Hematology - First Aid Flashcards
What ingredients contribute to the formation of a purine?
Remember that guanine is the one with a ketone.

What ingredients contribute to the formation of a pyrimidine?
Remember that thymine has a methyl group.

Deamination of what nucleotide will form uracil?
Cytosine
Where in the purine and pyrimidine synthesis pathways do these antineoplastic/antibiotic drugs act: hydroxyurea, 6-mercaptopurine, 5-fluorouracil, methotrexate and trimethoprim?
Hydroxyurea: inhibits ribonucleotide reductase production of deoxynucleotides. 6-MP: blocks Gln-PRPP amidotransferase, preventing PRPP conversion to PRA. 5-FU inhibits thymidylate synthase, decreasing dTMP synthesis. Methotrexate inhibits FH2 reductase, decreasing dTMP synthesis. Trimethoprim only inhibits bacterial FH2 reductase.

A mother brings in her newborn boy complaining of lethargy, irritability and hyperventilation 36 hours after birth. Over the next 24 hours, the lethargy increased and progressed to coma requiring mechanical ventilation. Hemodialysis was started at 5 days and the child died after one week. Two of the mother’s four brothers died shortly after birth from encephalitis. Labs at 36 hours reveal high blood pH, low blood CO2 and low BUN. On day 5 high plasma ammonium, high glutamine, Arg/Citrulline undetectable and high orotic acid in the urine. What is the pathogenesis of this disease?
Ornithine transcarbamoylase (OTC) deficiency. When this enzyme is deficient, the carbamoyl phosphate originally produced for the urea cycle by CPS I cannot continue on in the urea cycle and backs up in the mitochondria. It goes into the cytoplasm to meet with Asp and CPS II takes it to carbamoyl aspartate, then to orotic acid, hence orotic aciduria. Upstream, CPSI isn’t as active from excessive amounts of carbamoyl phosphate and NH4+ builds up. This pushes the equilibrium of glutamine synthetase from glutamate to glutamine and Gln builds up.

A mother brings in her baby complaining of failure to thrive. Labs reveal orotic aciduria, megaloblastic anemia and normal serum ammonia levels. Further testing shows normal B12 and folate levels. How should you treat this child?
Hereditary orotic aciduria is a condition where UMP synthase is lacking and you get build up of orotic acid in the blood. Since they are not making UTP and CTP, they are not making pyrimidine nucleotides and erythropoiesis shuts down in the bone marrow. Giving the child uridine will inhibit CPS II, decrease the amount of orotic acid forming and increase UTP available for use in erythropoiesis.

What is one of the major causes of severe combined immunodeficiency disease (SCID) in kids that is autosomal recessive?
Adenosine deaminase deficiency. This is a defect in the purine salvage pathway that prevents conversion of adenosine to inosine. This results in excess ATP and dATP that feedback inhibits ribonucleotide reductase. This inhibition prevents DNA synthesis and results in a decreased lymphocyte count.

A mother brings in her 2 year old son complaining of retardation, self-mutilation and aggression. Physical exam reveals athetosis in the hands and a swollen big toe. Labs show hyperuricemia. What is most likely causing this child’s condition?
X-linked recessive disorder: Lesch-Nyhan syndrome. This is due to absence of HGPRT. When HGPRT is absent you cannot convert hypoxanthine to IMP or guanine to GMP. This results in excess uric acid production and de novo purine synthesis.

What are the enzymes indicated in the image below?

This is the purine salvage pathway: 1) HGPRT + PRPP is involved in conversion of guanine to GMP. 2) APRT + PRPP is involved in conversion of adenine to AMP. 3) Adenosine deaminase is involved in conversion of adenosine to inosine. 4) Xanthine oxidase is involved in the conversion of hypoxanthine to xanthine and xanthine to uric acid.
What are the three steps involved in polymerase chain reactions (PCR) in the lab?
1) Denaturation: DNA is denatured by heating into 2 separate strands 2) Annealing: while DNA cools, excess pre-made DNA primers anneal to a specific sequence on each strand to be amplified 3) Elongation: heat-stable (Taq) DNA polymerase replicates DNA sequence that follows each primer

Adding a fluorescent labeled DNA or RNA probe that binds to a specific gene site on a chromosome
FISH (Fluorescence in situ hybridization)
Deficiency in what enzyme can cause macrocytic, megaloblastic anemia and is associated with neural tube defects?
Folic acid. It is converted to FH2 by dihydrofolate reductase and then to FH4 by the same enzyme. FH4 is converted to N5,N10-methylene FH4, which is necessary for synthesis of dTMP. If dTMP is absent, DNA and RNA synthesis cannot proceed and erythropoiesis will stall, hence the anemia. N5,N10-methylene FH4 can also be reduced to N5-methyl FH4, which only participates in the reaction with B12 to convert homocysteine to methionine in the cycle that keeps SAM methylated.

What drugs can cause folate deficiency?
Sulfonamides in bacteria and methotrexate in humans. Phenytoin can also cause it.

A 69 year old man presents with fatigue and peripheral neuropathy. Peripheral blood smear shows a macrocytic megaloblastic anemia with hypersegmented neutrophils. Homocysteine and MMA levels are elevated. What are likely causes of this patient’s condition?
He has B12 deficiency, note high MMA and homocysteine levels. Deficiency is usually caused by malabsorption (tropical sprue, enteritis, Diphyllobothrium latum, Crohn’s) or lack of intrinsic factor (pernicious anemia or gastric bypass).

A 69 year old man presents with fatigue and peripheral neuropathy. Peripheral blood smear shows a macrocytic megaloblastic anemia with hypersegmented neutrophils. Homocysteine and MMA levels are elevated. What test would you do on this patient to determine the etiology of his B12 deficiency?
Schilling test: 1) Give a B12 shot to saturate hepatic B12 receptors 2) Give oral radiolabeled B12. If < 10% B12 is found in URINE, it means it was not absorbed and was excreted in the feces. 3) Give oral radiolabeled B12 + intrinsic factor. If urine B12 does not correct it means there is malabsorption. If urine B12 does correct (>10% B12 in urine) it means that he has pernicious anemia.
Among many other reactions, this particular enzyme is involved in the conversion of norepinephrine to epinephrine. Deficiency in what vitamins would inhibit this process?
B12 and Folate. SAM is a universal methyl donor. Once it donates its methyl group it is converted to homocysteine. Homocysteine is converted to methionine by homocysteine methyltransferase, which requires B12. In order to transfer the methyl group, B12 needs to receive it from TF4. Finally, methionine + ATP regenerates SAM.

A mother gives birth to a newborn child and refuses the vitamin K shot. What lab values are likely to be abnormal in this newborn?
Neonates have sterile intestines and cannot synthesize vitamin K because there are no normal flora. If you don’t have vitamin K, the liver cannot catalyze gamma-carboxylation of Glu residues on clotting factors. The child may have an increased PT and aPTT due to lack of clotting factor activity (II, VII, IX, X). Note that they will also be deficient in protein C and S.
A vegan mother of a small child comes in for the child’s wellness check up. You notice areas of hypo and hyperpigmentation on the child’s skin and his belly is swollen. Labs show anemia. What would you expect to see if you examined the child’s liver grossly?
This child has kwashiorkor from protein deficiency. The liver becomes fatty in these kids because there is decreased apolipoprotein synthesis.
What type of malnutrition results in muscle wasting, loss of subcutaneous fat and variable edema in kids?
Marasmus.
What is the rate determining enzyme in de novo pyrimidine synthesis?
Carbamoyl phosphate synthetase II (CPS II)

What is the rate determining enzyme in de novo purine synthesis? What inhibits this enzyme?)
Glutamine-PRPP amidotransferase. Inhibited by AMP, IMP and GMP (excess purines

What is the rate determining enzyme in the urea cycle? What activates this enzyme?
Carbamoyl phosphate synthetase I (CPS I). Activated by N-acetylglutamate.

A 23 year old African American man presents with fatigue after a bout of pneumonia for which he was given antibiotics. Labs show anemia and peripheral blood smear shows bite cells and Heinz bodies. What is causing this guy’s anemia?
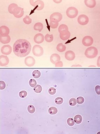
He has X-linked G6PD deficiency, the most common human enzyme deficiency, especially in African due to increased resistance to malaria. Sulfonamides, primaquine, anti-Tb drugs and fava beans can cause oxidative stress that increase the workload of G6PD. Inability to produce enough NADPH in RBCs results in inability to reduce glutathione reductase. This results in inability to reduce glutathione peroxidase and accumulation of free radicals that damages the RBC and causes hemolytic anemia. Heinz bodies are oxidized Hbg precipitates in the cytoplasm and bite cells are a consequence of splenic macrophage removal of Heinz bodies from RBCs.

What amino acids are solely glucogenic?
Met, Val, His

























