Corneal Dystrophies Flashcards
What are the five layers of the cornea?
Corneal Epithelium
Bowman’s membrane
Corneal Stroma
Descements Membrane
Corneal Endothelium
Which layers of the cornea do we mainly have a problem with, if any?
Corneal Epithelium
Corneal Stroma
Corneal Endothelium
What is Epithelial basement mebrane dystrophy?
The epithelium is very weak and doesn’t stick to bowman’s layer underneath.
What are the symptoms associated with a scratch on the cornea if a patient has Epithelial basement membrane dystrophy?
Pain
Watering - epiphora
Photophobia + glare
Waking with a painful eye
How may epithelial basement membrane dystrophy appear under a slit lamp?
Epithelial Micro-cysts
As tiny dots or ‘cogans’ in the corneal epithelium - these are basically patches where the cornea has healed itself following any abrasions.

What is the acute management of a nasty scratch on the cornea?
Anaesthetics - for the pain
Antibiotics - as a preventative measure
Perhaps mydriatics and cyloplegics to rest the eye - when there is a scratch on the cornea the ciliary muscle goes into spasm.
Perhaps a bandage contact lenses
How would we manage recurrent epithelial erosion syndrome (i.e. recurrent damage of the epithelium because it is weak)?
- Debridement - basically take off the current epithelium which is already loose and hope that a new stronger one grows back.(OLD METHOD)
- Anterior stromal puncture - puncture holes in the corneal eptihelium so the bowman’s layer has something to stick onto. (OLD METHOD)
- Excimer laser PTK (phototherapeutic keratectomy)- resurfaces the cornea - it makes the cells of the bownman’s layer rougher so when epithelial cells regrow they have something to stick to. (CURRENTLY USED)
What is Reiss Buckler’s?
Is it unilateral or bilateral?
Is it common or rare?
What is it caused by?
A type of corneal dystrophy that affects the bowman’s membrane - it is caused by an autosomal dominant inheritance.
It is unilateral
It is very rare.
It is caused by abnormal collagen
True or False- Dystrophies are inherited conditions.
True
What are dystrophies?
Abnormal deposition of naturally occuring substances
What condition can be seen in the image below?
In whom is this condition prevalent?
What is this condition the result of?
What does this condition indicate?

Arcus Senilis
Those over the age of 50
This condition is the result of deposits of cholesterol esters and glycerides in the stroma
Indicates Raised Chloesterol
What do you need to know about granular dystrophy?
It is very rare.
Essentially granular deposits.
It is hereditary

What is macular dystrophy and what do you need to know about it?
Diffuse dots all across the surface of the cornea.
it is caused by an excess of naturally occuring material.
It is autosomal recessive.
[Macular is just latin for space]

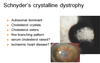
What type of dystrophy is this and what is it caused by?

It is lattice dystrophy. It is an autosomal domiant condition. It is caused by a network of deposits.
It is a rare condition
[Despite having a corneal regraft it still reoccurs].
What condition is this?

Gelatinous Droplet Keratopathy
It is autsomal recessive.
Caused by Amyloid inbalance.
Whta type of dystrophy is this and what is it caused by?

VERY VERY RARE
What does corneal Ectasia mean?
The cornea is buldging aka it is coming forward

What is another name for corneal ectasia?
Keratoconus
How may keratoconus be identified via retinoscopy and slit lamp?
As a scissor reflex in retinoscopy and an oil droplet flashback through ophthalmoscopy.
What is the aetiology of Keratoconus?
udefective collagen cross-linking?
uincreased collagenolysis
- reduced protein synthesis
- defects in RNA translation
- increased corneal compliance
ucorneal hysteresis
-iatrogenic – caused by LASIK laser eye surgery – this is where they take away parts of the cornea – if they take away too much they leave the px at risk of keratoconus – which occurs when the cornea is very thin and so susceptible to distortion.
What are some associations of Keratoconus?
Px with the following conditions are more likely to have keratoconus:
- atopic disease: vernal conjunctivitis, eczema, asthma
- Down’s syndrome (trisomy 21)
- eye rubbing
- aniridia (congenital condition where you are missing the iris)
- Retinitis pigmentosa
- Leber’s congenital amaurosis
- ectopia lentis
- microcornea
- blue sclera – osteogenesis imperfecta………………..
What are signs of keratoconus?

What is the managment of keratoconus?
- Spectacles – however VA limited by irregular astigmatism
- Gas Permeable Contact lenses succeed in 85% of cases
- Collagen Cross-Linking (CCL, CXL, CCXL) – method of strengthening the corneea
- Intacs to ‘reinforce’ mid-peripheral stroma
Corneal grafting
True or False- In corneal grafts the entire cornea is removed and replaced
False - typically only the central 8mm are removed and replaced (the average cornea is 10-11mm wide).



