(16.1) Pulmonary Pathology II (Singh) Flashcards
What is a restrictive lung disease?
aka interstitial lung dz, characterized by volume restriction (stiff lungs) = cannot fill the lung
FEV1/FVC ratio is normal or increased (both are reduced BUT the ratio is not necessarily reduced)
(FEV=force expiratory volume, FVC=forced vital capacity)
What is the pathogenesis of Idipoathic pulmonary fibrosis?
IPF damages pulmonary tissue with waves of inflammatory injury leading to fibrosis
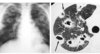
What would a CXR look like for a idiopathic pulmonary fibrosis pt?
Basilar infiltrates
“Honeycomb lung”

What do the lungs sound like on auscultation for idiopathic pulmonary fibrosis?
Crackles on exam
“Velcro-like”
What are the contributing factors to idiopathic pulmonary fibrosis?
Enviornmental factors (SMOKING)
Genetic factors
Increasing age
What is unique about the histology of idiopathic pulmonary fibrosis?
Very different patterns due to the “wave like” nature of the disease
Some patches are normal, some have inflammation, others have fibroblast foci and some have peripheral honeycombing

What do pathologists call idiopathic pulmonary fibrosis when found on pulmonary biopsy?
Usual Interstitial Pneumonia (UIP)

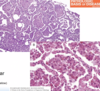
What do these images represent?

Honeycomb fibrosis

What is the prognosis for patients with idiopathic pulmonary fibrosis?
NOT GOOD
Most patients die from respiratory disease 3-5 years after diagnosis (either from respiratory failure or cor pulmonale)
Only truly effective treatment = lung transplant
What are some experimental medications being used to treat idiopathic pulmonary fibrosis?
These meds are used to arrest fibrosis
- Tyrosine kinase inhibitors*
- TGF-Beta inhibitors*
What is non-specific interstitial pneumonia (NSIP)?
VERY SIMILAR TO UIP
Idiopathic
Has UNIQUE HISTOLOGY = uniform infiltrates and fibrosis
Has better prognosis than UIP
What is this lung disorder?

Non-specific interstitial pneumonia (NSIP)

What does cryptogenic organizing pneumonia (COP) looks like histologically?
Looks like cotton candy
The “cotton candy” is fibroblast foci (Masson bodies) = organizing plugs of connective tissue

Cryptogenic organizing pneumonia (COP)
Prognosis?

Very good!
Patient tend to have full recovery with oral steroids since the fibroblast foci are early fibrosis that are so poorly established
How do you diagnose cryptogenic organizing pneumonia (COP)?
Diagnosis of exclusion
-Not an infection, drug- or toxin-induced, or related to connective tissue disorders
What is an important consideration for patients presenting with possible pulmonary fibrosis (IFP, NSIP, COP)?
This may be secondary to their autoimmune/connective tissue disease such as RA, Scleroderma or SLE
important to treat the underlying disorder that is causing the fibrosis
What is this?

Granulomatous inflammation

What is sarcoidosis?
Systemic disease manifesting non-caseating (non-necrotizing) granulomata
What is the clinical presentation of sarcoidosis?
Incidental abnormal radiograph
or
Dyspnea
What are some of the hallmark granuloma inclusions of sarcoidosis?
Granuloma inclusions:
Asteroid body (A)
Schaumann bodies (B-D)

What is the demographic of sarcoidosis?
<40 years of age
African americans
Commonly involve LUNGS
Elevated ACE levels
Sarcoidosis
Do the stages occur in order?
What are the common causes of death in sarcoidosis?
No
from pulmonary, cardiac or neurologic involvement
What is this?

Hypersensitivity Pneumonitis
Granuloma isn’t well defined becuase it is mixed with inflammatory cells as a reaction to inhaled substance
What is hypersensitivity pneumonitis?
Immune reaction to inhaled organic antigens (bird poop, hay, Mycobacterium avium complex)