Orthopaedic Problems of The Hand Flashcards
Who is dupuytrens most common in?
Men
What is the aetiology for dupuytrens disease?
- Autosomal dominant – variable penetrance
- Sporadic in 30% of cases
- Onset may be sex linked
- Almost exclusively white races
- Few sporadic reports in other races
Associations with diabetes, alcohol, tobacco, HIV, epilepsey
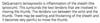
What is the pathology and clinical presentation of dupuytrens contracture?
Fibrosis and contracture of the palmar fascia
Inability to extend fingers fully (test is to put hand flat on the table)
Assoicated with puckering of the skin and palpable nodules.
Little and ring fingers are usually worst affected.
Very slowly progressive - Painless - main symptoms are associated with catching the affected finger becoming snagged in posckets or poking the eye during face washing.
Are you able to flex the finger in dupuytrens contracture?
Yes
What are the non-operative treatments for dupuytrens disease?
Observe (until the condition progresses to the point that they need an operation)
Radiotherapy
Splints do not work
What are the operative treatments for dupuytrens disease?
Partial fasciectomy - main treatment
Dermo-fasciectomy
Arthrodesis
Amputation
Percutaneous needle fasciectomy
Collagenase
Dupuytrens will eventually come back after treatment
What is recurrence rate of dupuytrens contracture at 5 years?
50%
What are the benefits of percutaneous needle fasciectomy?
Quick
No wounds
Return to normal activities in 2-3 days
Does not prevent traditional surgery in the future
What are the limitations of percutaneous needle fasciectomy?
HIgher recurrence (although the procedure can be repeated)
Risk of nerve injury
What is the risk of using collagenase?
RIsk of tendon rupture
(since collagen is everywhere)
What is the pathophysiology of trigger finger?
Swelling in tendon catches on pulley
(stenosing tenosynovitis in flexor tendon sheath)
Intermittent locking of the finger in flexion
The pulleys are like the hoops on a fishing rod (they keep the tendon close to the bone)
Who does trigger finger commonly affect?
- Women more frequent than men
- 40s-60s
- Ring > Thumb > Middle
- Repetitive use of hand ?
- Local trauma
- Associations
- RA, DM, Gout
What is the diagnosis of trigger finger?
- Patient History
- Clicking sensation with movement of digit
- Lump in palm under pulley
- May have to use other hand to ‘unlock’
- ‘Clicking’ may progress to ‘locking’
Palpable lump in the palm over A1 pulley
Feel the triggering around the A1 - pulley
What is non-operative treatment of trigger finger?
Splintage
Steroid
What is operative treatmetn of trigger finger?
Percutaneous release
Open surgery
What rendon sheaths are involved in de quervain’s syndrome?
Abductor pollicis longus
Extensor pollicis brevis
Where is the pain in de quervain’s tenovangitis syndrome?
radial aspect of the distal forearm and wrist.
Marked pain on ulnar deviation with the thumb held in the patients hand (finkelsteins sign)
Localised tenderness over tunnel - may have warmth, linear swelling or crepitus
What is the pathological process of de quervain’s tenosynovitis?
Inflammation of the sheath that surrounds the APL and the EPB
Who is de quervain’s common in?
Common in females
Age 50-60
Increased in post partum and lactating females
Activites with frequent thumb abduction and ulnar deviation

What is a differential for de Quervain’s tenovangitis?
Base of the thumb OA
What is non-operative and operative treatment of de Quervain’s syndrome?
Non-operative = splints and steroid injection
Operative = Decompression
What is a ganglion?
Myxoid degeneration from joint synovia
- Arises from joint capsule, tendon sheath or ligament
A ganglion cyst is a tumor or swelling on top of a joint or the covering of a tendon (tissue that connects muscle to bone). It looks like a sac of liquid (cyst). Inside the cyst is a thick, sticky, clear, colorless, jellylike material.
Who gets ganglia?
More common in females
more common on the back of the hand than the front of the hand
May be associated with recurrent injury around the wrist
What is the clincal presentation of ganglia?
Lump
Firm
Non-tneder
Change in size (classic sign is that it changes in size to become bigger or smaller)
Smooth
Occasionally lobulated
Normally not fixed to underlying tissues
Never fixed to the skin
What is ganglia treatment?
Non-operative:
Reassure and observe
Aspiration - you need a thick needle because the fluid is so thick
Hit with a bible
(it will spontaneously go away in many cases)
Operative:
Excision including the root
Recurrence rate is very high after surgery
What are the clinical features of OA of the base of the thumb?
Pain
Stiffness
Swelling
Deformity
Loss of function
How common is OA in the base of the thumb?
Common - 1 in 3 women get OA in the base of the thumb
What are the changes in the thumb when there is base of thumb OA present?
Dorsal subluxation
Metacarpal adduction
MCPJ hyperextension
What are the non-operative treatments for OA base of thumb?
- Life style modifications
- NSAIDS
- Splint
- Steroid Injection
What are the operative treatments for OA base of thumb?
Trapeziectomy - gold standard, good pain releif.
The space where the trapezium was fills in with scar tissue. There is loss in strength of the thumb. Pinch strength may feel like it is improving because there is less pain after operation (but this will occur about 3-6 months after the operation).
Fusion (only works if one joint is affected) - young people with heavy handling job - fusing is better for maintaining strength than a trapeziectomy.
Replacement
