Oral path photos Flashcards

Odontogenic Myxoma
o Radiographic feature: thin septations at right angles to each other. Thin, wispy septations.
o Can grow large; resection is difficult as tumor is jelly-like and may send myxoid fingers into surrounding bone, not visible on imaging.
o Conservative resection necessary.

Oral Melanotic Macule
- 2:1 female predilection
- tan to brown round macule, usually solitary
- tx not required, biopsy if unknown etiology

Ranula
- Mucocele on floor of mouth
- plunging = dissecting through mylohyoid. May grow large.
- DDx
- Dermoid cyst is in ddx,
- Cystic Hygroma (neck lymphangioma).

Hemangioma (Arterio-venous Malformation)
- Multilocular RL ddx (if intraosseous).
- Aspirate prior to biopsy
- Congenital hemangiomas often spontaneous resolve toward adulthood

Erythema Multiforme
- Probably autoimmune; 50% pts had other infx
-
EM Minor: Target lesions of skin, assoc w/ HSV
- Mostly male, 20s-30s, self-limiting (2-6 wks)
- 20% recurrence, irreg lesions necrose/ulcer
-
EM Major: (Stevens-Johnsons Syndrome)
- Sick Patients, trigger often a med, 5M/yr
-
Toxic Epidermal Necrolysis (TEN)
- Old pts, tx in burn unit, sloughing of skin

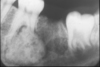
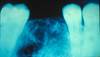
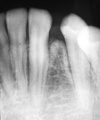
Osteosarcoma
Freq in long bones: proximal tibia/distal femur, in pubescent boys. Gnathic osteosarcs = older age, average 35. X-ray hallmarks of osteosarcoma: asymm widening of PDL space; bone formation in soft tissue; bone formation above the alveolar crest. Spiking root resorption; irregular, ill-defined borders; may be RL to Mixed to RO; “Sun-burst” only in 25% of jaw osteosarcs. Radical resection is only effective tx.

Veruccous Carcinoma
- A less aggressive, less invasive variant of conventional SCC.
- Exhibits a prominent papillary, exophytic growth pattern.
- Does not metastasize; if metastatic, likely represents transformation to conventional SCC.

Eruption Cyst
o Overlying soft-tissue impacted tooth, may clinically appear blue or red.
o Usually, spontaneous resolution with subsequent eruption of the tooth, no need to make an incision.

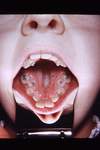
Wegeners Granulomatosus
- “Saddle Nose,” affects Respiratory/Renal Systems
- Oral Manifestation = “Strawberry Gingiva”
- before renal involvement
- florid, granular hyperplasia (bumpy, hemorrhagic, and friable)
- bone destruction and tooth mobility

Central Giant Cell Granuloma
- Multilocular RL ddx; some may be aggressive.
- Can be associated with aneurysmal bone cyst
- Same histology seen in Cherubism; Brown Tumors of hyperparathyroidism.

Macule
- A circumscribed flat area, up to 1.0 cm in diameter
- Perceptibly different color from surrounding tissue

Papule
- A circumscribed, solid elevation in skin or mucosa

Buccal Bifurcation Cyst
Be familiar with typical clinical presentation
- associated tooth is vital
- tx with curettage
- DO NOT extract tooth.

McCune-Albright Syndrome
- Polyostotic Fibrous Dysplasia
- Cafe-au-lait (Coast of Maine)
- Endocrinopathies (early menses in Females)
- Hockey Stick deformity to Femur

Squamous Papilloma
- HPV subtypes 6 & 11 found in 50% of squamous papillomas
- tongue, lips; most common soft tissue mass of soft palate
- cauliflower appearance, finger-like projections
- Papilloma Ddx= Squamous Papilloma, Verruca Vulgaris, Condyloma Acuminata, Heck’s Disease

HSV-1
- Cold sores…not the same as Canker sores/apthae
- Typically initially presents in Kids, crusting mouth, low fever
- Rarely initial presentation in adults, high fever, pharnyx

Erythema Multiforme
Probably autoimmune; 50% pts had other infx
EM Minor: Target lesions of skin, assoc w/ HSV
- Mostly male, 20s-30s, self-limiting (2-6 wks)
- 20% recurrence, irreg lesions necrose/ulcer
EM Major: (Stevens-Johnsons Syndrome)
- Sick Patients, trigger often a med, 5M/yr
Toxic Epidermal Necrolysis (TEN)
- Old pts, tx in burn unit, sloughing of skin

Osteoma
- Benign neoplasm; multiple seen in Gardner’s syndrome.
- Primarily craniofacial distribution.

Amelanotic Melanoma
- 20% of oral melanomas are non-pigmented
- Oral are of the Acral Lentiginous variety
- Rarely ulcerate

Epulis Granulomatosum
- histologically identical to pyogenic granuloma
- occurs within the socket of a recently extracted tooth
- hyperplastic growth of granulation tissue

Fibrous Dysplasia
Developmental; post-zygotic mutation of GNAS1 gene. Monostotic (late mutation), Polyostotic (intermediate mutation), Syndromic (early mutation).
- Polyostotic may affect just craniofacial bones.
- “Ground glass” radiopaque appearance to bone expansion. Ill-defined borders.
- Syndromes:
- McCune-Albright (FD, café au lait pigmentations (coast of Maine), endocrinopathies)
- Jaffe-Lichtenstein (FD, café au lait pigmentations).
- Growth often continues through adolescence, then slows/stops in adulthood. Lesions may need to be debulked periodically.

Cherubism
- presents in Kids
- multiple quadrants of CGCL
- often resolves in adulthood, sometimes not.

Thyroglossal Duct Cyst
o Midline of neck, anywhere from foramen cecum (base of tongue) down to thyroid.
o Usually attached to hyoid bone; cyst moves when patient swallows.
o Surgical procedure is Sistrunk procedure: remove cyst and involved portion of hyoid bone.

Epstein Barr
- HHV-4

Oral Melanoacanthoma
- Rapid onset and growth
- Buccal mucosa most common site
- Dark-brown or black pigmentation
- Flat or slightly raised
- Biopsy tends to incite resolution.
- Considered reactive, but etiology unknown.
- Black Females 20s/30s most common

Actinic Lentigo (Liver spots)
- not considered premalignant (no cytologic atypia)
- UV damaged skin
- Common in people with light skin (90% of whites over 70 years); Rare under 40 years
- well-demarcated, irregular borders
- usually multiple, may coalesce (to form into one)
- no treatment required (cosmetic)

Neurofibroma
- most common BPNST
- most percutaneous including facial skin; oral lesions less common
- young adults, M=F
- tongue & buccal; mandible
- soft painless nodule; unencapsulated bundles of spindle cells
- Multiple: concern for neurofibromatosis

Angular Chelitis
- usually related to candidiasis, but may have other cutaneous bacterial microfloral admixed
- redness, cracking of corners of the mouth
- often waxes and wanes
- may require topical or systemic antifungal therapy

Mucoepidermoid Carcinoma
- Malignant. Most common malignant salivary gland neoplasm.
- Any location; parotid and palate more common.
- Bluish nodule, may be ulcerated.
- Mucicarmine special stain highlights mucous cells histologically.
- Graded: low, intermediate, high grades.
- DDX in the palate: necrotizing sialometaplasia, MEC, SCC.

Giant Cell Fibroma

Hemangioma

COC with Ghost Cells
o Maxillary = mandible; often anterior.
o Mixed RL/RO ddx; can sometimes appear multilocular RL.
o On histology: ghost cell formation.
o Usually enucleates fairly easily (peels out of bone); low recurrence rate.

Cicatricial Pemphigoid
- Cicatricial means “scarring”
- Pemphigoid is between epithelium & Base Mem
- less deadly
- detectable with Direct Immunofluoresence 90% of the time
- Symblepheron: conjunctival adhesion bulbar/palpebral
- blocks eye ducts, overproduces keratin

Residual Periapical Cyst
- Radiographically appears as an oval or round lucency within the alveolar ridge at the site of a previous tooth extraction.
- Histology is similar to the periapical cyst…
- The clinical history and radiographic description that you provide are necessary to diagnose this

Peripheral Ossifying fibroma
- Part of Gum Bump Differential
- Peripheral Ossifying Fibroma
- Peripheral Giant Cell Granuloma
- Pyogenic Granuloma
- Fibroma

Mixed Tumor

Central Ossifying Fibroma
- neoplastic, unlimited growth potential, needs to be completely removed if possible.
- More common in mandible, slow growth typically.
- Downward bowing of the inferior border of the mandible is a radiographic feature of large OF’s.
- Juvenile active ossifying fibroma (JAOF or just active OF): more aggressive, rapid growth, more common in maxilla, younger patients. Can occur in ethmoid bone, other craniofacial bones.

Crouzon’s Syndrome
- Premature closing of cranial sutures.
- Normal intelligence.
- Proptosis (shallow orbits, bulging eyes appearance),
- mid-face hypoplasia, high arched palate.
- Beaten copper skull films.

Epidermoid Cyst
o Extremely common dermal cyst, along continuum of epidermoid cyst – dermoid cyst – teratoma. EIC has only 1 germ cell layer (epidermal)
o Filled with keratin – stinky. Patients may complain of periodic smelly “drainage”, if in continuity with skin surface.
o Multiple EICs can be seen in patients with Gardner Syndrome.

Neurofibroma
- most common BPNST
- most percutaneous including facial skin; oral lesions less common
- young adults, M=F
- tongue & buccal; mandible
- soft painless nodule; unencapsulated bundles of spindle cells
- Multiple: concern for neurofibromatosis

Epulis Granulomatosum
- histologically identical to pyogenic granuloma
- occurs within the socket of a recently extracted tooth
- hyperplastic growth of granulation tissue

Seborrheic Keratosis
- acquired, benign proliferation of epidermal cells
- very common; correlated w/ sun exposure
- “stuck-on rasin” or “stuck-on burnt cornflake”
- many are not pigmented
- No treatment required
- Multiple seborrheic keratosis with pruritis (itching)
- Leser-Trelat sign - indication of internal malignancy

Florid Cemento Osseous Dysplasia
- Predilection for Afr-Amer females, 30-50 years old
- Multiple quadrants involved
- Usually no symptoms or expansion
- Radiogrpahic: Lobular, irregular ROs with RL areas
- Pattern similar to PCOD & Focal COD
- 50% are associated with idiopathic bone cavities
- Treatment: usually not necessary
- Maintain oral health to avoid extraction/dentures
- Exposure of sclerotic masses to oral cavity may cause chronic osteomyelitis

Gingival Cyst of the Adult
- Considered the soft tissue counterpart to the lateral periodontal cyst
- 60% - 70% of cases occur in the mandibular canine and premolar area, on the facial gingiva or alveolar mucosa; maxillary cysts may also be found in the incisor region
- Patients are usually in the 5th to 6th decades

Verruca Vulgaris
- HPV types 2, 4, 6, or 40 are found in almost every lesion
- contagious, may spread via auto-inoculation
- tx must include base of the lesion
- HPV Differential
- Verruca Vulgaris
- Condyloma Acuminata
- Heck’s Disease
- Squamous Papilloma

Sturge-Weber Syndrome
- Related to CN V
- Port Wine stain of skin
- may include buccal mucosa

Sialolithiasis
- Most common in submandibular gland (tortuous Wharton’s duct), but also seen in parotid, minor glands.
- the condition that forms a “Sialolith”

Central Ossifying Fibroma
- neoplastic, unlimited growth potential, needs to be completely removed if possible.
o More common in mandible, slow growth typically.
o Downward bowing of the inferior border of the mandible is a radiographic feature of large OF’s.
o Juvenile active ossifying fibroma (JAOF or just active OF): more aggressive, rapid growth, more common in maxilla, younger patients. Can occur in ethmoid bone, other craniofacial bones.

Epidermoid Cyst
o Extremely common dermal cyst, along continuum of epidermoid cyst – dermoid cyst – teratoma. EIC has only 1 germ cell layer (epidermal)
o Filled with keratin – stinky. Patients may complain of periodic smelly “drainage”, if in continuity with skin surface.
o Multiple EICs can be seen in patients with Gardner Syndrome.

Calcifying Epithelial Odontogenic Tumor
o Most often posterior mandible.
o Mixed RL/RO ddx; often presents with central dense calcification, often around crown of an impacted tooth, then more radiolucent toward periphery.
o Produces amyloid-like material (histology) and concentric calcifications called Leisegang rings.
o Conservative excision, lower recurrence rate.

Oral Melanoacanthoma
- Rapid onset and growth
- Buccal mucosa most common site
- Dark-brown or black pigmentation
- Flat or slightly raised
- Biopsy tends to incite resolution.
- Considered reactive, but etiology unknown.
- Black Females 20s/30s most common

Necrotizing Sialometaplasia
- Chronic, non-healing ulcer, can grow large, but often comes on relatively quickly (compared to SCC). Often located on palate.
- Clinical and histologic ddx includes Mucoepidermoid Carcinoma and SCC. Ischemic necrosis? Biopsy often incites resolution.
Salivary gland neoplasia, general trends:
o Parotid is most common location, followed by mainor glands.
o Neoplasia in parotid is twice as likely to be benign; still more likely to be benign than malignant in submandibular gland; but in sublingual gland, neoplasia is less common, but much more likely to be malignant than benign.
o In minor glands, palate is most common location, followed by lips. All in all, neoplasia in minor glands is more likely to be malignant than benign (50/50 on palate).
o Even malignancies may be slow growing and not very aggressive.
o Concerning clinical features include facial nerve paresthesia or paralysis; ulceration.
o Most common benign salivary gland neoplasm: pleomorphic adenoma. Most common malignant salivary gland neoplasm: mucoepidermoid carcinoma (at SAMMC, it seems to be adenoid cystic carcinoma).

Recurrent HSV1

Pemphigus Vulgaris
- Splits epithelium up from itself
- Positive Nikolsky Sign (sloughing of tissue)
- 60-80% die if untreated
Osteoma
- Benign neoplasm
- multiple seen in Gardner’s syndrome.
- Primarily craniofacial distribution

Warthin Tumor
- Benign; typical patient is older male, smoker.
- Warthin tumor primarily occurs in the parotid, often bilaterally, although not necessarily at the same time.

Gorlin Syndrome
- AKA Nevoid Basal Cell Carcinoma Syndrome
- Mandibular prognathism
- numerous basal cell carcinomas (frequent head and neck region)
- 65% palmar and plantar pits
- 60-75% of patients have skeletal abnormalities: bifid ribs, spina bifida, etc.

Central Giant Cell Lesion
- Multilocular RL; some may be aggressive.
- Can be associated with aneurysmal bone cyst features.
- Same histology seen in cherubism; brown tumors of hyperparathyroidism.

Adenoid Cystic Carcinoma
- Malignant. Minor glands more common; palate, also sinonasal. Middle age, 40’s and male common. Slow, relentless growth, pain and paresthesia can be seen. This tumor spreads via skip lesions along nerves. Difficult to resect; eventually results in distant metastases (lung).
- All salivary gland neoplasms need to be completely excised due to propensity for unlimited local growth.
- Additional treatment modalities (neck dissection for lymph node metastases, chemo, radiation) is dependent on lymph node mets, and on grade of tumor (high grade, poorly differentiated).
- Frey’s syndrome: damage to auriculotemporal branch of facial nerve during parotid surgery: gustatory sweating (sweating of facial skin during salivation).

Lupus Vulgaris
- mucocutaneous lesions of secondary tuberculosis
- Mycobacterium

Herpetiform Apthous

Crouzon’s Syndrome
- Premature closing of cranial sutures.
- Normal intelligence.
- Proptosis (shallow orbits, bulging eyes appearance),
- mid-face hypoplasia, high arched palate.
- Beaten copper skull films.

Actinic Keratosis
- precancerous skin growth-squamous carcinoma
- ill-defined, scaly plaques < 1 cm in diameter
- tan, red or skin colored
- related to cumulative lifetime sun exposure
- more common on sun-exposed sites in fair-skinned elderly
- face, neck, forearms, & dorsal hands
- excess keratin build-up may cause cutaneous horn
- same as in squamous cell carcinomaestimated: progress to malignancy in 5-20% (10%)

Cervical Facial Actinomycosis
- Woody induration to soft tissue
- bacteria burrow straight through hard and soft tissue (direct extension)
- often create a draining sinus tract extraorally
- Can mimic malignancy. Part of normal flora

OKC
o On multilocular radiolucent ddx.
o May grow large and cause expansion, but more often tracks up ramus of mandible.
o Maxillary OKC’s can grow into maxillary sinuses.
o Must be completely removed; high recurrence rate with curettage about 30%). Can do peripheral ostectomy or marsupialization to shrink cyst prior to excision/resection.
o Multiple OKC’s are highly suggestive of Nevoid Basal Cell Carcinoma Syndrome (aka Gorlin Syndrome).

Gorlin Syndrome

Ameloblastic Fibroma
- Kiddo tumor, 1st-2nd decades common.
- Should be on the ddx for RL lesion in a kid, or mixed RL/RO in a kid.
- Can grow large, displace teeth.
- Conservative excision; recurrences may require resection.

Central Ossifying Fibroma
- neoplastic, unlimited growth potential, needs to be completely removed if possible.
o More common in mandible, slow growth typically.
o Downward bowing of the inferior border of the mandible is a radiographic feature of large OF’s.
o Juvenile active ossifying fibroma (JAOF or just active OF): more aggressive, rapid growth, more common in maxilla, younger patients. Can occur in ethmoid bone, other craniofacial bones.

Oral Melanoacanthoma
- Rapid onset and growth
- Buccal mucosa most common site
- Dark-brown or black pigmentation
- Flat or slightly raised
- Biopsy tends to incite resolution.
- Considered reactive, but etiology unknown.
- Black Females 20s/30s most common

Oral Melanotic Macule
- 2:1 female predilection
- tan to brown round macule, usually solitary
- treatment is not required
- biopsies recommended for most oral presentations of etiology is unknown
- may be watch this clinical history and presentation is not concerning

COC-Calcifying Odontogenic Cyst
o Maxillary = mandible; often anterior.
o Mixed RL/RO ddx; can sometimes appear multilocular RL.
o On histology: ghost cell formation.
o Usually enucleates fairly easily (peels out of bone); low recurrence rate.

Multiple Mucosal Neuromas
- Diagnositic for Multiple Endocrine Neoplasia in kids

Hemangioma (Arterio-venous Malformation)
- Multilocular RL ddx (if intraosseous).
- Aspirate prior to biopsy
- Congenital hemangiomas often spontaneous resolve toward adulthood

Canalicular Adenoma
- Benign. 75% are found in the upper lip; half of remainder in anterior buccal mucosa.
- Should be at the top of the ddx for a submucosal nodule of the upper lip.
- May be multifocal
- (Mucoceoles don’t exist on Upper Lip)

Adenomatoid Odontogenic Tumor
o 2/3rds tumor: Anterior, maxilla, female, young, impacted canine
o Included in the mixed RL/RO ddx.
o Usually shells out of bone in large pieces, easily. If removed completely, no recurrence.

Ameloblastic Fibroodontoma
o Kiddo tumor, 1st-2nd decades common. Should be on the ddx for RL lesion in a kid, or mixed RL/RO in a kid.
o Can grow large, displace teeth.
o Conservative excision; recurrences may require resection.

AOT
o 2/3rds tumor: Anterior, maxilla, female, young, impacted canine
o Included in the mixed RL/RO ddx.
o Usually shells out of bone in large pieces, easily. If removed completely, no recurrence.

Lupus Vulgaris
- mucocutaneous lesions of secondary tuberculosis
- Mycobacterium

Crouzon’s Syndrome
- Premature closing of cranial sutures.
- Normal intelligence.
- Proptosis (shallow orbits, bulging eyes appearance),
- mid-face hypoplasia, high arched palate.
- Beaten copper skull films.

Amyloidosis
- deposition of an extracellular proteinaceous substance known as amyloid…waxy
- Can be caused by end stage Renal Disease
- associated with Multiple Myeloma

Probably Treacher-Collins Syndrome

Denture Stomatitis

Mixed Tumor
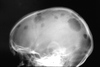
Multiple Myeloma
- “Punched-out radiolucency”. Neoplastic proliferation of plasma cells (the end differentiation of B-cells.) May produce amyloid.

Epidermoid Cyst
o Extremely common dermal cyst, along continuum of epidermoid cyst – dermoid cyst – teratoma. EIC has only 1 germ cell layer (epidermal)
o Filled with keratin – stinky. Patients may complain of periodic smelly “drainage”, if in continuity with skin surface.
o Multiple EICs can be seen in patients with Gardner Syndrome.

Goriln’s Syndrome
- AKA Nevoid Basal Cell Carcinoma Syndrome
- Mandibular prognathism
- numerous basal cell carcinomas (frequent head and neck region)
- 65% palmar and plantar pits
- 60-75% of patients have skeletal abnormalities: bifid ribs, spina bifida, etc.

Botryoid odontogenic cyst
- 5th-6th decade of life, 75-80% occur in mandibular premolar-canine-lateral incisor areas
- Usually well-circumscribed lucency lateral to vital tooth
- polycystic (grapelike) multilocular appearance
- Type of lateral periodontal cyst

Actinic Keratosis
- precancerous skin growth-squamous carcinoma
- ill-defined, scaly plaques < 1 cm in diameter
- tan, red or skin colored
- related to cumulative lifetime sun exposure
- more common on sun-exposed sites in fair-skinned elderly
- face, neck, forearms, & dorsal hands
- excess keratin build-up may cause cutaneous horn

fibroma

COC
o Maxillary = mandible; often anterior.
o Mixed RL/RO ddx; can sometimes appear multilocular RL.
o On histology: ghost cell formation.
o Usually enucleates fairly easily (peels out of bone); low recurrence rate.

Multiple Mucosal Neuromas
- characteristic of MEN 2b syndrome
- Thyroidectomy by age 30 to prevent cancer

Lipoma

Acinic Cell Adenocarcinoma
- Malignant, mostly found in parotid
- Commonly found at SAMMC

Actinic Chelitis
- typically associated with candidiasis

Condyloma Acuminata
- HPV 16 and 18 - higher risk for SCC (anogenital)
- Watch where you put your tongue!!

Basal cell carcinoma
- most common cancer
- from sun exposure (cumulative)
- if in young person, look for Gorlins aka Nevoid Basal Cell Carcinoma Syndrome
Cementoblastoma
o Young adults, kids; more common in posterior mandible.
o Often painful, expansile. Neoplastic, must be removed.
o RO, or mixed RL/RO, with RL rim. Attached to tooth root(s).
o Associated teeth need to be extracted.

Ameloblastic Fibroma
o Kiddo tumor, 1st-2nd decades common. Should be on the ddx for RL lesion in a kid, or mixed RL/RO in a kid.
o Can grow large, displace teeth.
o Conservative excision; recurrences may require resection.

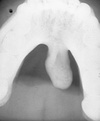
Nasal Palatine Duct Cyst
o Anterior maxillary midline, can present either to the facial or palatal to teeth 8/9.
o Heart-shaped radiolucency, associated teeth are vital.
o Simple curettage usually curative.

Ossifying Fibroma
- Adults - age 20-40, mean 32 years
- No sex or racial predilection
- 80% in mandible
- Radiolucent to opaque with a lucent rim
- BOWING OF INFERIOR BORDER OF MANDIBLE
- NEOPLASTIC - completely excise, curettage, or en bloc for more aggressive tumors
- A few cases have been identified with mutations in the tumor suppressor gene HRPT2
- Associated with a rare condition: HYPERPARATHYROIDISM - JAW-JAW TUMOR SYNDROME. Characterized by parathyroid adenoma or carcinoma, ossifying fibromas of the jaws, renal cysts, and Wilm’s tumors (specific kind of malignant kidney tumor usually seen in small kids.)

OKC
o On multilocular radiolucent ddx.
o May grow large and cause expansion, but more often tracks up ramus of mandible.
o Maxillary OKC’s can grow into maxillary sinuses.
o Must be completely removed; high recurrence rate with curettage about 30%). Can do peripheral ostectomy or marsupialization to shrink cyst prior to excision/resection.
o Multiple OKC’s are highly suggestive of Nevoid Basal Cell Carcinoma Syndrome.

palisaded encapsulated neuroma

basal cell carcinoma

cervical facial actinomycosis

hsv 1

Ameloblastoma
o Benign neoplastic, can be aggressive. Must be completely removed, often requires resection of up to 1 cm clear margins.
o Can occur anywhere, but posterior mandible common.
o Included in the multilocular radiolucent ddx.
o Several histologic sub-types; desmoplastic ameloblastoma is the only clinically relevant sub-type.
o Desmoplastic ameloblastoma: More common in anterior maxilla; radiographically similar to a benign fibro-osseous lesion (BFOL), ground glass, than to multilocular RL. May be considered more aggressive.

amyloidosis

Ameloblastic Fibroodontoma
o Kiddo tumor, 1st-2nd decades common. Should be on the ddx for RL lesion in a kid, or mixed RL/RO in a kid.
o Can grow large, displace teeth.
o Conservative excision; recurrences may require resection.

scrofula

zygomycosis

Dentigerous Cyst
o Most common developmental odontogenic cyst
o Most commonly associated with impacted thirds and canines
o If an impacted tooth has a pericoronal radiolucency greater than about 3mm, tissue should be curetted and sent for histologic eval to rule out more concerning entities.
o Tx: Extract tooth and send tissue to pathology

Central Odontogenic Fibroma
o Anterior maxillar, posterior mandible.
o When in maxilla, may produce a characteristic palatal “notch” clinically.
o RL, can have RO flecks.
o Enucleation, low recurrence.

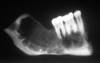
Odontoma
o Compound versus complex. Hamartoma.
o Multiple odontomas can be seen in Gardner syndrome, cleidocranial dysplasia, others.

Langerhans
“Eosinophilic granuloma” is another name for a unifocal lesion. Monoclonal proliferation of Langerhans antigen presenting cells. Radiographically, “teeth floating in air.” May be multifocal in jaws. Disseminated Langerhans = poor prognosis; limited may have a good prognosis. Chemo, rad.

Periapical Cemento Osseous Dysplasia

Veruccous Carcinoma
- Verrucous Carcinoma: A less aggressive, less invasive variant of conventional SCC. Exhibits a prominent papillary, exophytic growth pattern. Do not metastasize; if metastatic, likely represents transformation to conventional SCC.

oral melanoacanthoma

toxic epidermal necrolysis

men 2b

Lateral Periodontal Cyst
o Associated with vital tooth.
o Bone window, simple enucleation is usually curative.
o Mandibular canine/premolar area most common; similar to gingival cyst of the adult (soft tissue counterpart to LPC).
Odontogenic Myxoma
o Radiographic feature: thin septations at right angles to each other. Thin, wispy septations.
o Can grow large; resection is difficult as tumor is jelly-like and may send myxoid fingers into surrounding bone, not visible on imaging.
o Conservative resection necessary.

Idiopathic Bone Cavity
- Usually younger patients (common in our BMT’s). Mandible, male predilection. Trauma? Empty bone cavity; ostectomy during “biopsy” often incites bleeding and healing. RL scallops tooth roots.

angular chelitis

hereditary hemorrhagic telangectasia

amyloidosis

laryngeal papillomatosis

Mccune Albright
o Syndromes: McCune-Albright (FD, café au lait pigmentations (coast of Maine), endocrinopathies); Jaffe-Lichtenstein (FD, café au lait pigmentations).

Plaque
In skin, a circumscribed, elevated, superficial and solid area greater than 1.0 cm in diamter

Vesicle
A small (less than 1.0 cm in diameter) circumscribed elevation of the skin or mucosa containing fluid

Florid Cemento Osseous Dysplasia
- Predilection for African American females, 30-50 years old
- Multiple quadrants involved
- Usually no symptoms or expansion
- Radiogrpahic: Lobular, irregular radiopacities with radiolucent areas
- Pattern of maturation similar to PCOD and Focal COD
- 50% are associated with idiopathic bone cavities
- Treatment: usually not necessary
- Maintain oral health to avoid extraction/dentures
- Exposure of sclerotic masses to oral cavity may cause chronic osteomyelitis

kaposi

pemphigus vulgaris

giant cell fibroma

Osteoma
Benign neoplasm; multiple seen in Gardner’s syndrome. Primarily craniofacial distribution.
Odontogenic Myxoma
o Radiographic feature: thin septations at right angles to each other. Thin, wispy septations.
o Can grow large; resection is difficult as tumor is jelly-like and may send myxoid fingers into surrounding bone, not visible on imaging.
o Conservative resection necessary.

scc

schwannoma

condyloma acuminata

Condensing Osteitis
Reactive bone sclerosis, due to inflammatory etiology, usually non-vital tooth. Can regress following resolution of inflammation.

gardner

Periapical Cemento Osseous Dysplasia
o In general, early lesions are RL, over time become mixed, late lesions are RO. Periapical cemental dysplasia (PCD): anterior mandible; florid COD = at least two quadrants affected.
o Rarely see expansion. In edentulous areas, sclerotic bone/cementum masses sequester, create opportunity for infection (osteomyelitis).
o Vital teeth
- Know sub-categories and etiologies of BFOL’s:
o Cemento-osseous dysplasia (PCD, focal, florid): reactive.
o Ossifying fibroma/juvenile active ossifying fibroma: neoplastic.
o Fibrous dysplasia: Developmental (GNAS1 mutation).

Mixed Tumor

hemangioma

stevens johnson syndrome

erosive lichen planus

Oral Lymphoepithelial Cyst
o Very common, often a yellowish nodule, 1 cm, on lateral posterior tongue or tonsillar area, soft palate. “Ectopic” tonsillar/lymphoid tissue. Simple excision. Be able to recognize these/properly include these in a ddx if given a clinical photo.

stevens johnson syndrome

chronic multifocal candida

Osteosarcoma
Most common in long bones: proximal tibia/distal femur, in pubescent boys. Gnathic osteosarcs = older age, average 35. Radiographic hallmarks of osteosarcoma: asymmetric widening of the PDL space; bone formation in soft tissue; bone formation above the alveolar crest. Also can see spiking root resorption; irregular, ill-defined borders; may be RL to mixed to RO; “sun-burst” seen only in 25% of jaw osteosarcs. Radical resection is only effective treatment.

Idiopathic Osteosclerosis
Vital teeth, no definitive etiology. No expansion

schwannoma

median rhomboid glossitis

wegeners granulomatosus

fibrous dysplasia (mccune albright)

oral melanotic macule

Osteosarcoma
Most common in long bones: proximal tibia/distal femur, in pubescent boys. Gnathic osteosarcs = older age, average 35. Radiographic hallmarks of osteosarcoma: asymmetric widening of the PDL space; bone formation in soft tissue; bone formation above the alveolar crest. Also can see spiking root resorption; irregular, ill-defined borders; may be RL to mixed to RO; “sun-burst” seen only in 25% of jaw osteosarcs. Radical resection is only effective treatment.

OKC
o On multilocular radiolucent ddx.
o May grow large and cause expansion, but more often tracks up ramus of mandible.
o Maxillary OKC’s can grow into maxillary sinuses.
o Must be completely removed; high recurrence rate with curettage about 30%). Can do peripheral ostectomy or marsupialization to shrink cyst prior to excision/resection.
o Multiple OKC’s are highly suggestive of Nevoid Basal Cell Carcinoma Syndrome.

Osteosarcoma
Most common in long bones: proximal tibia/distal femur, in pubescent boys. Gnathic osteosarcs = older age, average 35. Radiographic hallmarks of osteosarcoma: asymmetric widening of the PDL space; bone formation in soft tissue; bone formation above the alveolar crest. Also can see spiking root resorption; irregular, ill-defined borders; may be RL to mixed to RO; “sun-burst” seen only in 25% of jaw osteosarcs. Radical resection is only effective treatment.

Dentigerous Cyst
o Most common developmental odontogenic cyst
o Most commonly associated with impacted thirds and canines
o If an impacted tooth has a pericoronal radiolucency greater than about 3mm, tissue should be curetted and sent for histologic eval to rule out more concerning entities.
o Tx: Extract tooth and send tissue to pathology

erosive lichen planus

kaposi

Focal Cemento Osseous Dysplasia
Usually Solitary lesion (vs. 2+ lesions in one quadrant)
88% female, predilection for African Americans
77% posterior mandible, often edentulous area
Rare symptoms or expansion
RAdiographic: SAme stages as PCOD
Gross characteristics: Small hemorrhagic calcifications upon surgical removal/biopsy
Treatment: None necessary
Confirm dx by biopsy
Periodic radiogrpahic follow up
Recommended: May progress to florid COD

medium rhomboid glossitis

Sialolithasis
Most common in submandibular gland (tortuous Wharton’s duct), but also seen in parotid, minor glands.

inflammatory fibrous hyperplasia

melanoma

Ameloblastoma
o Benign neoplastic, can be aggressive. Must be completely removed, often requires resection of up to 1 cm clear margins.
o Can occur anywhere, but posterior mandible common.
o Included in the multilocular radiolucent ddx.
o Several histologic sub-types; desmoplastic ameloblastoma is the only clinically relevant sub-type.
o Desmoplastic ameloblastoma: More common in anterior maxilla; radiographically similar to a benign fibro-osseous lesion (BFOL), ground glass, than to multilocular RL. May be considered more aggressive.

Calcifying Epithelial Odontogenic Tumor
o Most often posterior mandible.
o Mixed RL/RO ddx; often presents with central dense calcification, often around crown of an impacted tooth, then more radiolucent toward periphery.
o Produces amyloid-like material (histology) and concentric calcifications called Leisegang rings.
o Conservative excision, lower recurrence rate.

squamous papilloma

Nnasal Palatine Duct Cyst
o Anterior maxillary midline, can present either to the facial or palatal to teeth 8/9.
o Heart-shaped radiolucency, associated teeth are vital.
o Simple curettage usually curative.

Periapical Cyst
Loss of lamina dura
Relatively well-circumscribed radiolucency surrounding the apex/root
May reach a large size

squamous papilloma

condyloma acuminata

Dermoid Cyst
o Midline of body, often midline floor of mouth, or inner canthus of eye.
o Two germ cell layers: epidermoid and mesodermal.

Fibrous Dysplasia
- Developmental; post-zygotic mutation of GNAS1 gene. Monostotic (late mutation), polyostotic (intermediate mutation), syndromic (early mutation). Polyostotic may affect just craniofacial bones.
o “Ground glass” radiopaque appearance to bone expansion. Ill-defined borders.
o Syndromes: McCune-Albright (FD, café au lait pigmentations (coast of Maine), endocrinopathies); Jaffe-Lichtenstein (FD, café au lait pigmentations).
o Growth often continues through adolescence, then slows/stops in adulthood. Lesions may need to be debulked periodically.

stuge weber

Cementoblastoma
o Young adults, kids; more common in posterior mandible.
o Often painful, expansile. Neoplastic, must be removed.
o RO, or mixed RL/RO, with RL rim. Attached to tooth root(s).
o Associated teeth need to be extracted.

actinic chelitis

traumatic neuroma

Cementoblastoma
o Young adults, kids; more common in posterior mandible.
o Often painful, expansile. Neoplastic, must be removed.
o RO, or mixed RL/RO, with RL rim. Attached to tooth root(s).
o Associated teeth need to be extracted.

Ameloblastoma
o Benign neoplastic, can be aggressive. Must be completely removed, often requires resection of up to 1 cm clear margins.
o Can occur anywhere, but posterior mandible common.
o Included in the multilocular radiolucent ddx.
o Several histologic sub-types; desmoplastic ameloblastoma is the only clinically relevant sub-type.
o Desmoplastic ameloblastoma: More common in anterior maxilla; radiographically similar to a benign fibro-osseous lesion (BFOL), ground glass, than to multilocular RL. May be considered more aggressive.

Dentigerous Cyst
o Most common developmental odontogenic cyst
o Most commonly associated with impacted thirds and canines
o If an impacted tooth has a pericoronal radiolucency greater than about 3mm, tissue should be curetted and sent for histologic eval to rule out more concerning entities.
o Tx: Extract tooth and send tissue to pathology

Periapical Cyst
Loss of lamina dura
Relatively well-circumscribed radiolucency surrounding the apex/root
May reach a large size

Central Giant Cell Lesion
Multilocular RL; some may be aggressive. Can be associated with aneurysmal bone cyst features. Same histology seen in cherubism; brown tumors of hyperparathyroidism.

actinic lentigo

melanoma

wegners granulomatosus

Dentigerous cyst
o Most common developmental odontogenic cyst
o Most commonly associated with impacted thirds and canines
o If an impacted tooth has a pericoronal radiolucency greater than about 3mm, tissue should be curetted and sent for histologic eval to rule out more concerning entities.
o Tx: Extract tooth and send tissue to pathology

hereditary hemorrhagic telangectasia

Squamous Papilloma
Part of the Human Papilloma Virus Differntial
Squamous Papilloma
Verruc Vulgaris
Condyloma Acuminata
Heck’s Disease
High Risk sub-types are 16 & 18

Focal Cemento Osseous Dysplasia
- Usually Solitary lesion (vs. 2+ lesions in one quadrant)
- 88% female, predilection for African Americans
- 77% posterior mandible, often edentulous area
- Rare symptoms or expansion
- RAdiographic: SAme stages as PCOD
- Gross characteristics: Small hemorrhagic calcifications upon surgical removal/biopsy
- Treatment: None necessary
- Confirm dx by biopsy
- Periodic radiogrpahic follow up
- Recommended: May progress to florid COD

Osteosarcoma
Most common in long bones: proximal tibia/distal femur, in pubescent boys. Gnathic osteosarcs = older age, average 35. Radiographic hallmarks of osteosarcoma: asymmetric widening of the PDL space; bone formation in soft tissue; bone formation above the alveolar crest. Also can see spiking root resorption; irregular, ill-defined borders; may be RL to mixed to RO; “sun-burst” seen only in 25% of jaw osteosarcs. Radical resection is only effective treatment.

Mucocele
Mucocele (mucous extravasation phenomenon):
o Does not occur on the upper lip.
o Most common on lower lip; may be anterior buccal mucosa or other locations. Again, not upper lip.
o Increases in size with salivation. If excised, take surrounding minor salivary glands along with the mucocele to decrease chance of recurrence (traumatized glands).

verruca vulgaris

Condensiing Osteitis
Reactive bone sclerosis, due to inflammatory etiology, usually non-vital tooth. Can regress following resolution of inflammation.

Oral Lymphoepithelial Cyst
o Very common, often a yellowish nodule, 1 cm, on lateral posterior tongue or tonsillar area, soft palate. “Ectopic” tonsillar/lymphoid tissue. Simple excision. Be able to recognize these/properly include these in a ddx if given a clinical photo.

aperts

Osteoporotic Marrow Defect
Middle-aged female typical; ill-defined RL, usually body of mandible, can be site of previous extraction. Can mimic metastasis. Defect filled with normal bone marrow.

periphreal giant cell granuloma

Ameloblastoma
o Benign neoplastic, can be aggressive. Must be completely removed, often requires resection of up to 1 cm clear margins.
o Can occur anywhere, but posterior mandible common.
o Included in the multilocular radiolucent ddx.
o Several histologic sub-types; desmoplastic ameloblastoma is the only clinically relevant sub-type.
o Desmoplastic ameloblastoma: More common in anterior maxilla; radiographically similar to a benign fibro-osseous lesion (BFOL), ground glass, than to multilocular RL. May be considered more aggressive.

Brown Tumor

Ameloblastic Fibroma
o Kiddo tumor, 1st-2nd decades common. Should be on the ddx for RL lesion in a kid, or mixed RL/RO in a kid.
o Can grow large, displace teeth.
o Conservative excision; recurrences may require resection.

Necrotizing Sialometaplasia
- Chronic, non-healing ulcer, can grow large, but often comes on relatively quickly (compared to SCC). Often located on palate. Clinical and histologic ddx includes mucoepidermoid carcinoma and SCC. Ischemic necrosis? Biopsy often incites resolution.
- Salivary gland neoplasia, general trends:
o Parotid is most common location, followed by mainor glands.
o Neoplasia in parotid is twice as likely to be benign; still more likely to be benign than malignant in submandibular gland; but in sublingual gland, neoplasia is less common, but much more likely to be malignant than benign.
o In minor glands, palate is most common location, followed by lips. All in all, neoplasia in minor glands is more likely to be malignant than benign (50/50 on palate).
o Even malignancies may be slow growing and not very aggressive.
o Concerning clinical features include facial nerve paresthesia or paralysis; ulceration.
o Most common benign salivary gland neoplasm: pleomorphic adenoma. Most common malignant salivary gland neoplasm: mucoepidermoid carcinoma (at SAMMC, it seems to be adenoid cystic carcinoma).

parulis

men2b

Condensing osteitis
Condensing osteitis: Reactive bone sclerosis, due to inflammatory etiology, usually non-vital tooth. Can regress following resolution of inflammation.

acute atrophic candida

Brachial Cleft Cyst
o Lateral neck is common, but may occur anywhere from ear downt o clavicle, along SCM. Lymphoepithelial cyst on histology.

Ranula
Mucocele on floor of mouth; plunging = dissecting through mylohyoid. May grow large. Dermoid cyst is in ddx, also cystic hygroma (neck lymphangioma).

trisomy 21
apert

Oral Lymphoepithelial Cyst
o Very common, often a yellowish nodule, 1 cm, on lateral posterior tongue or tonsillar area, soft palate. “Ectopic” tonsillar/lymphoid tissue. Simple excision. Be able to recognize these/properly include these in a ddx if given a clinical photo.
Osteosarcoma
Most common in long bones: proximal tibia/distal femur, in pubescent boys. Gnathic osteosarcs = older age, average 35. Radiographic hallmarks of osteosarcoma: asymmetric widening of the PDL space; bone formation in soft tissue; bone formation above the alveolar crest. Also can see spiking root resorption; irregular, ill-defined borders; may be RL to mixed to RO; “sun-burst” seen only in 25% of jaw osteosarcs. Radical resection is only effective treatment.

Ranula
Mucocele on floor of mouth; plunging = dissecting through mylohyoid. May grow large. Dermoid cyst is in ddx, also cystic hygroma (neck lymphangioma).

condyloma acuminata

gardner

actinic karatosis

Mucocele
Mucocele (mucous extravasation phenomenon):
o Does not occur on the upper lip.
o Most common on lower lip; may be anterior buccal mucosa or other locations. Again, not upper lip.
o Increases in size with salivation. If excised, take surrounding minor salivary glands along with the mucocele to decrease chance of recurrence (traumatized glands).
Ideopathic Osteosclerosis
Vital teeth, no definitive etiology. No expansion

Sialolithasis
Most common in submandibular gland (tortuous Wharton’s duct), but also seen in parotid, minor glands.

Adenomatoid Odontogenic Tumor
o 2/3rds tumor: Anterior, maxilla, female, young, impacted canine
o Included in the mixed RL/RO ddx.
o Usually shells out of bone in large pieces, easily. If removed completely, no recurrence.

Bulla
A fluid filled blister greater than 1.0 cm in diameter appearing as a circumscribed area of seperation between the epidermis and the underlying dermis

Odontoma
o Compound versus complex. Hamartoma.
o Multiple odontomas can be seen in Gardner syndrome, cleidocranial dysplasia, others.

Developmental Inclusion Cyst of Neonate
o Epstein’s pearls and Bohn’s nodules – distribution.
Spontaneously resolve.

schwannoma

Central Odontogenic Fibroma
o Anterior maxillar, posterior mandible.
o When in maxilla, may produce a characteristic palatal “notch” clinically.
o RL, can have RO flecks.
o Enucleation, low recurrence.

hsv 1

stuge weber

OKC
o On multilocular radiolucent ddx.
o May grow large and cause expansion, but more often tracks up ramus of mandible.
o Maxillary OKC’s can grow into maxillary sinuses.
o Must be completely removed; high recurrence rate with curettage about 30%). Can do peripheral ostectomy or marsupialization to shrink cyst prior to excision/resection.
o Multiple OKC’s are highly suggestive of Nevoid Basal Cell Carcinoma Syndrome.

Idiopathic Osteosclerosis
Vital teeth, no definitive etiology. No expansion.

Mucocele
Mucocele (mucous extravasation phenomenon):
o Does not occur on the upper lip.
o Most common on lower lip; may be anterior buccal mucosa or other locations. Again, not upper lip.
o Increases in size with salivation. If excised, take surrounding minor salivary glands along with the mucocele to decrease chance of recurrence (traumatized glands).

Glandular Odontogenic Cyst
o Propensity for mandible; premolar/incisor region, crosses midline.
o Can include on multilocular RL ddx.
o Can be aggressive; resection may be necessary.
o Histologically, may be a pitfall for pathologists: can be misdiagnosed as intraosseous mucoepidermoid carcinoma.

verruca vulgaris

melanoma

Fibroma

Infected Dentigerous Cyst

Focal Cemento Osseous Dysplasia
Usually Solitary lesion (vs. 2+ lesions in one quadrant)
88% female, predilection for African Americans
77% posterior mandible, often edentulous area
Rare symptoms or expansion
RAdiographic: SAme stages as PCOD
Gross characteristics: Small hemorrhagic calcifications upon surgical removal/biopsy
Treatment: None necessary
Confirm dx by biopsy
Periodic radiogrpahic follow up
Recommended: May progress to florid COD

hecks disease

Cementoblastoma
o Young adults, kids; more common in posterior mandible.
o Often painful, expansile. Neoplastic, must be removed.
o RO, or mixed RL/RO, with RL rim. Attached to tooth root(s).
o Associated teeth need to be extracted.

neurofibroma

Parulis

OKC
o On multilocular radiolucent ddx.
o May grow large and cause expansion, but more often tracks up ramus of mandible.
o Maxillary OKC’s can grow into maxillary sinuses.
o Must be completely removed; high recurrence rate with curettage about 30%). Can do peripheral ostectomy or marsupialization to shrink cyst prior to excision/resection.
o Multiple OKC’s are highly suggestive of Nevoid Basal Cell Carcinoma Syndrome.

Periapical Cemento Osseous Dysplasia

Juvenile Active Ossifying Fibroma
o Juvenile active ossifying fibroma (JAOF or just active OF): more aggressive, rapid growth, more common in maxilla, younger patients. Can occur in ethmoid bone, other craniofacial bones. CARDED

allergic fungal sinusitis

Adenomatoid Odontogenic Tumor
o 2/3rds tumor: Anterior, maxilla, female, young, impacted canine
o Included in the mixed RL/RO ddx.
o Usually shells out of bone in large pieces, easily. If removed completely, no recurrence.

OKC
o On multilocular radiolucent ddx.
o May grow large and cause expansion, but more often tracks up ramus of mandible.
o Maxillary OKC’s can grow into maxillary sinuses.
o Must be completely removed; high recurrence rate with curettage about 30%). Can do peripheral ostectomy or marsupialization to shrink cyst prior to excision/resection.
o Multiple OKC’s are highly suggestive of Nevoid Basal Cell Carcinoma Syndrome.

Ideopathic Osteosclerosis
Vital teeth, no definitive etiology. No expansion

hecks disease

Gingival Cyst of the Adult

Necrotizing Sialometaplasia
- Chronic, non-healing ulcer, can grow large, but often comes on relatively quickly (compared to SCC). Often located on palate. Clinical and histologic ddx includes mucoepidermoid carcinoma and SCC. Ischemic necrosis? Biopsy often incites resolution.
- Salivary gland neoplasia, general trends:
o Parotid is most common location, followed by mainor glands.
o Neoplasia in parotid is twice as likely to be benign; still more likely to be benign than malignant in submandibular gland; but in sublingual gland, neoplasia is less common, but much more likely to be malignant than benign.
o In minor glands, palate is most common location, followed by lips. All in all, neoplasia in minor glands is more likely to be malignant than benign (50/50 on palate).
o Even malignancies may be slow growing and not very aggressive.
o Concerning clinical features include facial nerve paresthesia or paralysis; ulceration.
o Most common benign salivary gland neoplasm: pleomorphic adenoma. Most common malignant salivary gland neoplasm: mucoepidermoid carcinoma (at SAMMC, it seems to be adenoid cystic carcinoma).

minor apthous

Fibrous Dysplasia
- Developmental; post-zygotic mutation of GNAS1 gene. Monostotic (late mutation), polyostotic (intermediate mutation), syndromic (early mutation). Polyostotic may affect just craniofacial bones.
o “Ground glass” radiopaque appearance to bone expansion. Ill-defined borders.
o Syndromes: McCune-Albright (FD, café au lait pigmentations (coast of Maine), endocrinopathies); Jaffe-Lichtenstein (FD, café au lait pigmentations).
o Growth often continues through adolescence, then slows/stops in adulthood. Lesions may need to be debulked periodically.

scc

epstein barr

pseudomembranous candida

Periapical Cyst
Loss of lamina dura
Relatively well-circumscribed radiolucency surrounding the apex/root
May reach a large size

major apthous

Pustule
A circumscribed, superficial elevation of the skin, up to 1.0 cm in diameter, containing purulent material

Anneurysmal Bone Cyst
More common in long bones than gnathic. Rapid expansion, can be aggressive. Female predilection, young patients. Multilocular RL, rapidly expansile. Histology: “Suicide” giant cells at periphery of blood lakes. Primary or secondary; primary is thought to be neoplastic, gene mutation. Secondary is in association with another entity (central giant cell lesion, etc).

OKC
o On multilocular radiolucent ddx.
o May grow large and cause expansion, but more often tracks up ramus of mandible.
o Maxillary OKC’s can grow into maxillary sinuses.
o Must be completely removed; high recurrence rate with curettage about 30%). Can do peripheral ostectomy or marsupialization to shrink cyst prior to excision/resection.
o Multiple OKC’s are highly suggestive of Nevoid Basal Cell Carcinoma Syndrome.

Verrucous Carcinoma
Verrucous Carcinoma arising in a setting of oral submucous fibrosis - use of betel quid

mucocutaneous candidiasis

basal cell carcinoma

Dermoid Cyst
o Midline of body, often midline floor of mouth, or inner canthus of eye.
o Two germ cell layers: epidermoid and mesodermal.

Odontogenic Myxoma
o Radiographic feature: thin septations at right angles to each other. Thin, wispy septations.
o Can grow large; resection is difficult as tumor is jelly-like and may send myxoid fingers into surrounding bone, not visible on imaging.
o Conservative resection necessary.

Odontoma
o Compound versus complex. Hamartoma.
o Multiple odontomas can be seen in Gardner syndrome, cleidocranial dysplasia, others.

oral melanoacanthoma

reticular lichen planus

Fibrous Dysplasia
- Developmental; post-zygotic mutation of GNAS1 gene. Monostotic (late mutation), polyostotic (intermediate mutation), syndromic (early mutation). Polyostotic may affect just craniofacial bones.
o “Ground glass” radiopaque appearance to bone expansion. Ill-defined borders.
o Syndromes: McCune-Albright (FD, café au lait pigmentations (coast of Maine), endocrinopathies); Jaffe-Lichtenstein (FD, café au lait pigmentations).
o Growth often continues through adolescence, then slows/stops in adulthood. Lesions may need to be debulked periodically.

Mixed Tumor

idipoathic osteosclerosis
Vital teeth, no definitive etiology. No expansion.
