What are the features of alcohol misuse?
- Harmful drinking
- Alcohol dependency
Alcohol withdrawal
Definition
Pathophysiology
Presentation- timeline of symptoms and signs
Investigations
Differential diagnoses
Management
Alcohol withdrawal
Definition
Physical and psychological changes due to the absence of alcohol
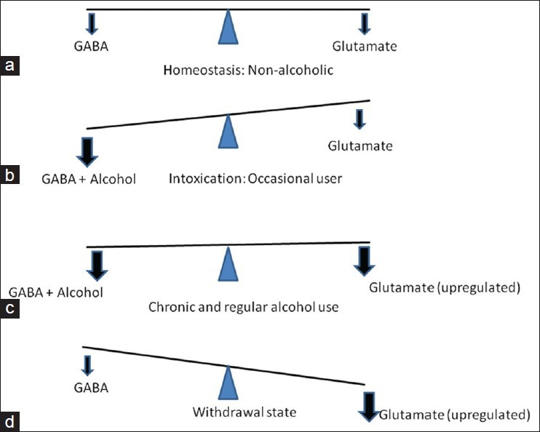
Pathophysiology
Alcohol is a CNS depressant, so GABA increases and glutamate decreases, increasing the body’s sensitivity to glutamate so when alcohol is removed and glutamate therefore increases, has a CNS stimulating effect
Presentation- timeline of symptoms and signs
Day 1
6hrs- mild hangover like
- Nausea and Vomiting/GI upset
- Palpitations
- Sweating and mild tremor
- Anxiety/agitation
12hrs- Mind
- Tactile and visual hallucinations
Day 2
24hrs- Body
- Generalised short tonic clonic seizures
Day 3
36hrs
- Delirium tremens- serious
- Severe tremor
- Confusion/delirium
- Fever
- High HR and BP
Investigations
- History:
CAGE and AUDIT questionnaire
CIWA-Ar scale - severity of withdrawal
- Exam:
Signs of chronic liver failure
- Basic obs
- Bloods:
- FBC
- U and E
- LFT
- INR
- Glucose
Differential diagnoses
- Wernicke’s encephalopathy
- Acute liver failure/decompensated chronic liver failure
- Hypoglycaemia
- Electrolyte abnormalities
Management
- Benzodiazepines- chlordiazepoxide
- Pabrinex [thiamine– affects vit b1 metabolism]
- Glucose [always give after pabrinex- affects vit b1 metabolism]
- Manage alcohol dependence- therapy, drug and alcohol liaison service etc.
Symptoms of Wernicke’s encephalopathy?
CAN
Confusion
Ataxia
Nystagmus
Symptoms of acute liver failure
AABB
Ammonia- encephalopathy
Albumin-oedema.
Bilirubin-jaundice
Blood clotting
Anaphylaxis
Definition
Aetiology
Pathophysiology
Types
Risk factors
Epidemiology
Symptoms and signs
Management
Anaphylaxis
Definition
Life threatening systemic hypersensitivity reaction to an allergen
Aetiology
Allergens=
Food- nuts
Drugs- penicillin, NSAIDS, latex etc
Toxins- bee sting, venom
Pathophysiology
Degranulation of mast cells and basophils
Increases vascular permeability
Causes angioedema, hypotension, urticaria and flushing
Types
Immunologic IgE mediated
Immunologic non IgE mediated
Non immunologic physical- triggered by cold, exercise etc
Non immunologic other- triggered by drugs
Risk factors
FH/PMH of atopy
Epidemiology
Most common in those aged 0-4
Symptoms and signs
Airway- throat swelling and stridor
Breathing
Cicrculation- low BP, high HR
Skin and mucosal changes=
Angioedema-swelling of lips and face
Urticaria
Management
- Call for help
- Oxygen
- Lie flat and raise legs
- IM adrenaline 1:1000 0.5mg
- ABC
- IV chlorphenamine and IV hydrocortisone
Follow up:
Allergy/immunology clinic= RAST specific Ig E testing
Epipen
Medic alert bracelet
Allergen avoidance advise
What is the ABCDE approach? Outline it and how you manage problems in
A- Airway
Obstructions, secretions/vomit
Manage= oxygen, airway adjuncts, remove obstructions
B- Breathing
Resp rate, O2 sats
C- Circulation
BP, HR
Manage: IV fluids, blood transfusion
D- Disability
GCS, PEARL, AVPU
E- examination of whole body
Poisoning/overdose
Definition
Epidemiology
Symptoms and signs
Investigations
Poisoning/overdose
Definition
Adminstration of excess pharmaceutical agent/poison
Epidemiology
Below 10- accidental poisoning
Above 10- deliberate poisoning usually alcohol associated
Symptoms and signs
Nausea and vomiting
Investigations
- ABCDE
- Basic obs
- ECG
- FBC, U and E, LFT, INR, glucose
- ABG
- Paracetamol and salicylate levels
Management
- TOXBASE database- info
- National Poisons Information Service
- Consider activated charcoal if less than 4hr
- Consider gastric lavage -rare
Aspirin overdose
Definition
Presentation- Symptoms and signs + late presentation
Investigation findings
Management
Aspirin overdose
Definition
OD= 150mg/kg, Severe OD=500mg/kg
[One tablet is 300mg]
Presentation- Symptoms and signs
- Lungs- hyperpnea [r-asp-rin] [stimulates resp centre in medulla]
- GI-nausea and vomiting
- Ears- tinnitus, deafness, dizziness [aspi-ringing]
- Systemic- sweating, hypothermia- [per-spirin-g]
Late presentation
- Low BP and heart block
- Low GCS and seizures
- Pulmonary oedema
Investigation findings
ABG
= initially respiratory alkalosis [due to hyperpnea]
= then high anion gap metabolic acidosis [uncouples ox phos, high glucose metabolism, no ATP= increased fatty acid metabolism + ketones + increased lactic acid]
+ usual Ix- see poisoning/overdose flashcard
Management
IV sodium bicarbonate- urine alkalinisation
Dialysis
Paracetamol overdose
Definition
Pathophysiology
Presentation- Symptoms and signs
Management
Paracetamol overdose
Definition
OD= 150mg/kg, Severe/fatal OD=12g
[One tablet is 500mg]
Pathophysiology
Paracetamol is metabolised by CYP450 enzymes in liver to NAPQI
NAPQI is toxic, so conjugated with glutathione and excreted
XS paracetamol= XS NAPQI- glutathione saturated, toxic NAPQI accumulates in liver = hepatocyte death and necrosis
Presentation - Symptoms and Signs
Often asymptomatic
6hr - mild nausea and vomiting, lethargy
24-72hr- RUQ pain, hepatomegaly, vomiting
>72hr- Acute liver failure
Management
IV N-Acetyl cysteine
Liver transplant
Opiate overdose
Presentation
Management
Opiate overdose
Presentation- CNS depression
Pin point pupils [Opiate_]_
Respiratory depression
Bradycardia
Hypotension
Severe/Late: Low GCS/coma
Management
IV naloxone
Catheter
What are the uses/Indications?
Types
Problems
Uses
Treat urinary retention
Monitor urine output
Types
- Foley catheter
- 3-way catheter
- Indications: recurrent clots/haematuria
- Extra lumen for irrigation
3.Suprapubic catheter
•Indications: long-term use, urethral damage (trauma, surgery, stricture)
Problems
UTI
Only treat if symptomatic: 1st step: replace catheter. 2nd step: antibiotics
Catheter blockage
Can be due to biofilm formation (infection with Proteus mirabilis commonly)
1st step: bladder wash out 2nd step: replace catheter
ABG
Indications
Work out blood oxygen levels immediately
Work out if resp or metabolic acidosis/alkalosis
Ad: immediate, blood results take a while to come back
Process:
- Allen test:
- Apply pressure over radial and ulnar arteries with hand elevated for 30 seconds until blanching of the palm
- Release the ulnar artery – colour should return <8 seconds, indicates sufficient collateral circulation
- Clean site (radial artery), apply local anaesthetic if possible, hold needle like a pen at 45 degrees and fill syringe, maintain pressure with gauze for 2 minutes afterwards
•
Indications:
- Accurate measurement of PaO2 required
- Otherwise can use VBG (venous blood gas) for same results
•
Provides:
pH. PaO2, PaCO2, HCO3 and base excess
Electrolytes: Na, K, Ca, Cl
Glucose, lactate
Useful in emergency setting as blood results can take up to 2 hours
Epidural
Definition
Layers crossed
Indications
Indwelling tube in space outside dural membrane between L3/4
Indwelling catheter put in extradural space, usually put in L3/L4
Layers crossed: skin, subcutaneous fat, muscle, supraspinous ligament, interspinous ligament, ligamentum flavum
Indications: lower extremity surgery (sensory and nerve block), particularly obstetrics
Blood transfusion
Process
Products
Early complications
Late complications
Process:
- Group and save (G&S) only valid for 72 hours, identifies blood type and presence of antibodies
- X-match: tests patient blood with donor blood to check compatibility
Products:
1.Packed red cells:
- Indicated if Hb <70g/l or >30% loss of blood volume
- 1 unit increases Hb by 10-15g/l
2.Platelets
•If platelets <20*109/L
3.FFP
•To correct clotting defects e.g DIC
Early complications (<24 hours):
- Anaphylaxis
- Acute haemolytic reaction
- Bacterial infection
- Febrile non-haemolytic reaction
- Transfusion associated circulatory overload (TACO) or transfusion associated lung injury (TRALI)
Late complications (>24 hours):
- Delayed haemolytic reaction
- Infection
- Transfusion associated graft vs host disease
- Iron overload
SBA
A 65 year old man with a history of self-harm presents to A&E with severe nausea and vomiting. He tells you that he took ‘some tablets’ but he didn’t bother to look at what they were. He suffers from stable angina but his PMHx is otherwise unremarkable. His observations are as follows:
HR 110
BP: 110/85
RR: 30
O2 sats: 100%
Temp: 39.0
What is the most likely diagnosis?
A: SSRI toxicity
B: Paracetamol overdose
C: Myocardial infarction
D: Aspirin overdose
E: Panic attack
D Aspirin overdose?
A 21 year old woman of average build is brought to A&E by her mother after she ingested 2 packets of paracetamol ~6 hours ago. She says she feels fine at the moment and wishes to be sent home.
What is the next best step in the management of this patient?
A: Send her home with a referral to the Community Mental Health Team
B: Admit her to the local Mental Health Unit
C: Admit her to the renal ward for immediate dialysis
D: Admit her and prescribe activated charcoal
E: Admit her and start IV N-acetyl cysteine
E: Admit her and start IV N-acetyl cysteine
An 18 year old girl is brought to A&E with difficulty in breathing. On examination, you note swelling of the lips and tongue and an erythematous rash over her face and trunk. Her observations are as follows:
HR 160
BP: 70/50
RR: 40
O2 sats: 92%
Temp: 37.2
Next best step in management?
[clue below]
A: IV adrenaline 0.5mg
B: IM adrenaline 0.5mg
C: IV adrenaline 0.25mg
D: IM adrenaline 0.25mg
E: Start high-flow oxygen
B: IM adrenaline 0.5mg
A 35 year old man presents to A&E in respiratory depression with needle track marks on his arms. He has pinpoint pupils on examination. His observations are as follows:
HR 40
BP: 60/30
RR: 8
O2 sats: 90%
Temp: 37.2
What is the next best step in management of this patient?
A: IV naltrexone
B: IV naloxone
C: IV saline 0.9% 1L bolus
D: IV flumazenil
E: IV atropine
B IV naloxone
A 62yr old gentleman is brought to A&E by his wife who suspects that her husband has been drinking. It is clear that the gentleman is disoriented, and he has a particularly unsteady gate. On examination, you note: spider naevi, gynaecomastia, nystagmus on lateral gaze and mild peripheral neuropathy. His blood results are as follows:
FBC:
Hb: 12.5g/dL (13.5-17.5g/dL)
MCV: 105fL (80-96)
HCT: 0.35 (0.4-0.5)
Platelet: 200*10^9/L (150-400*10^9)
WBC: 8,000/mL (4,000-10,000)
U&E: Normal
CRP: Normal
INR: 0.7 (<1.1)
What is the most likely diagnosis?
A.Hepatic Encephalopathy
B.Wernicke’s Encephalopathy
C.Encephalitis
D.Normal Pressure Hydrocepahlus
E.Delirium tremens
A Wernicke’s encephalopathy?
-
Headache28
-
Upper GI39
-
Bones and Calcium Metabolism38
-
Sodium and LFTs23
-
Acute Neuro36
-
Acute medicine19
-
cardiac conditions: chest pain32
-
cancer and bleeding conditions30
-
chronic shortness of breath16
-
Neurodegenerative disease22
-
Vascular diseases25
-
cranial and ophtalmology33
-
Cardiac causes of SOB27
-
Acute respiratory problems14
-
ENDO20
-
infections and antibioticcs28
-
Urology30
-
Vasculitis and Autoimmune disease43
-
from oxford handbook61
-
Lower GI21
-
Derm35
-
breast18
-
anaemia55
-
acute GI30
-
Valvular disease and HTN42
-
Biliary and liver49
-
Arthritis21
-
Infectious diseases31
-
renal83
-
ECG and CXR55
-
Adrenal30
-
Cough27
-
ABGs30
-
Infectious disease 232
-
Questions for cardio42
-
Extra questions155
