Week 10: Renal System for Volume – Pressure Control and Micturition Reflex Flashcards
(30 cards)
What is the effective circulating volume
- The Effective circulating volume (ECV) is the volume of ECF that is present in the arterial system, that has a definite pressure, which perfuses tissues. There are sensors which detect changes to this ECV known as volume receptors. If there are changes, in ECV there will be a change in ECF
Describe the renal regulation of ECF volume if there is decrease perfusion pressure
- If there is a decrease perfusion pressure, there is less stretch of the afferent arteriolar wall. This causes renin release which activates the angiotensin-aldosterone axis
- This aldosterone will then cause the increased reabsorption of sodium
- This increase in ECF sodium will then cause increased serum osmolarity. This will then trigger ADH release which will increase water retention. This will dilute the excess sodium chloride maintaining osmolarity, whilst also increasing ECF volume

what are teh two main secretions by the kidneys which regulate blood pressure
- Regulation sodium secretion
- Regulating water secretion
If the ECV is low, what are the mechanisms which will be initiated (x3)
- In the high-pressure zone of the afferent arteriole in the Juxtaglomerular apparatus, there will be increased release of renin (as a result of renal ischemia)
- This will upregulate the Renin-Angiotensin-Aldosterone System, to increase sodium and water retention
- This will increase ECF volume, which will raise mean arterial blood pressure - The sympathetic nervous system will also be stimulated by high pressure receptors
- This will cause cardiac excitation
- There will also be increased sodium reabsorption in proximal tubule in the PCT (alpha receptors)
- Both of these will raise mean arterial blood pressure - The low-pressure baroreceptors (present in atria, and pulmonary circulation) will stimulate the hypothalamus to increase ADH secretion
- ADH acts to increase water reabsorption in the distal convoluted tubule
- This will raise the mean arterial blood pressure
- All of these mechanisms work to increase the mean arterial blood pressure

If ECV is high, what are the mechanisms which will be initiated?
- In the high-pressure zone of the afferent arteriole in the juxtaglomerular apparatus, there will be reduced release of renin
- This will downregulate the RAAS, causing sodium and water loss
- This will lower ECF volume, which will lower the ECV - The sympathetic nervous system activity will be decreased
- This will cause reduced cardiac activity
- This will increase afferent arteriole dilation (to increase GFR to increase loss of fluid) - The Low-pressure baroreceptors are stimulated when stretched to release of ANP (possibly BNP as well)
- ANP will cause natriuresis (reduce sodium levels)
- Water retention will be less
- All of these mechanisms work to reduce the mean arterial blood pressure

What are the renal mechanisms for if ECF volume gets to large
- If the ECF volume gets bigger, the baroreceptors in both the high and low pressure vascular circuits send signals to the kidneys
1. Decreased activity of the renal sympathetic nerves - Will cause the glomerular filtration rate to increase à decrease sodium reabsorption
2. Increased release of ANP and BNP from the heart and urodilatin by the kidneys - Urodilatin is a natriuretic peptide, which causes natriuresis (sodium loss). It is released from DCT and Collecting Ducts to act on the nephrons causing decreased sodium reabsorption)
- Urodilatin is stimulated by increased volume
- ANP and Urodilatin will cause afferent arteriole dilation (vasodilation) which increases filtration of water and sodium by raising GFR
3. Inhibition of ADH secretion - Reduced water reabsorption
4. Decreased renin secretion and thus decreased production of angiotensin 2
5. Decreased aldosterone secretion (which is caused by reduced angiotensin 2 levels and inhibition by elevated ANP) - This increased excretion of sodium chloride and water
- All of these increase sodium and water excretion, causing reduced ECV

What are the renal mechanisms for if ECF volume gets to small
- If the ECF gets smaller, the volume sensors in both the high and low pressure vascular circuits send signals to the kidneys
- These signals basically reduce the sodium chloride and water excretion
- The specific signals that act on the kidneys include;
1. Increased renal sympathetic activity - This decreases the glomerular filtration rate
- Will increase sodium reabsorption will occur
2. Increased secretion of renin - which causes elevated angiotensin 2 levels which increases secretion of aldosterone by the adrenal cortex
- Angiotensin 2 increases sodium reabsorption
- Aldosterone increases sodium reabsorption
3. Stimulation of ADH secretion by the posterior pituitary - This increased water reabsorption in the Distal Convoluted tubule and collecting duct
4. Decrease ANP and BNP

what is pressure natriuresis and pressure diuresis and when are they used?
- Pressure natriuresis
- Elevated blood pressure can lead directly to increased excretion of sodium, particularly if the body contains excess fluid
- This occurs within the renal system, that is, it doesn’t require external signalling
- This can be overridden by external signalling such as in aerobic exercise when arterial pressure is raised, by sodium excretion is decreased. - Pressure diuresis
- Is when the increased pressure caused increased water excretion
- If you put more volume into the glomerulus, the increased pressure reduces the time for tubular reabsorption

what are some factors that cause renal failure which results in hypertension? (x5)
- Decreased nephron number (due to ischemia or infarction of renal tissue)
- Decreased glomerular capillary filtration coefficient (is the permeability area available)
- Increased distal and collecting tubule reabsorption
- Increased preglomerular resistance
- Increased reabsorption in the PCT and Loop of Henle
All of these increase sodium and water reabsorption

What are teh 4 main signals involved in the control of renal sodium and water excretion

What is the micturition reflex and what does it briefly involve (two broad steps)
- Is the process by which the bladder empties
1. Bladder fills progressively causing tension in bladder wall to increase (bladder is made up of smooth muscle)
2. This tension initiates a nervous reflex (the micturition reflex) which either empties the bladder or causes the conscious desire to urinate - Thus, the micturition reflex is a complex act that involves both autonomic and somatic nerve pathways, and a number of reflexes that can either be facilitated or inhibited by higher centres in the brain
- Basically, it is an autonomic spinal reflex, that is controlled by a higher centre
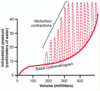
What are the 3 phases of cystometrogram
- Segment 1a
- Apart of the filling phase - Segment 1b
- Apart of the filling phase
- This is the plateau phase, which is facilitated by the inherent properties of the detrusor muscle (smooth muscle)
- This inherent property is better known as the stretch relaxation
- Can be attributed to the law of Laplace - Segment 2
- Apart of the voiding phase

Explaint he stretch relaxation mechanism of the destrusor muscle and what it contributes to cystometrogram
- If you stretch the detrusor muscle, and keep it stretch, the muscle will relax at that point and reduce the tension
- When this muscle relaxes, the length does not decrease, but rather the tension just decreases
- So, as volume increases (like in phase 1b) this causes increased tension initially, however after the stretch relaxation mechanism kicks in, tension decreases
- The flatness segment of 1b is a manifestation of the Law of Laplace (pressure is directly proportional to (2 x tension / radius)
- So, using this rule, if the tension decreases and the radius doesn’t change (that much), there will be little increase in pressure
- In other words, you can fill the bladder without much change in pressure initially
explain the nerve supply to the bladder (somatic, sympathetic and parasympathetic

- Somatic
- Which is through the pudendal nerves (S2, S3, S4) which is under the control of the higher centre
- This controls the external urethral sphincter (skeletal muscle)
- Uses ACh and acts on nicotinic receptors - Sympathetic
- Which is through the hypogastric nerves (L1, L2, L3)
- This controls bladder wall relaxation (Beta3), and internal sphincter contraction (alpha1)
- Thus, if there is sympathetic activity, there is filling
- Receptor difference between the bladder wall and sphincter allows opposite effect - Parasympathetic
- Pelvic Nerves (S2, S3, S4)
- This controls bladder wall contraction (detrusor muscle), and internal sphincter relaxation
- Thus, if there is parasympathetic activity, there is emptying

Explain the 5 components of the micturition reflex (receptor —> afferent etc…)
- Receptor
- Is the stretch receptor in the bladder wall
- The receptors in the posterior ure thra are highly sensitive to stretch, thus when this area begins to fill you really feel it - Afferent
- A signal is sent from the receptor to the centre by the pelvic nerves - Centre
- This afferent signal is received by the spinal cord (in the sacral segment)
- However, despite being a spinal reflex, it is actually under the control of the pons, medulla, hypothalamus and cortex (so the signal is also taken here) - Efferent
- A signal is sent from the centres to the effector by the pelvic nerves - Effector
- The signal is received by the detrusor muscle of the bladder wall
- As well as the internal and external sphincters

explain the 2 types of higher centre control of the micurition reflex
- Facilitatory areas
- Consists of the pons (the pons micturition centre is the most important switch for micturition
- Has the main pontine switch
- These are the ones that will relax the external sphincter, so will help with voiding
Sorta 1.
Hypothalamus which stimulates pons
- Inhibitory areas
- Consists of the cerebral cortex and midbrain
- These areas inhibit the pontine switch so that the external sphincter remains closed

what are the 3 abnormalities you can have of miturition
- Interruption of the afferent nerves from the bladder
- Sensory is lost - Interruption of both afferent and efferent nerves
- The bladder is denervated - Interruption of facilitatory and inhibitory pathways descending from the brain
- The lesion is above L1 or L2 meaning the higher centre control is lost
What is an atonic bladder
- Is simply a large dilated bladder that does not empty as a result of sensory nerve fibres being damaged (FIRST ABNORMALITY OF MICTURITION)
- Therefore, a person loses bladder control despite the intact efferent fibres to the bladder
- All the reflex contractions of the bladder are abolished meaning it becomes distended, thin walled and hypotonic
- In patients with damaged sensory nerve damage will have a bladder that fills to capacity and overflows a few drops at a time through the urethra, thus patients will have overflow incontinence
- It will be a hypotonic bladder
- This is commonly caused by;
- Crush injury to sacral region of spinal cord
- Tumours
- Tabes dorsalis (degeneration of spinal cord)
What is an automatic bladder
- Is caused by damage to the spinal cord above the sacral region
- This causes the loss of high centre control, but maintains the sacral micturition reflex centres - therefore will empty without somatic input, just empties due to strecth reflex of detrusor muscle
- The bladder will become overfilled, and the urine will dribble through the sphincters, thus patients will have overflow incontinence
- Without higher control, it is a pure automatic reflex
- The external sphincter in this condition will be relaxed (as the higher control pontine centre which controls it won’t be there)
what is renal clearance
· Renal clearance - To evaluate the ability of the kidneys to handle solutes and water
· Describes the rate at which substances are removed (or cleared) from plasma
· Renal clearance - the rate of removal by the kidneys
· The rate at which the kidney excretes a solute into the urine equals the rate at which the solute disappears from the plasma
· Thus renal clearance is the ratio of urinary excretion (Ux × V̇) to plasma concentration
· The higher the renal clearance, the more plasma that is cleared of the substance
what is the formula for renal clearnace
· The formula for renal clearance is: Cl = (UxV) / P
· The concentration of solute in the urine (U) The volume of urine formed in a given time (V) The concentration of solute in systemic blood plasma (P)
what is the substance tested for GFR and what does a fall in this indicate
Creatinine clearance is used clinically to assess glomerular filtration rate
Fall in GFR may be the first and only clinical sign of kidney disease
what is the perfect substance to use to measure the glomerular filtration rate (but it is not used clinically)
inulin
Say for each of these whether they are stimulated, relaxed or contracted.
For Filling:
Sympathetic system:
parasympathetic system
internal sphincter
external spincter
detrusor muscle
Stimulated
Relaxed
Contracted
Contracted
Relaxed

