29. Kidneys and Urinary System Flashcards
(21 cards)
Where is the renal angle?
Are the L and R kidneys at the same level?
Are the kidneys in contact with the pritoneal space?
Junction of 12th rib and lateral border of erector spinae (pic) (examine for tenderness here)
No - R = slightly lower so covered by just 12th rib and on L side abit higher (covered by 11th and 12th ribs)
No - in own capsule. They are found in retroperitoneal space in posterior abdominal wall, surrounded by own layer of fascia.

What are A and B in this ultrasound slide (positve FAST scan)?

A: fluid in potential peritoneal space = makes it a real space. Could be blood or ascites.
B: R kidney
What muscles and nerves are in contact with the kidneys?
What is Gerota’s fascia?
Diaphragm, psoas major, qudratus lumborum. T12 subcostal nerve. L1 divides to iliohypogastric (to hypogastrium) and ilioinguinal.
Layer of CT (fascia) encapsulating the kidneys and the adrenal glands, merges with adventita of great vessels.

Label A-D of this kidney transverse section.

A: pararenal fat
B: renal capsule
C: perirenal fat (surrounds kidney)
D: renal fascia (gerota’s facia)
E: abdominal muscles
F: quadratus laborum
G: psoas
Label A - C on this para-sagittal section (RHS) of the kidney.

A: hepatorenal recess
B: fascia and fat (kidney in own layer of deep fascia)
C: peritoneum
What can you see here?
What could have caused this?
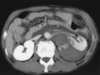
Trauma to back e.g. kick
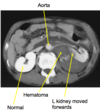
A 28yo male was kicked in the back. He experienced severe pain in R flank, had no broken bones, and haematuria. On CT: hematoma on R next to kidney, which is higher than it should be.
Why flank pain?
Why is the blood confined to L side?
Why haematuria?
Fibres from sympathetic trunk from T10-T12. Visceral sensory from kidney back to sympathetic trunk at this level = get referred pain across T10 - 12 dermatomes = flank pain.
Because there are 2 discrete compartments
Gone into internal kidney architecture
Label A-F of the kidney
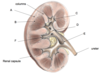
A: cortex
B: medullary pyramid
C: minor calyx
D: major calyx
E: pelvis
F: renal papilla
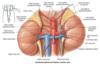
Describe the internal vasculature of the kidneys.
Where do the renal arteris and veins arise?
Where does the lymph drain to?
What is the (autonomic) nervous supply of the kidney?
Arteries: renal artery divides at hilum to 5 segmental arteries that supply discrete renal segments -> lobar arteries (1/pyramid).
Venous drainage via a similar path.
Renal arteries: L1/2 (R post to IVC), renal veins: L2 (anterior to aorta, L longer than R due to R lateral position IVC. R receives L suprarenal an gonadal vains)
Lateral aortic lymph nodes
Via renal plexus: sympathetic, visceral afferent, and from thoracic and lumbar splanchnics

22yo male, L sided back pain, weight loss, painless lump in L testicle developed over last 12 months, no fever/dysuria, palpable mass in L flank which moves inferiorly on inspiration (thus visceral - not with post abdo wall). Tender below 12th rib on same side (renal angle).
What is the likely diagnosis and why?
Testicular tumour. Testes develop next to kidneys and the descend from the posterior abdominal wall = same blood supply, venous and lymph drainage around posterior wall -> lymph node around kidneys = common site for metastasis.
18yo male, L painful testes, look like a ‘bag of worms’.
What is the likely diagnosis?
Would this scenario be equally as likely on the RHS?
Why might a renal ultrasound be requested?
Varicocele - vaicose veins in testes. Abnormal enlargement of the pampiniform venous plexus in the scrotum.
No, almost always L b/c testicular vein drains up to L renal vein, which tends to be flat over aorta and has superior mesenteric over it, so pressure in L renal vein higer than IVC. Thus blood doesn’t drain as easily.
If tumour grows from kidney into renal vein -> cause varicocele b/c testicular vein won’t drain properly
Label A-E

A: aorta
B: duodenum
C: R renal vein
D: pancreas
E: spleen
What are ureters? Describe their course.
Describe the trilayers of the ureter walls.
How do ureters propel urine to the bladder?
Retroperitoneal, muscular tubes. Pass over pelvic brim (division between basin or pelvis and wider pelvis) at bifucation of common iliac arteries, run on lateral walls of pelvis, oposite ischial spine, curve anteromedially. Oblique entrance to bladder - one way flap valve.
Transition epithelial mucosa (same as bladder), smooth muscle muscularis, fibrous CT adventitia.
Peristalsis - response to SM stretch

Where are the 3 points of narrowing in the ureter?
Why are they clinically significant?
Why might pain from a calculi in the ureter radiate to the groin?
1) Renal pelvis -> ureter (PUJ - pelvi-ureteric junction)
2) Ureter changes direction, goes into true pelvis over bifurcation
3) 1-way flap valve into bladder
Concentrate on these 3 areas when looking for calculus
Visceral afferents enter at spinal levels T11 - L1/2. Loin pain referred along the ilioinguinal and iliohypogastric nerves (L1). As stone descends, patient may start to feel pain descend over groin and strotum/labium majora (“loin to groin”). This is because of the changing nerve segments and the pain is now referred through the ilioinguinal nerve (L1,2).
Why might a woman have right flank pain following total hysterectomy?
Where is the bladder located?
What happens to it as urine accumulates?
Ureter can be damaged during it b/c close to uterine artery which is normally clamped for the operation.
Retroperitoneally on pelvic floor posterior to pubic symphysis. It’s connected anteriorly to the umbilicus (median umbilical ligament - urachus).
Bladder exapands without significant rise in internal pressure (because roof domes up but trigone stays the same)

What are the three layers of the bladder wall?
What is the trigone?
Why is it clinically significant?
Transitional epithelial mucosa, thick muscular layer (dentrusor muscle), fibrous adventita.
Triangluar area outlined by opening for ureters (ureteric orifices) and the urethra (internal urethral orifice). “Smooth” texture - rest of bladder ‘rugged’
Infections tend to persist in this region

What is the urethra?
Describe the 3 types of sphincters found along it.
Muscular tube that drains urine from the body and conveys it out of the body. Starts at urethral orifice. Sphincters keep it closed when urine is not being passed.
1) Internal urethral sphincter (males) - involuntary, at bladder-urethra junction (prevents retrograde ejaculation)
2) External urethral sphincter - voluntary, surrounds urethra as it passes through urogenital diaphragm
3) Levator ani muscle - voluntary urethral sphincter (pelvic floor!)
Label A-E

A: levator ani (pelvic floor)
B: detrusor muscle
C: trigone
D: internal urethral orifice
E: external urinary sphincter (voluntary)
The male urethra has a double curvature and is longer than the female. What 4 sections is it divided into as it passes through pelvic structures?
1) Intramural (pre-prostatic): through area where internal urinary sphincter is
2) Prostatic: contains ejaculatory ducts
3) Intermediate (membranous): penetrates perineal membrane, surrounded by external urethral sphincter
4) Spongy
Label A-F

A: ureteric orifice
B: trigone
C: internal urethral orifice
D: prostate
E: voluntary external sphincter
F: (from top to bottom) prostatic, membranous and spongy urethra
What is benign prostatic hyperplasia?
What is micturition? How does it happen?
Describe the voiding reflexes?
Enlarged prostate gland, may squeeze/partly block urethra. Affects elderly men most (pic)
Emptying bladder. Distension of bladder walls initiates spinal and sympathetic reflexes that stimulate contraction of external urethral sphincter and inhibit the detrusor muscle and internal sphincter (temporarily)
Parasympathetic - efferent. Stimulate the detrusor muscle to contract, inhibit the internal and external sphincters.

