5 - MZH - Homeostasis 6 - Excretion and the Kidneys Flashcards
Define:
Excretion
Osmoregulation
Excretion = The emilination of metabolic waste including
Osmoregulation = The balancing and control of of the water potential in the blood
What is the approximate human blood pH?
pH = 7.4
Fill in the table and give examples of each


Summarise 2 main functions of the kidneys
- Act as excretory organs - Removes nitrogenous and other waste from the body
- Important role in homeostasis - Helps to regulate blood pH, water and Na+ conc in the blood and tissue fluids
What waste fluid do mammalian kidneys produce?
Urine which is more concentrated than the body fluids
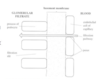
Lable the diagram


Lable the diagram of the kidney


Name the 2 different types of nephron
-
Cortical nephrons
- Allow only minor water conservation
- Used in normal water availabilty conditions
-
Juxtamedullary nephrons
- Allow water conservation
- More present in animals that need to conserve more water

Name a type of animal that has more of:
- Cortical nephrons
- Juxtamedullary nephrons
WHY?
- Beaver, otta or platypus - No problem with having access to frsh water.
- Camel - Need to conserve max volume of water
What is the name of the functional unit of the kidney?
Nephron
What does it mean?
Afferent and efferent?
Afferent = A blood vessle supplying blood to a structure
Efferent = A blood vessle carrying blood away from a structure
Lable the diagram of the nephron


Briefly describe how blood travels through the kidneys

- Blood enters each kidney via the left/right renal arteries that branch into arterioles.
- Each arteriole divides into a knot of capillaries called the glomerulus. Each glomerulus is found in the cup of each renal capsule/Bowman’s capsule.
- Blood leaved the glomerulus into the efferent vessel which is an arteriole and divides into the second capillary network which surrounds the PCT, DCT and loop of Henle.
- Blood from this capillary network then drains into venules and finally into the renal vein.
- Kidney filtrate is formed in the renal capsule and flows down the nephron via the PCT, loop of Henle and DCT and enters the collecting duct which emties it into the pelvis.
What are the 3 main processes that occur in the kidneys?
-
Ultrafiltration - From glomerulus to Renal/Bowman’s capsule
- Water and soluble substances pass from the blood into the lumen of the renal capsule. This becomes the filtrate which is now in the nephron, it contains excretory products & useful products.
-
Selective reabsorption - Mainly PCT
- Useful substances e.g. glucose are reabsorbed into the blood.
-
Concentration - Loop of Henle and collecting duct
- Loop of Henle creates the right conditions in the medulla allowing a conc gradient to occur.
What makes up the renal corpuscle?
Bowman’s capsule and the glomerulus
What is ultrafiltration?
Ultrafiltration = High pressure filtration of blood between the glomerular capillaries and the renal/bowman’s capsule and results in the formation of glomerular filtrate which will pass down the length of the nephron
How is a high pressure created during ultrafiltration? (3)
- High blood pressure in renal arteries
- Narrow glomerular capillaries
- Wider afferent arteriole and narrow efferent arteriole

What are podocytes?
Podocytes = Specialised cells found in the epithelium of the Bowman’s capsule. They’re wrapped around the capillaries

Ultrafiltration:
What step is this in the process?
Describe the process
What does the filtrate contain? (7)
What remains in the blood and why? (2)
- It’s the 1st step
- The high pressure in the glomerulus results in a high hydrostatic pressure which forces water and solutes from the blood plasma into the renal capsule forming filtrate.
- Filtrate consists of:
- Dissolved ions
- Glucose
- Vitamins
- Amino acids
- Fatty acids
- Glycerol
- Urea
- Blood cells and plasma proteins are too large to be filters so they remain in the blood.

What layers are there to the filtration barrier in ultrafiltration? (3)
There’s 3 layers:
-
Endothelium of capillary
- Pores allow fluid passage but hinder blood cells
-
Basement membrane is the actual filter
- Made of a mesh of collagen fibres
- Blocks molecules > Mr 69,000
- Large proteins blocked due to size & repelled by negative charges on callagen
-
Epithelium of renal capsule
- Contains podocytes
- Filtration slits allow passage of fluid into filtrate
What step occurs right after ultrafiltration?
What is it’s purpose?
Where does this occur in the kidney?
- Selective reabsorbtion occurs after ultrafiltration.
- It retunrs the useful substances from the filtrate back into the blood.
- It occurs mainly in hte PCT (proximal convoluted tubule)
Selective reabsorbtion:
Where does it occur? What particular about the structure of this location and how is it adapted to carry out this process? (6)
Mainly in the PCT. The PCT is composed of a single layer of epithelial cells.
- Large SA - Relatively long PCT. Microvilli on tubule cells also increase SA.
- Convolutions - Slows down flow rate, more time for reabsorbtion.
- Maintain conc gradient - Many blood capillaries close to the tubule.
- Short distance between filtrate and blood.
- Many mitochondria - Produce ATP for active transport.
- Specific carrier/ transport proteins in the cell membranes.
Describe how selective reabsorbtion happens
- Na+/K+ pump in the proximal tubule cell membrane uses ATP made by the mitochondria. As ATP is being used K+ ions are pumped into the cell and Na+ ions out to increase the K+ ions conc and reduce the Na+ ions conc inside the cell.
- Na+ ions actively transported into the basal channels but they can only be transported if they are paired up with a glucose molecule. Simultaneously glucose can enter the cell via a symport protein.
- Glucose leaves the cell by facilitated diffusion

Cotransporter proteins and their role in selective reabsorbtion?
In this case it’s when Na+ ions are holding onto something else e.g. glucose. Unless it’s paired with a glucose moelcule it can not be transported by that cotransporter protein.
Different cotransporters bring about the reabsorbtion of all the other substances that need to be removed from the filtrate as well.
What happens to these substances in the selective reabsorbtion stage?
- Glucose
- Water
- Urea
- Small proteins
- Glucose - Filtrate → Epithelium → Basal Channels → Blood
- Water - Continuous solute removal to blood maintains a water potential gradient for reabsorbtion of water into blood by osmosis
- Urea - Up to 50% is unfortunately reabsorbed by diffusion
- Small proteins - Uptake by pinocytosis & lysosomes liberates amino acids. Amino acids used by cell or enter the same pathway as glucose: Filtrate → Epithelium → Basal Channels → Blood
At the end of selective reabsorbed what is the solute potential compared between the blood and filtrate?
Filtrate in PCT becomes isotonic compared to blood
What process occurs after selective reabsorbtion? Where does it occur?
Water reabsorbtion
It occurs in the loop of henle
In selective reabsorbtion is glucose actively transported?
No - it is transported passively. It relies on the active transport of sodium ions though
What does hypertonic urine mean?
Very concentrated urine - it means that it has a high conc of solutes. Allows water to be conserved
What is the function of the loop of Henle?
To produce a conc gradient of NaCl across the medulla which creates the necessary water potential gradient to allow water to leave the filtrate by osmosis
What are the different regions of the loop of Henle and how do they compare with permeabilities to water and sodium ions?
What is common amongst the whole loop of Henle?
-
Descending limb
- Highly permeable to water
- Slightly permeable to sodium ions
-
Ascending limb
- Impermeable to water
- Narrow region is highly permeable to sodium ions and it’s wide region actively pumps sodium ions from the filtrate into the surrounding tissue fluid
Whole loop is relatively impermeable to urea so most of the urea molecules remain in the filtrate
Fill in the blanks for the loop of Henle diagram


Describe what would happen in the loop of Henle if the fluid did not flow.
Use the example with tje stationary fluid starting a conc of 300 units

Explain how the loop of Henle allows the production of concentrated urine

Describe what happens in the loop of Henle if the fluid did not flow
-
Ascending limb:
- Na+ & Cl- ions are actively transported out of the asending limb into the tissue fluid.
- Water cannot follow as wall of ascending limb is impermeable to water.
- Surrounding tissue fluid increase conc of Na+ & Cl- and makes it more conc by 200 units (tissue fluid is 400 units now).
-
Descending limb:
- Water diffuses out & into tissue fluid until equilibrium is achieved.
This scenario can only produce a concentration difference of 200 units at any given point due to leakage of ions back into ascending limb

Describe what happens in reality in the loop of Henle i.e. when the fluid is flowing.
Why does the NaCl and water not accumulate in the tissue fluid?
-
Ascending limb:
- As fluid rises, active removal of NaCl causes it to become less & less concentrated.
- This increases thr NaCl concentration in the surrounding tissue fluid.
-
Descending limb:
- As fluid descends, water can continuously exit by osmosis to the more concentrated tissue fluid.
The water & NaCl don’t accumulate in tissue fluid forever as they’re removed by the capillary network - a dynamic equilibrium is reached. A total change of concentration of 900 units can be achieved - but only the 200 unit difference at any given point.

Why the arrangement of the loop of Henle regarded as a counter-current multiplier?
- Counter current - The fluid flows in the 2 limbs in opposite directions
- Multipler - The total conc change is increased as a factor of the increase in the length of the loop of Henle
Give points on the role of the loop of Henle (7)
- Sets up a conc gradient of NaCl across the medulla
- This sets up a water potential gradient across the medulla
- The deeper into the medulla the higher the NaCl conc and the more negative the water potential
- This means the water potential of fluid in the colecting ducts is always less negative than the water potential in the tissue fluid of the medulla
- As a result water can be removed by osmosis, down a water potential gradient, all the way down the collecting duct
- The longer the loop of Henle the more water can be removed from the colelcting ducts and the more conc the urine becomes
- Long loops of Henle are characteristic of dessert animals
Structure and role of the distal convoluted tuble (DCT) and structure
-
Structure:
- Cells that make up the wall of the DCT have microvilli on their plasma membranes in contact with filtrate and man mitochondria that allow them to rapidly absorb substances from the filtrate by diffusion & active transport.
-
Role:
- Final judgements to the water and salts that need to be reabsorbed.
- Maintain blood pH by selectively absorbing ions . Maintain blood pH at 7.4.
What heppens when the blood pH falls below the norm of 7.4? Why does it fall?
- Blood pH falls - Metabolism tends to generate acids which lower blood pH.
- If blood pH falls below norm
- Actively secrete H+ into nephron fluid which is the glomerular filtrate
- Lowers blood pH and the H+ ions leave the body via the glomerular filtrate
Give 3 causes that can result in a more negative water potential?
- Too little water being consumed
- Water loss due to sweating
- Large amounts of salt being ingested
Describe the sequence of occur in response to a decrease in water potential (7)

Where is ADH made and stored?
What stimulates the secretion of ADH?
What are the effectors of ADH?
- ADH is produced in the cell body of neurosecretory cells in the hypothalamus
- It travels down their axons to be stored at their axon terminals in the posterior pituitary
- Secretion of ADH is stimulated by osmoreceptors
- ADH causes epithelial cells of DCT & CD to add aquaporins to their plasma membrane. It also stimulated the thirst center of the brain to alert the person they need a drink!
Describe the sequence of events that occur as a result of a higher/less negative water potential being detected?

List 5 causes of renal failure
- Infection - Either to kidneys or other parts of the body
- Poisons
- Damage to the circulatory system resulting in an inadequate flow of blood to the kidneys
- Hypertension (raised blood pressure)
- Diabetes mellitus
How does infection cause renal failure?
- During infections, the structure of the podocytes and the tubules may be damaged or destroyed.
- Means that ultrafiltration can’t happen.
- Decrease function of the kidneys and can’t get rid of waste products.
How does diabetes mellitus cause renal failure?
Glucose in the bloodstream can not be reabsorbed so they leave the body as a part of urine
How does hypertension cause renal failure?
-
Raised blood pressure
- Damage the structure of epithelial cells and basement membrane of the bowman’s capsule.
-
Know it’s happening as damaged podocytes and basement membrane can’t act as filters:
- Protein in urine - Larger molecules like proteins will be filtered out.
- Blood in urine - RBC will be filtered out into urine
What is dialysis?
Dialysis is using a partially permeable membrane to filter the blood
Symptoms of renal failure (3)
- Oedema (swelling of tissues) and rise in blood pressure due to retention of salt and water in the tissues.
- Drop in blood pH due to retention of urea and other excretory products
What are the 2 different forms of dialysis that is available right now?
Haemodialysis
Peritoneal dialysis
Treatments available for renal failure
- Dialysis
- Haemodialysis
- Peritoneal dialysis
- Kidney transplant
In the future we may be able to use stem cells
How does Haemodialysis work?
What is special about the dialysis fluid?
Blood from the patient is taken from a vein and passes through a dialyser/ artificial kidney which contains dialysis fluid.
- Pores in the membrane allow free passage of small molecules e.g. H2O, glucose, amino acids, urea and Na+ and Cl- ions.
- Pores are too small to allow the passage of plasma proteins and blood cells.
- Higher pressure of the blood speeds up the removal of urea from the blood much like in ultrafiltration in the renal capsules.
- These molecules and ions will only leave the blood down their conc gradients.
NOTE: Composition of the dialysis fluid is carefully balanced so that only urea, excess water and excess ions leave the blood and glucose & amino acids are retained

What do these parts of the dialyser for haemodyalysis do?
- Heparin pump
- Dialyser
- Air trap/air detector
Heparin pump = Acts as a blood thinner to prevent blood clotting
Dialyser = Where the actual dialysis takes place. Waste products are removed in thr form of urea
Air trap/air detector = Gets rid of all air bubbles in the blood before the blood is returned into the patient’s body

Why might a fistula or graft be required for haemodialysis?

- Easy access to the artery and vein required for dialysis
- Reason:
- Vein will then have walls that can withstand the pressure of being repeatidty poked at with a needle

What is the dialysis fluid from haemodialysis composed of?
What is the benefit of the counter current flow?
- Composition of dialysis fluid:
- Normal plasma levels of glucose - ensures no net movement
- Normal levels of plasma fluid mineral ions so excess mineral ions in blood will diffuse down a conc gradient into the dialysis fluid
- Counter current flow ensures a conc gradient is constantly being maintained

Problems with dialysis (4)
- Each treatment takes several hours
- Usually done in a hospital
- Several treatments may be needed each week
- The person has to eat a restricted diet, low in salt and protein
How does peritoneal dialysis work and differ from the traditional haemodialysis?
Done inside the body, and uses the body’s own abdominal membrane - the peritoneum as the dialysis membrane.
- Permanent tube is implanted in the abdomen.
- Dialysis fluid passes through the tube and fills the space between the abdominal wall and periteoneum.
- After several hours the used dialysis fluid is drained from the abdomen.
Can be carried out at home or at work - much less of an impact on lifestyle

Problems arising from kidney transplatation as a form of treatment of renal failure (5)
What are xenotransplants? + 2 problems associated with it
- Shortage of donors
- Tissue type of the donor must be a close match to the recipient
- Immunosuppressant drugs are needed for the rest of the recipient’s life
- Recipients are at greater risk of infections
- Global trade in kidneys - exploiting poor people AKA black market
Possible use of xenotransplants i.e. from animals (e.g. pigs) but:
- Increases risk of infection diseases jumping species
- Raises ethical issues.
Name 5 things that can be tested using urine
- Glucose in the diagnosis of diabetes
- Alcohol to determine blood alcohol levels
- Many recreational drugs
- Human chorionic gonadotrophin (hCG) in pregnancy testing
- Anabolic steroids to detect improper use in sport
How is a positive test using urine for the presence of glucose an indication that the person is diabetic?

In a non diabetic no glucose will be present in the urine
What is the name of the test for pregnancy?
Why do 2 blue lines reliably indicates a pregnancy?

Human chorionic gonadotrophin (hCG) test
- Urine carries along test until it reaches a window.
- Here there’s immobilised monoclonal antibodies arranged in a line or a pattern such as a + sign that only bind to the hCG/antibody complex.
- If the woman is pregnant, a coloured line or pattern appears in the frst window.
- Urine continues up through the test to a second window.
- Here there is usually a line of immobilised monoclonal antibodies, regardless of whether they’re bound to hCG or not. This coloured line forms regardless of whether the woman is pregnant or not
- It indicates that the test is working

How can urine be used to test for anabolic steroids?
Use gas chromatography and mass spectrometry.
- Urine sample is vaporised with a known solvent and passed along a tube.
- Lining of the tube absorbs the gases and is analysed to give a chromatogram that can be read to show the presence of drugs.

