Renal Blood Flow and Glomerular Filtration Rate Flashcards
Filtration
- blood to lumen
- Formation of a cell- and mostly protein-free plasma filtrate in the glomerulus. Filtration of the blood by the glomerulus forms the ultrafiltrate. At this point the ultrafiltrate has the same composition as blood, except for protein and blood cell components of blood. The ultrafiltrate enters the Bowman’s capsule and flows through the lumen of the renal tubule. As it flows through the lumen its composition and volume are altered by tubular activity, i.e. by reabsorption and secretion.
Rebasorption
- lumen to blood
- Movement (transport) of a substance out of the tubular lumen. Most substances eg salt and water, cross the epithelial layer of the tubule (ie enter via the apical membrane, and cross the basolateral membrane, or via paracellular pathways). These substances then enter the renal interstitium and are returned back to the bloodstream via uptake into nearby capillaries. However, reabsorption can also involve the uptake of a substance from the tubular lumen into tubular epithelial cells, where it is degraded or metabolized
Secretion
- blood to lumen
- Movement (transport) a substance into the tubular lumen. This involves transport of a substance from peritubular capillary blood, across the epithelial layer of the tubule (ie across the basolateral membrane and then the apical membrane, into the tubular lumen. However, some substances are added to the tubular lumen after synthesis by the epithelial cells (Note: glomerular filtration is NOT a form of secretion)
Excretion
- lumen to external environment
- Elimination of a substance from the body in the final urine. The net effects of filtration, reabsorption and secretion determine the rate at which a substance is excreted.
Quantitative Relationship between Filtration, Reabsorption, Secretion & Excretion
Excreted/min= Filtered/min – Reabsorbed/min + Secreted/min
Basic Physiological Functions of the KIdney
- Eliminate METABOLIC WASTE PRODUCTS
- Eliminate FOREIGN COMPOUNDS
- Regulate BODY FLUID OSMOLALITY
- Regulate plasma IONIC COMPOSITION
- Regulate EXTRACELLULAR FLUID VOLUME
- Help regulate ARTERIAL PRESSURE
- Help maintain ACID-BASE BALANCE
- Metabolize POLYPEPTIDE HORMONES
- Act as an ENDOCRINE organ:
»Erythropoietin
» 1,25-(OH)2vitamin D3
»Renin
Two Types of Postglomerular Capillaries
- pertitubular capillaris in the cortex
- vasa recta in the medulla (only 10% of renal blood flow)
Ultrafiltration
- The formation of a virtually protein-free filtrate of plasma as blood passes through the glomerular capillaries
- The glomerular ultrafiltrate has a composition identical to plasma except for the almost complete absence of protein.
‘• The ultrafiltrate is formed as fluid passes through the walls of the glomerular capillaries and into Bowman’s space (from whence it can enter the proximal convoluted tubule)
Inulin
•filtered and secreted
Sodium
•filtered and partially reabsorbed and excreted
Glucose
•filtered and completely rebasorbed
PAH
•filtered and secreted and excreted
Important Characteristics of Renal Blood Flow
- Essentially all blood flows through glomeruli.
- Blood traverses sequentially through the following structures: Aorta, renal artery (and large branches), interlobar artery, arcuate artery, interlobular artery, afferent arteriole, glomerular capillaries, efferent arteriole, postglomerular capillaries (peritubular capillaries in cortex; vasa recta in medulla), venules, interlobular vein, arcuate vein, interlobar vein, renal vein (see video on hold in library)
- Unusual aspects of this vascular anatomy:
- The inflow and outflow vessels of the glomerular capillaries are both arterioles (high resistance).
- There are 2 capillary beds (glomerular and postglomerular) arranged in sequence. These capillary beds are specialized for either filtration (glomerular capillaries) or absorption (postglomerular capillaries).
The ease with which a solute can pass across the filtration barrier is determined by:
- Molecular Size
- Electrical Charge
- Molecular Shape
Molecular Size
•Freely filtered: substances with low molecular weight (<5500 Da) and small effective molecular radius (<2 nm). These substances are present in Bowman’s space at the same concentration as in plasma.
-Examples: urea, glucose, inulin.
• Solute passage is increasingly restricted as molecular weights exceed 14 kDa and effective molecular radii exceed 2 nm.
-Albumin has a molecular weight of 69 kDa and a 3.6 nm molecular radius — characteristics that limit its passage across the filtration barrier.
Electrical Charge
- Macromolecular substances with a negative charge pass less readily than neutral substances. This phenomenon is termed electrostatic restriction. In turn, positively charged macromolecules pass more readily than neutral substances.
- Albumin (the primary plasma protein) has a valence of –18 at pH 7.4. Thus, in addition to the molecular size of albumin, its passage across the filtration barrier is also impeded by its polyanionic nature.
Molecular Shape
•Loosely coiled, elongated molecules without tertiary structure (which are relatively deformable) can cross the filtration barrier more readily than globular proteins of equivalent molecular weights and hydrodynamic radii. This phenomenon is termed steric hindrance.
What characteristics of the ultrafiltration barrier give it the ability to restrict solute passage on the basis of size, charge and shape?
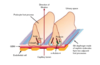
Ultrafiltrate is formed as components of plasma in the capillary lumen pass through
- endothelial fenestrations
- the basal lamina (basement membrane)
- filtration slits (the space between pedicels) into Bowman’s space



Size Barrier
No discrete structure of the capillary wall has an obvious dimensional configuration that might provide the size barrier.
- Endothelial fenestrations (70 nm diameter) and filtration slits (25-60 nm diameter) are far too large!
- Traditionally, the size barrier function has been ascribed to the basement membrane (300-350 nm thick), which consists of a highly cross-linked type IV collagen framework containing sialoglycoprotein and sulfated glycoprotein fibers in a hydrated gel. Steric hindrance is thought to occur as globular macromolecules interact with this meshwork.
- The slit diaphragm (which spans the filtration slits) is emerging as an important size barrier limiting filtration of plasma protein. Its structure is assembled in a highly organized, almost zipper-like fashion. Novel proteins (nephrin, podocin, etc) represent integral components of this structure. Deletions or mutations of the genes encoding any one of these proteins results in a nephrotic syndrome (the term applied to array of diseases that result in the excretion of massive amounts of protein in the urine). As slit diaphragm structure and function are becoming better understood, the glomerular basement membrane is beginning to be viewed as a “prefilter,” with the slit diaphragm viewed as the final critical size barrier
Charge Barrier
- Proteoglycans and other glycoproteins with negative charges are present on the surface of endothelial cells, pedicels and slit diaphragm (still debated?), as well as throughout the basal lamina. These fixed negative charges underlie electrostatic restriction against the passage of large, negatively charged molecules.
- Many glomerular diseases are associated with a loss of fixed negative charges, allowing increased passage of protein through the glomerular capillary wall.
Size or Charge — Which is more important?
•Estimates provided by mathematical models:
- 30% ↓ in fixed negative charge density → 25-fold ↑ in albumin filtration.
- 100% ↑ in pore radius → 5-fold ↑ in albumin filtration.
- Suggests that electrostatic restriction plays a prominent role in limiting albumin transit across the filtration barrier.
- Loss of fixed charges in the glomerular filtration barrier may trigger a physical rearrangement of the structure that influences the size of the barrier. (Glycoproteins contribute to the structure of the basement membrane and also contribute fixed negative charges.) Most glomerular diseases compromise both the size- and charge-selective properties of the filtration barrier.
- In the final analysis, any alteration that leads to the filtration of protein at a rate exceeding the ability of the proximal tubule to reabsorb protein will result in excretion of protein in the urine.
Proteinuria
Proteinuria (the presence of protein in the urine) is the hallmark of glomerular injury.
Advantages of the parallel arrangement of multiple capillaries:
- It minimizes the hydrostatic pressure drop between entrance and exit vessels
- It provides a very large surface area for filtration