents with splenomegaly and cytopenia, especially monocytopenia, and infections (especially with mycoplasma)
- Peripheral blood shows “hairy cells”








