Neuropathology 2 Flashcards
A: Describe [Radicular Root Pain]
B: What causes it (2)
C: What, associated with this, causes a [dull & local pain]?
A: [LSS Pain-Lightning/Stabbing/Shooting Pain] that situates itself in the dermatomal distribution of a dorsal root
B:
- Inflammation of [Dorsal Root]
- Extramedullary compression of [Dorsal Root]
C: The extramedullary lesion itself
A: Clinical sensory deficits correlate to the ____[vertebrae / spinal cord] level
B: Which between the two listed above extends down longer?
A: Clinical sensory deficits correlate to the Spinal Cord level
B: Vertebral column becomes longer than spinal cord during development
Describe the sensory signs for Spinothalamic Tract lesions (3)
- Contralateral deficit of pain and temp
- [Sacral Sparing during intramedullary lesions] (since sacral fibers are far lateral)
- [Deficit is up to dermatomal level in EXTRAmedullary lesions]

A: Clinical Manifestation for [ANT Spinal Artery Occlusion] (3)
B: What types of things cause this?
A:
1) Sudden Hyperreflexic spastic paraparesis
2) Loss of Pain/Temp inferior to the lesion
3) Preserved [2TVP-2point/Touch/Vibration/Position]
B:
- Atherosclerotic aortic Dz
- Aortic Surgery

A: Describe [SuB ACute Combined Degeneration] (2)
B: What are the causes (3)
A: [Demyelinating lesions] in Posterior and Lateral Columns (usually at thoracic level) –>
- loss of [2TVP- 2point discrimination/Touch/vibration/position] of LE
- but with…*
- intact Pain and Temp
B: [SuB ACute Combined Degeneration]
1) B12 Deficiency
2) Copper Deficiency
3) AIDS/HIV

A: Describe [ALS-Amyotrophic Lateral Sclerosis]
B: Clinical Manifestation (3)
C: Prognosis and Tx
D: Issue with diagnosing ALS
E: Breathing Evaluation (2)
A: Progressive Degeneration of [UMN Pyrimidal Betz Cells] AND [LMN ANT Horn cells <–AFFECTED MORE!] –> Spheroid lesions
B:
1) Weakness affecting speech/chewing/breathing and eventually proximal limb atrophy = LMN sign
2) Fasciculations Diffusely = LMN sign
3) [Exaggerated Reflexes + Babinski] = UMN sign
C: Fatal but can give [Riluzole (glutamate blocker)] since glutamate over exites motor neurons
D: UMN signs may be first confused with a cervical spinal cord lesion!
E: many pts fear respiratory failure. Mitigate with:
- Aggressive = [Tracheostomy Mechanical Ventilation]
- Supportive= [CPAP vs. BiPAP]

Motor Neuron Disease
A: ALS-Amyotrophic Lateral Sclerosis Pgn
B: Mode of Inheritance
A: Progressive Degeneration of [UMN Pyrimidal Betz Cells] AND [LMN ANT Horn cells <–AFFECTED MORE!] –> Spheroid lesions & has the WORST PGN OF ALL MOTOR NEURON DISORDERS (50% Die within 3 years from respiratory failure or profound weakness)
B: [RARELY FAMILIAL (Chromo 21 Superoxide Dismutase Gene mutation) but affects more Males]

Clinical Manifestation of Tabes Dorsalis (4)
1st) Lightning pain from [initial dorsal root lesion] (from loss of DRG and dorsal root)
2nd) Loss of [2VP-2point discrimination/vibration/position] from dorsal column degeneration –> [Romberg] + [Stomping Gait] + [Charcot Joints]
3rd) Loss of ALL SENSES (from loss of DRG and dorsal root)
4th) [Areflexia but Preserved Strength]

A: Describe the 3 main sx for [Brown Sequard Syndrome]
B: Causes (3)
- Contralateral STT Loss of Pain/Temp
- Ipsilateral DCP Loss of 2TVP-2point/Touch/Vibration/[Position Proprioreception]
* 3.* Ipsilateral CST Loss –> Muscle Weakness
B:
[(Extramedullary Tumor] vs. Trauma vs. (Herniated Disc)]

A: Pathophysiology of Myasthenia Gravis
B: When does it onset? Describe the 2 types.
C: What things are preserved in this dz? (2)
D: What is Myasthenic Fatigue
A: Autoimmune Dz that blocks and INC degradative turnover of [postsynpatic nicotinic ACh Receptors]]
B: [Generalized (more common) vs. Ocular] and occurs at ANY AGE!
- Generalized= P DDD WF
[Ptosis/[Diplopia from Disconjugate gaze]/Dysarthria/Dysphagia/ [Weakness(Respiratory and limbs)/ Fatigue-especially with certain activities] ]
- Ocular= [Ptosis/Diplopia] after 2-3 years of dx
C: Sensation and Reflexes
D: Exercise normally DEC ACh release but is compensated by the saftey factor.
During Myasthenia Gravis, this DEC ACh during exercise PLUS the [Loss of EPP-End Plate Potential]–> Loss of muscle depolarization –> Myasthenic Fatigue

A: 3 ways to diagnose Myasthenia Gravis
B: Which test is most specific
- Elevated [Serum Antibody against (postsynpatic nicotinic ACh Receptors)] = MOST SPECIFIC
- Positive [Tensilon Edrophonium] : short acting AChEsterase inhibitor. If after IV injection, pt feels better = they have Myasthenia Gravis
- EMG showing evidence of abnormal Neuromuscular junction transmission (i.e. repetitive nerve stimulation)
Myasthenia Gravis Tx (4)
- AntiCholinesterase drugs –> allows ACh to stick around longer
- Thymectomy (remove part of Thymus that contains ACh Receptor-like material)
- Immunosuppresants
- -[Azthioprine vs. Mycophenolate Mofetil]*
- -Cyclosporine*
- -Corticosteroids*
4. [Plasmapheresis vs. IV Immunoglobulin]= Transient but potent fixes
A: Pathophysiology of [Lambert Eaton Myasthenic Syndrome]
B: Clinical Manifestation (3)
C: Dx (3)
D: What CA is this syndrome associated with?
A: [Autoimmune attack against (Presynpatic Ca+ channel)–> No ACh release]
B:
- Fatigable weakness of Proximal limbs and trunk that mimic myopathy
- Improved briefly by exertion
- Autonomic sx (Dry mouth & Orthostasis)
C: [Nerve Stimulation test vs. EMG vs. Ab Detection]
D: usually associated with SOLC-Small Oat cell Lung Carcinoma
[Lambert Eaton Myasthenic Syndrome] tx (3)
- Tx underlying CA
- Drugs to enhance ACh release (Guanidine vs. Diaminopyridine)
- Immunosuppresants
A: What is Mononeuropathy
B: Pathophysiology
C: Dx (2)
D: Examples (3)
A: Single Major “named” nerve is involved (sensory vs. motor vs. Both)
B: [Trauma or Compression] —> focal demyelination of a nerve and possibly axonal damage if lesion is severe
C: Diagnosed with EMG and nerve testing
D: Ex:
- [Carpal Tunnel Median mononeuropathy] = most common!
- Ulnar mononeuropathy from leaning on elbow
- Peroneal mononeropathy from [lateral knee injury]
A: [Carpal Tunnel Median mononeuropathy] pathophysiology
A2: What do severe cases of this lead to?
B: Tx (3)
A: is a compression mononeuropathy that occurs when [inflammed flexor tendons/fluid retention (pregnancy) / swelling] all compress the Median nerve in the carpal tunnel –> Tingling Numbness.
A2: Severe cases = Thenar atrophy–> weakness
B: Tx
- Anti-Inflammatory
- Local Rest
- Surgery vs. Splint
- MOST COMMON MONONEUROPATHY*
What is Wallerian Degeneration?
When the peri and epineurium are preserved after the nerve trauma the axons undergoes Wallerian Degeneration. The perserved scaffolding allows sufficient axonal sprouting and regeneration within the PNS

A: Pathophysiology of [Peripheral Polyneuropathy]
B: Clinical Manifestation of [Peripheral Polyneuropathy] (4)
A: [Disorder of multiple, major AND small n.] caused by -axonal degeneration(will DEC EMG amplitude) and -secondary demyelination(will DEC EMG velocity). Both due to inadequate axoplasmic flow–>
B: 1. [early sensory loss of distal limbs (i.e. feet)]–> eventually [motor loss of distal limbs] –> atrophy–> weakness. (longest sensory cells are affected 1st)
- [Early loss of muscle stretch reflexes]
- Paresthesia= spontaneous tingling
- Dysesthesia= Unpleasant sensation from non-noxious stimulus
* eventually hands are affected as well*
A: Causes of [Peripheral Polyneuropathy] (4)
B: Dx (3)
- Hereditary
- Toxic (Drugs vs. Occupation)
- Other Multiple Mononeuropathies or autoimmune pathologies (DM vs. SLE vs. Guillain Barre)
- Idiopathic= MOST COMMON
B: EMG vs Blood testing vs. Nerve biopsy
Describe the EMG
Needle Electromyography. Electrical activity of muscles within 1 motor unit to be assessed for nerve damage and muscle dz
A: Describe Guillain Barre Syndrome
B: What Pt demographic is mostly affected by this
A: Acute Polyneuropathy manifesting as inflammation and demyelination of [peripheral n. and roots] –> [ascending NON-reflexic paralysis (includes respiratory paralysis)] –> [little sensory loss but some paresthesia and eventually reflex loss]
B: Occurs at any age, but 50% of pts have [Viral URI] prior to getting Guillain Barre
Guillain Barre Syndrome
A: Dx (2)
B: Pgn
C: What tx would help accelerate recovery?
A: Dx
1) EMG testing that reveals demyelination
2) Elevated CSF Protein and possible WBC
B: Pgn = GOOD!
C: [Plasmapheresis vs. IVIG] may shorten illness
Remember that Guillain Barre is a type of Polyneuropathy
[Chronic Acquired Polyneuropathies]
Causes (8)
[Chronic Acquired Polyneuropathies] : takes months-years to actually develop
May Destroy NITRIC
- Metabolic/Endocrine (Uremia vs. hypOthyroid)
- DM
- Nutrition (Vitamin B Deficiency)
- Infection (Leprosy = MOST COMMON WORLDWIDE)
- Toxins (alcoholism vs. lead)
- Rheumatological (RA vs. Lupus)
- Idiopathic
- CA (myeloma)
Hereditary Neuropathies
A: Pathophysiology
B: When does it onset
C: Clinical Manifestation and tx
A: known or unknown metabolic vs. genetic disorders –> [Distal sensorimotor deficits with little to no paresthesia/dysesthesia]
B: Childhood
C: Orthopedic Deformities (scoliosis/hammertoes/pes cavus): Give assistive devices, but otherwise NO TX
A: Myopathy Clinical Manifestation (3)
B: Dx (4)
A:
1) Proximal Limb (shoulders/hips) weakness and atrophy
2) LATE loss of reflexes after muscular atrophy onsets
3) Intact sensation
B:
- Family hx of muscualar dystrophy
- Elevated Creatinine Kinase (muscle enzyme)
- EMG
- Muscle Biopsy
A: Polymyositis (Describe and List causes (4))
B: Clinical Manifestation (2)
C: Dx
D: Tx
A: A type of myopathy involving multiple muscles and caused by:
1) Autoimmune= MOST COMMON IN USA
2) Viral
3) Drugs
4) CA= rare
B:
- Proximal weakness over weeks to months
- Dermatomyositis: Rash around eyes or fingers
C: *[Inflammation-mononuclear inflammatory infiltration]/necrosis on biopsy
D: Corticosteroids

Duchenne’s Muscular Dystrophy
A: pathophysiology
B: Onset
C: Clinical Manifestation (2)
A: [X-linked disorder] –> Absence of the [dystrophin muscular structural protein]–> [Cardiac / Respiratory / Proximal Limb Weakness]
B: Boyhood
C:
1) Calf Pseudohypertrophy (from muscle being replaced by fat & connective tissue)
2) Cardiorespiratory Death by Age 30
A: Describe Motor Neuron Disease
B: MOD for sub-type: Spinal Muscular Atrophy
- Clinical Manifestation
- Infant type: Name and MOD
- Teen/Adult type: Pgn
A: Degeneration of UMN, LMN, or both –> varying serverity and rate of degeneration
B: [Spinal muscular atrophy] = specifically [ANT Horn Cell degeneration] from [Chromo 5 SMN1 and 2 gene mutations]–> LMN signs of FAW- Weakness/[atrophy & areflexia] /Fasciculations
*Infantile onset = (Werdnig Hoffman) –> [AutoRecessive terminal condition –> Floppy Baby from defuse [Distal muscle atrophy]
*Milder childhood/adult onset types –> [Non-fatal Chronic Disability]
A: Clinical Manifestation of Olfactory Nerve lesion (3)
B: How are these lesions associated with Head Trauma?
A:
1) [Sinusitis vs. URI] (most common)
2) Anosmia
3) Orbitofrontal Tumor (rare)
B: Shears nerve branches in Cribiform Plate
A: Describe the difference between Binocular Diplopia and monocular Diplopia
B: Lesion of [CN 3/4/6] produces what type of Diplopia?
A:
Binocular= single image appears when 1 eye is covered
vs.
monocular= DOUBLE image appears when 1 eye is covered (comes from Psych dz vs. [ocular pathology i.e. dislocated lens])
B: Binocular Diplopia
A: Clinical Manifestation of Pineal Tumors
B: Mechanism of Dz
C: Other Causes with same manifestation (2)
A: Pupil constricts with near reflex but not with light
B: Selective disruption of [light reflex pathway] in [Pretectal Midbrain]
C:
1) Neurosyphilis (Argyll Robertson pupil)
2) [Dorsal midbrain lesions] (Pineal tumors- Parinaud’s Syndrome - will also have poor upgaze
A: What is [MLF-Medial Longitudinal Fasciculus] syndrome AKA?
B: Clinical Presentation (3)
C: What causes MLF syndrome in younger vs. Older pts?
A: Internuclear Ophthalmoplegia
[MIOS-MLF Internuclear Ophthalmoplegia Syndrome]
B:
*[Impaired ADDuction of affected eye]
+
[Normal ADDuction of affected eye during [near reflex convergence]
+
*[Nystagmus of UNaffected eye when attempting to ABduct]
C:
1) Younger pts= Multiple Sclerosis
2) Older pts= Ischemic infarction

What are the 4 common HA
- Tension
- Migraines
- [Fever/Hunger provoked]
- HEENT related
HA Red Flags:
What [signs & sx concomitant with Acute onset HA] make you suspect [Aneurysmal SubArachnoid Hemorrhage] or [Cerebellar Hematoma] (5)
- Split second / unexpected
- Worst or not previously encountered
- Loss of Consciousness
- Vertigo
- Vomiting
HA Red Flags:
[Fever & Skin Rash] with Acute Onset HA may indicate what HA Dx?
Meningitis
(keep in mind that Acute Meningitis evolves rapidly, including impaired consciousness / nuchal rigitidity / NV)
HA Red Flags:
[Immunocompromised pts] with Acute Onset HA may indicate what HA Dx? (2)
- CryptoSporidium Meningitis
- Toxoplasmosis
HA Red Flags:
[Coagulopathy / anticoagulation] with Acute Onset HA may indicate what HA Dx?
[SubDural vs. intradural Hematoma]
A: What are the 3 Clinical Questions that help to diagnose Migraine?
B: Migraine General Characteristics (6)
A:
1) Have nausea when u have HA?
2) HA exacerbated with light?
3) HA limit you from everyday functioning?
B: “DUCAP gives me Migraines, and Migraines gives me PANTOS”
Periodic
Activity-limiting
[Diminishes in freq. throughout life] (Rare for older pts to have migraines for 1st time)
Unilateral & Pulsating usually
Childhood-late vs. early adult onset
Name 5 Migraine triggers
- Stress
- Sleep Deprivation
- Hunger vs. Foods
- Alcohol/nitrates
- Fumes/smoke
Migraine Phases:
Prodrome
A: Duration
B: Sx (6)
A: Prodrome: [6-48 hour duration] occuring BEFORE Migraine
Right In Front of DDangerous HA
[Rhinorrhea vs. Lacrimation]
Irratilibility
Fatigue
Depression and Drowsiness
Hunger (Cravings for chocolate/nuts/bananas)
Migraine Phases:
Aura
A: Duration
B: Define Acephalgic Migraine
C: Describe Aura
A: Aura: [Before >during>> after] Migraine. [Migraine HA] onsets within an hour after experiencing Aura, but Aura last no longer than 1 hour.
B: Aura May not be present with Migraine. = Acephalgic Migraine
C: [Visual sx (most common)= blind spot near center of vision w/flashing & pulsating bands of light spreading across + diplopia
Migraine Phases:
PAIN
A: Location (3)
B: Duration
C: Associated sx (7)
A: Pain: [Head > Abd > Precordial]
B: _[(_minutes to hour gradual onset) with (Hours to Days duration)]
C: “DUCAP gives me Migraines, and Migraines gives me PANTOS”
- [PhoTophobia vs. PhoNophobia]
- [Aphasia + Dizziness (Cortex involvement)]
- N/V
- Thermophobia
- Osmophobia (fear of odors)
- Sensorimotor deficit (Tingling)
Migraine etx ; How are theTrigeminal nerves associated-2
Genetic [GainOfFunction mutation in excitatory NMDA receptor]–>burst of cerebral activity when triggered—>hyperemia (usually occipital lobe)–> sx. Burst is followed by ⬇︎ cortical activity= Cortical Depression tht has slow but deliberate forward advance –> Triggers Trigeminal pathway
Trigeminal afferents :
- send impulses–>Brain Stem & hypothalamus–> Nausea/Photophobia/Phonophobia
- retroactively depolarize–>release of substance P –> neurogenic inflammatory pain + vasoDilation
Migraine Phases:
PostDrome
A: Duration
B: Sx (3)
A: PostDrome: [last several hours after]
B:
- Mood change (euphoria vs. fatigue)
- concentration problems
- Scalp/muscle tenderness
Migraine
A: Tx (5)
B: 3 things to keep in mind when treating Migraine
C: Alternative Tx (5)
A: [Effective Dose NSAID] > Triptans > [Butalbital (habit forming) > DHE > Ergotamine
B:
- Treat EARLY (including Associated sx)!
- Less is Best!
- Px should be used when attacks> 2-3/month, severe and abortive therapies have failed
C: Botox vs. Butterbur vs. [St.John’s Wort] vs. Ginger vs. VitB2
Triptans Rx
A: MOA
B: When are these indicated (2)
C: When is the pt relieved of pain?
A: [5HT1B/D Receptor Agonist] –> vasoconstriction–> relieves Migraines
B:
- Pt fails to respond to [Effective Dose NSAID]
- Pt has Moderate-to-Severe Migraine Pain
C: 2 (more common) vs. 24 Hours
Triptans Rx
A: Cx (6)
B: Side Effects (2)
- Description and location
- Duration
A: Contraindications:
- Vascular Risk Factors (Ischemic Heart Dz / uncontrolled HTN / Renal Dz)
- Pregnancy
- [Basilar or Hemiplegic Migraine]
- Avoid within 24 hours of Ergotamine
- Pts taking [MAOI]
- Renal or Hepatic impairment (Ergotamine Cx)
- Age > 60 (Ergotamine Cx)
B: Side Effects =
-
Triptan Sensations
- [Pressure/Pain/Tightness/Warmth/Tingling] commonly in [Face/Limbs/Chest] but can occur anywhere
**Short duration and resolve spontaneously
+
- Serotonin Syndrome (excessive 5HT1a and 2 receptor activation)–> [Dysautonomia (Diarrhea / lacrimation)] + Encephalopathy
A: Ergotamine
- Route of Administration
- SE (2)
B: DHE
-Route of Administration (3)
Migraine specific Rx
A: Ergotamine (arterial vasoconstrictor)
- Route of Administration = Suppository ONLY
- [Severe Nausea] vs. Uterine Contractions
B: DHE (arterial & venous vasoconstrictor)
-Route of Administration = [IV vs. SubQ vs. Nasal Spray]
A: Botulinum Toxin Indication
B: Onset & Duration
A: [Chronic Migraine HA] AFTER pt has failed other meds (works by relaxing muscles)
B: Takes a week to onset but will last up to 12 weeks
A: Cluster HA Dx Criteria
B: location
C: Demographic
D: Tx (5)
A: Rapid onset (15-30 min) of([1-4 Attacks/day] each lasting [20 min - 3 Hr] x [6-12 weeks]
B: ALWAYS UNILATERAL
C: [Men during spring & fall]
D:
- Inhaled O2 100%
- Injectable Sumatriptan vs. Nasal Triptan
- Nasal Lidocaine
- Nasal DHE
- Prednisone
A: Describe Tension HA
B: Associated sx
C: Clinical Presentation
D: Common Causes (3)
A: [Classic Everyday Bilateral HA]= Most common HA
B: PhoNophobia vs. PhoTophobia (NOT AT SAME TIME)
C: [Pressing or Tightening Band head pain] lasting [4-6 Hr] maybe brought about by:
- TCA rx
- sleep deprivation
- depression
A: Describe Trigeminal Neuralgia
B: Tx
C: Most common Cause
A: SEVERE Paroxysmal attacks of jaw-radiating pain lasting [
B: [Carbamazepine 200-1200 mg/day]
C:
[Young people with Multiple Sclerosis]
A: Describe Pseudotumor Cerebri
B: Demographic
C: Clinical Presentation (2)
D: Tx (3)
A: HA that can make (mostly young Female) pts go Blind!
B: Overwt young female taking BCP
C: Papilledema + [High ICP(>250) confirmed with spinal tap]
D: Topiramate(will also –> Wt loss :-) ) vs. Acetazolamide vs. Surgery

A: Clinical Presentation of Multiple Sclerosis (3)
B: Demographic
C: Associated Causes (4)
A: “Charcot had MS and thought it was a SIN”
Charcot’s Triad
- Nystagmus
- [Intention Tremor]
- [Scanning Speech]
B: Mostly [Young White Female] but can be anyone especially those with [low Vitamin D/sun exposure]
C:
- Genetic Contribution (HLA & SNP) but MS is not Genetic Dz
- Lack of Sun –> low Vitamin D
- Viral: EBV / [Canine Distemper Virus]
- Tobacco
A: Multiple Sclerosis MOD
B: Clinical Course (4)
A: Activated [Autoreactive T Cells] travel from peripheral lymph node to CNS–>break down BBB w/interleukins that induce inflammation—> then secrete inflammatory cytokines –> [myelin destruction and neuronal death of White mater]
B: [Sx>24 hrs from demyelination]–> [remission (complete vs. partial improvmnt)] –> [Relapses every 1-2 years x 5-10 years] –> [Progressive sx with no more relapses/new lesions]

Name the 5 most common syndromes associated with Multile Sclerosis
- Optic Neuritis
- Afferent Pupillary Defect
- [Brainstem Syndromes (Internuclear Ophthalmoplegia / Ataxia / Trigeminal Neuralgia)
- [Spinal Cord Syndromes]
- Romberg (MS lesions “love” dorsal column destruction)
Optic Neuritis is a syndrome highly associated with Multiple Sclerosis
B: Sx (3)
C: Other phenomena Opitc Neuritis my be associated with (2)

Unilateral Optic Disc Swelling on fundoscopic

- [Scotoma Blindspot] vs. [Complete Blindness]
- Eye mvmnt pain
- DEC [Red/Green]
C:
- [Marcus Gunn Afferent Pupil defect]
- Uhthoff Phenomenon (heat intolerance after being placed in hot tube)
Brainstem Syndromes is a syndrome highly associated with MS
B: What’s the biggest example
B: [MIOS-MLFInternuclearOphthalmoplegiaSyndrome]

Spinal Cord Syndromes is a syndrome highly associated with MS
B: Classic signs (4)
C: How do you differentiate this from Guillan Barre
D: Description of location of spinal cord MS lesions
Pts w/”Sensory Level” should be assumed to have Spinal Cord Lesion until proven otherwise. Not MS
B:
- Deafferented Hand
- Urinary sx + Erectile Dysfunction
- Progressive Asymmetric spastic paraplegia
C: [Guillain Barre Pts] do NOT get numb in torso
D: small, located in cord periphery (especially in dorsal columns). Begin at pial surface.
A: Dx Criteria for Multiple Sclerosis (4)
B: Location of MS lesions (5)
C: Which location lesion is shown in image?
D: Which Radiography is used for dx? (2)

Dx of MS is a clinical dx + radiographic corroboration

A:
- [2 or more separate parts of CNS involved]
- [2 or more worsening episodes (separated by 1 month or more and each lasting 24 hrs)]
- Radiography: [Periventricular White Matter lesion (> 3mm) disseminated in time & space] = Dx of Exclusion
- CSF Fluid with [Oligoclonal bands] + [DEC Cell count] + [IgG abnormalitites] + [Normal Glucose & Protein] = NOT MANDATORY
B: [Corpus Callosum] / [Optic Radiation] / [Brainstem abutting 4th vt] / [T1 = Black Holes] / [Dawson’s Finger on T2W (shown in image)]
C: [Dawson’s Finger on T2W (shown in image)]
D: [MRI: T2W vs. FLAIR] (will have Hyperdense/High Signal)
Common other DDx of [MS-like presentation] include [Neuromyelitis Optica] vs. [ADEM] vs. [PML]
- Describe Neuromyelitis Optica*
- B: Clinical Presentation (3)*
Longitudinally extensive spinal cord lesion (>3 vertebrae) –> Bilateral optic neuritis

B:
- Hic-coughs
- Normal Brain
- [NMO IgG Ab Positive] - aquaporin 4 channel
Common other DDx of [MS-like presentation] include [Neuromyelitis Optica] vs. [ADEM] vs. [PML]
- Describe [ADEM-Acute Disseminated EncephaloMyelitis]*
- A: Onset*
- B: Associated sx (3)*
- C: Demographic*
A: Post-meningoencephalitis/infectious [Large FLUFFY Multifocal] lesions
B:
- HA
- Vomiting
- Drowsiness
- Meningism
C: Children

Common other DDx of [MS-like presentation] include [Neuromyelitis Optica] vs. [ADEM] vs. [PML]
- Describe PML-Progressive Multifocal Leukoencephalopathy*
- B: Location (2)*
- C: How is PML related to the drug, Natalizumab?*
- D: Demographic*
- E: Histology (3)*
Opportunistic infection 2º to [John Cunningham PolyomaVirus]—-> [multiple white matter lesions] (Hyperintense Flair signal on radiology) –> Death vs. Severe Neuro injury

B: [SubCortical Hemispheric White Matter] or [Cerebellar Peduncles]
C: Also can be caused by Rare Side Effect of Natalizumab (MS drug) in pts who are also JC Virus positive
D: HIV pts (reversal of immunosuppresion stops viral progression)
E: “PML’s HISTO is like a MOB”
- Myelin Loss (with axonal sparing)
- Bizarre astrocytes
- Oligodendroglial inclusions (–> focal discoloration in white matter & Ground glass appearance)
A: Multiple Sclerosis Tx (4)
B: Which one is used for [Acute MS Relapses]?
A: Tx
- [IV vs. Oral Methylprednisolone] (IV is preferred)
- ACTH
- Plasmapharesis
- IVIG
B: [IV vs. Oral Methylprednisolone] (IV is preferred)
Name the 5 major causes of Meningitis and descriptions of each
- Bacterial= Acute
- Fungal= affects Immunocompromised
- Amebic(Parasitic) & TB= Granulomatous
- Viral= [ASEPTIC meningitis] & [self-limiting]
- Non-Infectious= Chemical vs. [Meningeal Carcinomatosis]

Acute Bacterial Meningitis
What common bacteria affect ages…
A: Neonates
B: 1-12 months (2)
C: 1 - 16 years (3)
D: 16 - 50 years (2)
E: Age Extremes (2)
A: Neonates:- [E.Coli] vs. [Group B Strep]
B: 1-12 months: [Strep Pneumo] vs. [H.Flu]
C: 1 - 16 years: [Neisseria meningitis] vs. [H.Flu] vs. [Strep Pneumo]
D: 16 - 50 years:[Neisseria meningitis] vs. [Strep Pneumo]
E: Age Extremes: [Listeria Monocytogenes] vs. [Pseudomonas Aeruginosa]
Describe CSF findings for Bacteria Meningitis
A: Fluid Quality
B: Cells Present
C: Protein level
D: Glucose (relative to plasma)
E: Pressure
F: Tx if Bacteria Meningitis is suspected (2)
A: Cloudy
B: PMNs
C: VERY HIGH PROTEIN
D: Low Glucose
E: HIGH PRESSURE
F: 1st: [Emergent IV Dexamethasone (in adults) + Broad Spectrum Abx] —–> [specific abx after identification]

Describe CSF findings for Viral Meningitis
A: Fluid Quality
B: Cells Present
C: Protein level
D: Glucose (relative to plasma)
E: Viral Causes (2)
A: Clear
B: [Lymphocytes with lymphocytic extension along Virchow-Robin spaces]
C: Slightly High Protein
D: Normal Glucose
E:
1) Enterovirus = Most Common
2) Arbovirus (West Nile)

Describe CSF findings for TB Meningitis
A: Fluid Quality
B: Cells Present
C: Protein level
D: Glucose (relative to plasma)
A: N/A
B: Lymphocytes
C: Moderately High Protein
D: Mildly Low Glucose

List the 4 causes of Chronic Meningitis
list examples
B: Demographics (3)
C: Presentation (2)
Evolves over weeks to months
- TB–> necrotizing Granuloma (PCR testing needed)
- Fungal (Cryptococcus neoformans vs. Histoplasma vs. Coccidioides immitis)
- Parasitic (Treponema Pallidum vs. Borrelia Burgdorferi) = RARE
- Non-Infectious (Neurosarcoid)
B: Elderly vs. Malnourished vs. Immunosuppresed
C: Subtle sx of HA and/or confusion with no obvious meningeal signs

In addition to Fungal Meningitis, fungus can also cause ______, _______ and [secondary vasculitis]
B: Clinical Manifestation of [secondary vasculitis] (2)
C: Microscopy
D: Stains used for dx (3)
In addition to Fungal Meningitis, fungus can also cause encephalitis, Brain Abscess and [secondary vasculitis]
B:
1) Vascular invasion–> infarct
2) Mycotic aneurysm–> Hemorrhage
C: Granulomatous Mononuclear infiltrate (overlaps with TB)
D:
[PAS vs. Mucicarmine vs. GMS]
Fungal Meningitis
A: Which are Hyphal & Pseudohyphal (4)
B: Which are Yeast (3)
A: CAZF
[Candida/Aspergillus/Zygomycetes/Fusarium]
B: [Histoplasma/Blastomyces/Cryptococcus]

Cysticercosis / Toxoplasmosis / Amoebiasis all can cause Parasitic CNS infections
A: Describe Cysticercosis
B: Geography (2)
MOST COMMON CEREBRAL PARASITE acquired via [Taenia solium Pork cestode]
B: [SW states] and Mexico


Taenia Solium Pork Cestode

Cysticercosis / Toxoplasmosis / Amoebiasis all can cause Parasitic CNS infections
A: Describe Toxoplasmosis
B: Acquisition (2)
C: Radiology
D: Congential Toxoplasmosis is part of _____
E: Dx (2)
Protozoan that crosses placenta (pregnant women should avoid changing cat litter)
B: Cysts in meat or [cat feces oocyst]
C: Brain Abscess (MRI Ring Enhancing Lesion)
D:
-Congenital Toxo is part of TORCH (Toxo/Others/Rubella/CMV/Herpes)
D2: Dx = Serology vs. Biopsy

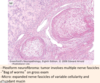
Cysticercosis / Toxoplasmosis / Amoebiasis all can cause Amoebiasis CNS infections
What 3 organisms are associated with Amoebiasis?
- [Naegleria Fowleri Free living Amoeba] –> [Fulminant Acute Meningoencephalitis]
* Image shows Trophozoites of Naegleria Fowleri* - Entamoeba Histolytica
- Balamuthia Mandrillaris

Viral Encephalitis
A: Major pathogens of [Summer/Early Fall] (3)
B: [Fall and Winter]
C: [Winter and Spring]
D: [Any Season] (5)
A: Summer/Early Fall = Arboviruses (West Nile Virus) vs. Enterovirus vs. Rocky Mountain(mimics viral encephalitis)
B: [Fall and Winter] = LCMV (Lymphocytic Choriomeningitis Virus)
C: [Winter and Spring] = Mumps
D: [Any Season] = HSV1/ EBV / CMV / Mycoplasma / Leptospira

Viral Encephalitis
A: Affects White or Grey Matter?
B: Histology (4)
A: Affects more Grey Matter (diffuse vs. focal)
B:
1) [Perivascular Lymphocytic inflammation]
2) [Leptomeningeal Lymphocytic inflammation]
3) [Microglial cluster nodules]
4) Neuronophagia
A: Polio Encephalitis MOD
B: Dx
C: Which pathogen can this be confused with?
D: Clinical Presentation
A: [Fecal-Oral transmitted] virus that replicates in [oropharynx & small intestine] & ultimately–> [ANT horn LMN destruction in brainstem/spinal cord]
B: Recovered from stool or throat
C: Can mimic [West Nile ArboVirus] & vice versa
D: [Asymmetrical LMN signs = Asymmetrical FAW = Fasciculations/[Atrophy & areflexia] / Weakness]

A: Describe MOD for Rabies and what virus causes it
B: Incubation period?
Rhabdovirus

A: Rabies= Exposure to rapid dogs (also bat/raccoon/skunk) —> [Prodrome of flu-like sx] + [Negri body cytoplasmic inclusions] seen in brainstem/hippocampus/[Cerebellar Purkinje cells]
B: [10 days to a year] depending on bite location
A: Herpes Encephalitis MOD
B: Where does this Virus remain Latent?
C: Histology
D: What does the [Burnt Out Herpes Encephalitis] refer to?
E: Tx
Most commonly recognized and devastating

A: HSV1 (transmitted via saliva) –> [(Hemorrhage—>Cavitation & Atrophy) / Acute Necrosis/ Edema] of [Medial Temporal & Frontal lobe]
B: Trigemial ganglion
C: [Owl’s Eye Intranuclear inclusion]
D: Chronic Phase= Cavitation and Atrophy with shrivelled/brown color in long term survivors
E: Acyclovir (should be started even if suspected)
A: CMV MOD
B: Demographic (2)
B2: Describe the Clinical Manifestation for each Demographic
C: General Microscopy (2)
A: Opportunistic Virus (Especially in AIDS and neonate pts) that is is part of TORCH (Toxo/Others/Rubella/CMV/Herpes)
B: AIDS and neonate pts
B1) Adults = Dilated CSF Ventricles and calcifications within periventricular region
B2) Postnatal infection = [multiple microglial nodules] + [occasional cytomegalic cellular inclusions]
C:
- Meningoencephalitis
- [Cytomegalic cellular inclusions] mostly in periventricular regions


[loss of myelin] and Atypical Astrocytes consistent with
PML-Progressive Multifocal Leukoencephalopathy
HIVE
HIV Encephalopathy
B: Describe 2 other neuro conditions associated with HIV
C: What Dx should you suspect in a Young HIV Pt witih Dementia? Pgn?
Widespread [microglial nodule GREY MATTER ENCEPHALITIS] —> [multinucleated giant cells]
*Also causes (Meningitis–>Persistent Pleocytosis & neuro sx) and Dementia via Direct Viral invasion vs. inDirect inflammation
C: AIDS Dementia= slow cognitive & behavioral decline with poor pgn. Note: This presentation is Similar to [SubAcute Combined Degeneration]
HIV LeukoEncephalopathy is the same thing but with White matter instead

HIV LeukoEncephalopathy
A: clinical presentation
B: Histology
C: Which brain cells are NOT affected by this?
A: Subacute onset with cognitive impairment and apathy
B: [Diffuse WHITE MATTER myelin pallor with microglial nodules and (multinucleated giant cells)
C: Oligodendrocytes are NOT infected
Unknown Etiology
Vacuolar Myelopathy

Spastic Paraparesis with hyperreflexia and ataxia caused by vacuolation of [Spinal Cord White Matter]
Brain Abscess
A: Solitary or Multifocal
B: Cause and [Dx method (3)]
C: Tx (2)
D: How are Brain Abscess related to CA
A: Usually Solitary (can be multifocal) within epidural or subdural of brain/spinal cord–> 20% Mortality
B: Caused by CNS infection that has to be indentified with [biopsy vs. aspiration vs. CT/MRI]. (LUMBAR PUNCTURE MAY CAUSE HERNIATION. Only use if concurrent with meningitis or ventriculitis)
C: Surgical Excision vs. Abx
D: Multiple Abscess can mimic [Metastatic CA]

Brain Abscess
A: Causes (4)
B: Common locations (2)
A:
1) Direct infection from elsewhere (otitis/sinusitis/dental/cellulitis): {also mechanism for Bacterial Meningitis}
2) Hematogenous from distant infectious site (Endocarditis/Osteomyelitis/Lung): {also mechanism for Bacterial Meningitis}
3) [Trauma vs. surgery] Direct organism introduction
4) [DM / EtOH]
B:
- [Grey-White Junction]
- [White Mater where collateral circulation is poor]

Brain Abscess
Describe the Evolution of Brain Abscess
1st: Early Cerebritis-granulation & early fibrous capsule formation (Day 1-3 )
2nd: Confluent Necrosis (Day 2-7 )
3rd: Early Encapsulation (Day 5-14 )
4th: Late Encapsulation ( > 2 weeks )

A: How do Adults acquire and present after Lead Poisoning?
A: How do Children acquire and present after Lead Poisoning?
A:
Adults: [Workplace paint vs. lead battery] –> Peripheral neuropathy
B: Children: [ingeting lead paint flakes] –> [Encephalopathy + Abd pain]
C:
-[Chemical Plant vs. Glue sniffing] –> [Peripheral neuropathy] or [Encephalopathy]. Dx is clinical
Bacteria Meningitis
A: Complications (4)
A:
1) Hydrocephalus (from pus obstructing CSF pathway)
2) 2º inflammation and edema of Cortex = meningoencephalitis
3) Thrombosis of inflamed superficial cortex vessels & spinal cord –> Infarct
4) deafness (espeically in children)
Encephalitits
A: General Sx (4)
B: Onset time
C: Tx (2)
A: [Focal Edema] —>
- [Change in Behavior/Consciousness (specific for Encephalitis)]
- High Fever
- HA
- [Seizures & Focal Neuro Deficits]
B: Hours to Days
C: [[IV Dexamethasone] vs. Sedatives] (For INC ICP and seizures)

West Nile Arbovirus Encephalitis
B: MOD
C: Which animal was subject to the West Nile Arbovirus prior to humans?
D: Which other pathogen can this be confused with?
West Nile Arbovirus
B: Affects Peripheral n. vs. [ANT Horn Cells] (similar to Polio virus) –> Weakness and Encephalitis
C: Birds
D: Polio Virus
A: Prion Dz MOD (2)
B: What is the Prion Dz manifestation in animals called?
C: What is the Prion Dz manifestation in HUMANS called? Describe the Clinical Presentation (2)
A: [Infectious Proteins! from human graft tissue or dirty neurosurgical instruments] induce conformational change in [normal neuronal proteins]–> neuronal death without inflammation –> [transmissible spongiform encephalopathies]. Also can be Hereditary.
B: Mad Cow Dz in Cows!
C: [CJD- Creutzfeldt Jakob Dementia] In Humans
*Rapidly progressive dementia with [prominent myoclonus] + [CST vs. extraCST vs. Cerebellar vs. LMN signs]–> Fatal in Weeks-Months!
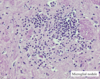
spongiform encephalopathy shown in image

A: Identify and Describe pathology shown below
B: Cause

OPTIC ATROPHY

A: [Pale Optic Disc with Sharp Distinct Margins] associated with residual [scotoma blindspot] or [loss of acuity]
B: Occurs weeks after Optic N. Lesion, which destroys [Retinal ganglion axons]–> OPTIC ATROPHY
A: Identify and Describe pathology shown in image
B: Cause and PGN
C: Which eye does this typically occur in?

A. Papilledema = [Bilateral Swollen Discs] with vessels mound over blurred Optic Disc margins.
B: Results from INC ICP –> normal vision initially but will impair vision if untreated
C: BILATERAL

A: Clinical Course (Visual manifestations) for Pituitary Tumor (2)
B: What other sx is typically associated
C: Pituitary Tumor MOD
1st: [BiTemporal Upper Quadrantanopia] (since compression starts from below initially) –>
2nd: [BiTemporal Heteronymous Hemianopsia]
B: Hormonal Dysfunction
C: Arises within [Sella Turcica] and compresses Optic Chiasm from below at first –> entire thing

A: Describe the difference between Sensorineural and Conductive Deafness
B: List causes for Sensorineural (4) and Conductive (2) Deafness
A:
-Sensorineural Deafness = [HIGH tone loss] from [Hair cells vs. Auditory n.] degeneration (causes: loud noise / drugs / ischemia / Trauma)
vs.
-Conductive Deafness = [Low tone loss] from impaired air conduction (causes: wax / ossicle lesion)
A: Benign Positional Vertigo MOD
A2: Clinical Presentation
B: Demographic
C: Tx (2)
A: [Degenerated Ca+ Crystals Otoliths] lodge around cilia of [semicircular canal hair cells] –> oversensitivity.
A2: Minor mvmnts of head (getting out bed vs. bending over) –> vestibular impulses–> [Benign Positional Vertigo]
B: Elderly
C:
1) Intermittent Benzodiazepine vs. Antihistamine
2) Head-positioning exercises

Acute Labyrinthitis also COMMONLY causes Vertigo
A. Causes (2)
B. Clinical Manifestation (5)
C: Tx (3)
Acute Labyrinthitis also COMMONLY causes Vertigo.

A. Viral Infection vs. [Inflammation of inner ear labyrinth] both resolving in days to weeks.
B: [Vertigo / NV / (Unilateral Deafness) / Gait ataxia / (Asymetrical Nystagmus)]
C:
- Benzodiazepine
- Antihistamine
- Antiemetic
Meniere’s Dz
A. Sx (3)
B. MOD
C. Complication
Meniere’s Dz= [Recurrent Vertigo] + tinnitus + deafness
B. [membranous labyrinth rupture –> intermixing of Endolymph and Perilymph –> loss of ionic gradient within semicircular canals. This causes Degeneration of vestibular & cochlear hair cells could–> Permanent Deafness
C: Permanent Deafness

A: MRI is best used for what (2)
B: Cons (4)
C: Contrast agent used
D: Brief MOA
A: Multiple Views (axial vs. sagittal vs. coronal) of Brain and Spinal Cord with no radiation
B: Longer scanning time / [images degraded by pt mvmnt] / [contraindicated with pacemakers or certain metal] / [Tight Enclosed space]
C: Gadolinium
D: [Spinning protons in water of living tissue] act as small magnets and are affected by [External Magnetic fields] induced by MRI. Serial RadioFrequencies from excited tissue generate the MRI image.
CT scan
A: Which views can be seen and how is this disadvantageous
B: How long is the scan
C: Contrast agent used
D: Cons (2)
A: Axial views (CT requires image reformatting for other views). All Axial views are computed –>Composite scan.
B: Shorter scanning time
C: Iodine-based
D:
- Radiation (Multiple X-ray images are taken as X-ray tube rotates in circular path around brain/spinal cord)
- requires image reformatting for other views

MRI
A1: T1W. Highlights _____. [CSF is ___ in color with ___ signal]
A1: T2W. Highlights _____. [CSF is ___ in color with ___ signal]
B: What is FLAIR?
C: Lesions appear _____[dark vs. bright] on T2W and FLAIR
MRI
A1: T1-Weighted = Highlights Anatomy. [CSF isDarkwith low signal] (Ais1st letter)
A2: T2-Weighted = Highlights PATHOLOGY. [CSF is WHITE with HIGH signal]
B: FLAIR = FLuid AttenuatIon Recovery: Similar to T2W but [visually distracting HIGH signal from CSF] is removed :-)
(Most lesions appear _BRIGHT_* *onT2WorFLAIR**. Lesions appear Dark on CT )
A: Which Radiographic Scan should be used for Acute Hemorrhage
B: Describe the Clinical Course of Acute Hemorrhage with this Scan (3)
C: Why does this change in Clinical Course occur?
A. CT scan
B. Radiographic course of Acute Hemorrhage([SubDural Outside] vs. [SAH inside])
1st: HYPERdense (Very White) = Acute
2nd: Isodense as time passes and edema subsides = SubAcute
3rd: hypOdense (very dark) on CT = Chronic
C: Hemorrhage density changes as iron content of Hematoma changes from HgB–>[met-HgB]__–>hemosiderin
A: Which Radiographic scan is best for Acute Infarction? Why?
B: Lesions appear ____ or ____ in color on CT
B2: What are 2 reasons why CT is not efficient for Acute Infarction
A: [MRI-Diffusion Weighted Imaging]
A2: Water diffusion is impaired in ischemic brain = best scan for earliest infarct detection
B: Lesions appear [**Dark-low signal] or [Lucent if in vascular area] on CT.
B2:
- Early infarcts may NOT be visibleor show subtle effacement
- Small lacunar infarcts may NOT be detected at all!
A: Contrast function (2)
B: What does Contrast enhance (2)
A Delineate [Tumor or Abscess] amidst surrounding edema.
B: Contrast Enhances [lesions with leaky blood brain barrier] and Normal Vascular Structures
C: Edema mainly involves ____ matter and spares _____
How does Edema appear on CT (2) as compared to [MRI T2W / FLAIR]
C: Edema mainly involves White matter and spares [cortical gyri fingers]: It appears…
CT= [hypOdense dark-low signal] vs. [lucent when in vascular areas]
[MRI T2W / FLAIR]= HYPERdense-High signal
A: Describe Hydrocephalus
B: List the Causes and which structures are affected in each Cause (2)
A: Ventricular enlargement without loss of brain tissue related to impaired CSF flow
B:
1) Aqueductal Stenosis –> [ONLY 3rd Vt enlargement]
2) [Blockage/Scarring of SubArachnoid Vili] –> [3rd AND 4th Vt enlargement]
Describe these Brain Tumor Processes
A: [Primary Brain Tumor] (3)
B: [Metastatic Brain Tumor] (3)
C: [Epidural Spinal Cord Metastasis]
A: “HIS primaries were tumor-like!”
[Solitary / [Irregularly shape] / [Hemorrhagic vs. heterogenous]
B: M for MSG
Metastatic= [( Multiple OR Solitary) / Spherical / [Gray-white junction]
C: Arises from [vertebral body] and encroaches upon spinal cord
Spondylosis: Degenerative Spine Dz
A: MOD
B: Radiographic scan used for Dx (2)

A: [Herniated Disc–>Torn Annulus and then eventually–>Toothpaste sign / [Elevated ligaments] and [Spinal Cord Stenosis]
B:
1st line: MRI:T2W
2nd choice: [Spinal CT that may require [intrathecal myelogram contrast] (outlines spinal cord and n.roots)]
Thecal Sac contains SubArachnoid Space
Image below shows

A: 5 major UMN signs
B: Asymmetrical Reflexes are ____ (normal vs. abnormal)
C: Major causes of Altered Mental System (2)
A: Weak MESH
- Weakness
- Spasticity
- [Exaggerated Reflexes (Babinski)]
- Mental Status change
- Hemiplegia
B: Asymmetric Reflexes = ALWAYS ABNORMAL
C: (can come from Intracranial Pressure changes)
1) Bilateral Hemisphere damage
2) Damage to RAS - Reticular Activating System
A: Compare the Pupil response differences between Compression and Ischemia of [Oculomotor CN3]
A:
- Compression of [Oculomotor CN3] –> Pupil DILATION (since Parasympathetic fibers are outside the [Oculomotor CN3 nerve fiber]
- -*Ischemia of [Oculomotor CN3] –> Pupil Stasis
Define the 3 Functional Groups of the Thalamus
A- [Specific Relay nuclei]= bidirectional inputs & projections to SPECIFIC motor/sensory Cortex
B- [Association nuclei]= bidirectional connections to association areas of Cortex & subcortical structures
C- [Non-specific nuclei]= NON POINT-TO-POINT connections in intralaminar & midline that “awaken/prepare” cortex for receipt
B: Specific inputs to the Thalamus use ____ as a NTS
C: What’s Internal Capsule Blood Supply? (3)
D: Internal Capsule Function
A: **PCA**
Postetrior Cerebral A.
——————————————————————————
B: Specific inputs to the Thalamus use GLUTAMATE as a NTS
C:
- *Internal Capsule** Blood Supply:
1. [lateral striate a.] from MCA
- [Recurrent a. of Heubner] from the ACA
- [ANT Choroidal a.]
D: Transmits [Cerebral Cortex [Forebrain/Brainstem/Spinal Cord]]

A: What Afferents travel TO the Thalamic [Thalamic RETICULAR nucleus] (2)
B: Where does the Efferent fibers of the Thalamic [Thalamic RETICULAR nucleus] project to?
C: What type of Thalamic nucleus is the [Thalamic RETICULAR nucleus]
D: What is Different of this Thalamic nucleus from the others?
[Thalamic RETICULAR nucleus]
A: Aff= Thalamus & Cortex—–> nc
B: Eff= nc—> ONLY other Thalamus nuclei
C: [Non-Specific nuclei]
D: Aside from this [Thalamic RETICULAR nucleus], All OTHER thalamic nuclei “decide” where info should go in Cerebral cortex
[SUP Cerebellar Peduncle] is the main ______[input/Output] pathway for the Cerebellum
[SUP Cerebellar Peduncle] is the main OUTPUT pathway for the Cerebellum
A: In what 2 instances do you see a POSITIVE Babinski Sign
B: Why is the interpeduncular Fossa significant? Where is it located?
POSITIVE Babinski Sign
- [UPPER Motor Neuron] damage –> {Weak MESH} sx
- infants
B: The interpeduncular Fossa is significant because [Oculomotor CN3] runs out of it. It is found in the MIDBRAIN between the 2 [Crus Cerebri Cerebral Peduncle}
- Which 2 tracts cross in Medulla?
- Sympathetics are found in the ____
- Medial and Lateral motor nuclei are related to the ____ Tract
- Which 2 tracts uses the [inferior Cerebellar peduncle] (ICP)?
- DSCT uses ___ Nucleus before going to _____
- ___, ____ and ____ tracts all cross in the Spinal Cord
- Medial Lemniscus uses the ____ _____ pathway
- Nucleus Proprius is related to the ___ ____ Tract
- CST and DCP = cross in Medulla
- Sympathetics are found in the [Lateral Horn/IML]
- Medial and Lateral motor nuclei are related to the CORTICOSPINAL TRACT (CST)
- DSCT & CCT use ICP [Remember: VSCT uses SCP]
- DSCT uses Clark’s Nucleus before going to ICP
- VSCT / [ANT CST]/ STT all cross in the Spinal Cord
- Medial Lemniscus uses the [Dorsal Column Pathway]
- Nucleus Proprius is related to the [Spinal Thalamic Tract]
A: Most common cause of Senile Dementia > 65 y/o
B: Describe the Genetic Associations with the Early onset type (3)
C: Describe the Genetic Associations with the LATE onset type (2)
A: Alzheimer’s Dz (Familial Auto Dominant type= early onset) vs. (Sporadic type= late onset)
B:
- [APP (Amyloid Precursor Transmembrane Protein) - Chromosome 21: Down Syndrome] - APP undergoes many proteolytic cleavages
- [Presenilin 1 Chromo 14]
- [Presenilin 2 Chromo 1]
C:
*[ApoE4 Chromo 19]
*[ApoE2: Protective]
Describe Gross Histology for Alzheimer’s (4)
A: [Generalized Cerebral Atrophy (starts w/temporal)]–>
- [Gyri Narrowing]
- [Sulci Widening]
- [DEC Brain Weight]
- [Dilated Vt with Hippocampus Atrophy]

A: Describe microscopic Histology for Alzheimer’s (2)
B: Which Stain is used to identify these changes (2)
A:
- [Intracell Neurofibrillary Tangles] = Intracell filamentous inclusions made of [Hyperphosphorylated Tau Protein] = [insoluble axon microtubule protein]
- [Extracell Amyloid Plaques] - [Found in Subarachnoid space & superficial cortex]. Also found in senile plaques.
B: Use [Bielschowsky Silver Stain] and H&E to identify.
Image shows [Intracell Neurofibrillary Tangles**]

CNS Tumor
A: Location: Adult vs. Children
B: Why are Benign Lesions still a problem in the CNS
C: Describe CNS Tumor Metastasis
A: [Adult CNS Tumor = supratentorial] vs. [Child CNS Tumor = infratentorial]]
B: Benign lesions can have FATAL outcomes from location alone! [Note: Malignant vs. Benign is harder to differentiate in CNS]
C: Although [1° CNS Tumor metastasis] to other places is rare… [SubArachnoid space] may allow spread –> [Medulloblastoma]. (2° CNS Tumors ARE MORE COMMON & come from metastatic spread TO brain FROM other places using via blood)
A: Cause of Death from CNS Tumors (2)
B: What happens to infants who have CNS Tumors
C: General Sx for CNS Tumors (4)
A: [Internal Herniation] and [Compression of vital centers (Medullary Cardiopulmonary Center)]
B: Head enlarges –> Fontanelles bulges –> Head Circumference INC
C: [HA / NV / Neuro deficits/ Seizures (superficial tumors)] from INC ICP
A: Most common [1º CNS Tumors] in Adults (3)
B: Most common [1º CNS Tumors] in Peds (3)
C: Which [1º CNS Tumor] is the MOST Malignant Astrocytoma?
A: GMS: [Glioblastoma (Grade 4)] / Meningioma / Schwannoma]
B: PEDs
- [Pilocytic Astrocytoma (Grade 1)]
- Ependymoma
- MeDulloblastoma
C: [Glioblastoma (Grade 4)]
A: Describe Astrocytoma
A: Astrocytoma is the most common glioma and so can occur anywhere in brain and to any age
The WHO has assigned 4 Grades of Histology for CNS Tumors
GRADE 1
A: Pgn
B1: Example
B2: Where is this Example located in the CNS (2)
B3: Radiographic description of Example
B4: Histology of Example (2)
A: [Low proliferative potential and slow growth] = Least malignant and can undergo [surgical resective cure]
B: Pilocytic Astrocytoma (common in PEDs)
B2: Cerebellum and Brainstem
B3: [Cyst with mural nodule]
B4:
- Rosenthal Fibers
- [Piloid cells with Hairlike processes]

The WHO has assigned 4 Grades of Histology for CNS Tumors
Decsribe GRADE 2 (3)
- [No mitosis / necrosis / vascular proliferation]
- [Infiltrative nature]
- [low level proliferative activity often recurs]
The WHO has assigned 4 Grades of Histology for CNS Tumors
A: Decsribe GRADE 3
B: Tx
- [Malignant tumor without microvascular proliferation/necrosis]
B: Radiation/Chemo
The WHO has assigned 4 Grades of Histology for CNS Tumors
GRADE 4
A: Example and Pgn
B: Name the 4 Sub-Grades
A: GLIOBLASTOMA = MOST MALIGNANT ASTROCYTOMA = POOR PGN!
B: image

Glioblastoma
A: Statistics
B: Location
C: Radiographic findings (2)
D: Histology (5)
E: Tumor marker

A: Most common [1° Malignant CNS Tumor] in Adults
B: Cerebral Hemispheres but may be multicentric (Diffusely infiltrating)
C: [[May cross Corpus Callosum] –> [MRI Butterfly lesion]] + [Midline shift from lateral vt compression]
D: CREEPY
- Yellow necrosis
- Reddish brown hemorrhage
- Cystic Change
- Pseudopalisading Necrosis on Histo
- Endothelial Cell Hyperplasia on Histo
E: GFAP positive

OligoDendroglioma
A: Pgn
B: Location
C: Radiographic Findings
D: Histology (3)
A: Better pgn than Astrocytoma of a similar grade
B: Most frequent Frontal lobe
C: [CT Intratumoral Calcifications]
D: “Oli -goes to store to get fried eggs to eat Chicken out of his Front house Satellite dish”
*[Perinuclear halos - “fried egg” appearance]
*[Chicken Wire Capillary pattern]
*[Satellitosis in 2° structures]

A: Describe Rosettes
B: Where are the nuclei for these located?
A: [Spoke-wheel arrangement of cells around central core which may be empty or filled w/cytoplasm. Cytoplasm is wedge shaped & directed toward core] resembles rose windows
B: peripherally positioned and form a ring around the hub
A: Identify
B: Describe the core of this structure

A: [MHW- MeDulloblastoma Homer Wright Rosette]
B: [delicate neuropil fibrils]
” M for Meaty Core!”
A: Identify
B: Describe the core of this structure

A: [RFW-Retinoblastoma Flexner Wintersteiner Rosette]
B: EMPTY
A: Identify
B: Describe the core of this structure
C: Name and describe the counterpart to this structure

A: [Ependymoma Perivascular Pseudorosette] vs.
B: Halo of tumor cells around blood vessel
C: [EpendymomaTRUE rosette] is shown in image below = [Halo of tumor cells around EMPTY blood vessel]

Ependymoma
A: Demographic
B: Location (2)
C: What structures are lined by Ependymal cells (2)
A: Any age but most frequent in kids
B: [4th Ventricle which may–> Hydrocephalus] vs. [Spinal in adults]
B: Ventricles and [Spinal Cord Central Canal]

Medulloblastoma
A: Where does it arise from
B: Location: Children vs. Adults
C: Tx
D: Histology
MeDulloblastoma / MHW

A: [Undifferentiated NeuroEctodermal cells]
B: [Children: Cerebellum/4th ventricle] vs. [Adults: Hemispheric]
C: Radiation tx sensitive :-)
D: [small blue cell tumor] composed of [Undifferentiated cell sheets] with scanty cytoplasm and dark nuclei
MeninGioma
A: Arises from what cells
B: Demographic
C: Location (2)
D: Sx (2)
E: Tx
“Men in Gio:”
A: Arachnoid Meninges
B: [Benign tumor of mid-aged Females]
C: [ExtraAxial = Outside Brain Parenchyma - common in convexities and parasagittal regions]
D:
- MOSTLY ASX
- [possible seizures/focal neuro deficits depending on location]
E: [Resection +/- radiation]

Name the 4 characteristics of MeninGioma
” Men in Gio sat in PEWS”
- Psammoma body laminated calcifications
- Whorls
- Syncytial Appearance
- [Elongated cells with collagen deposition]

Craniopharyngioma
A: Demographic
B: What is this CNS Tumor often confused with? What are the sx (4)?
C: What cells does it arise from?
D: Histology
A: [Benign Childhood tumor]
B: [Pituitary Adenoma!] since it causes:
- Endocrine dysfunction
- Visual sx
- Hydrocephalus
- Calcifications
C: Rathke’s Cleft (Rathke’s pouch remnants) —> [Rathke’s Cleft Cyst]
D: Wet Keratin contained in complex epithelium

A1: Identify
A2: Malignant or Benign?
B: Location (2)
C: Sx (2)
D: Which associated dz has [Bilateral Acoustic Neuromas]?
E: Which Stain is used for dx

A1: Schwannoma
A2: Benign (involves cranial OR spinal nerves)
B: [CerebelloPontine Angle] and [Vestibulocochlear CN8 = Acoustic Neuroma]
C: [(Loss of Hearing) + Tinnitus]
D: [Neurofibromatosis Type 2]
E: S100 protein
A: [2° CNS Metastatic Brain Tumors] come from which organs mostly? (5)
B: Which of these organs –> Hemorrhagic Metastases (3)
C: Characterization of [2° CNS Metastatic Brain Tumors] (3)
A: Lung > Breast > melanoma > kidney > GI
B:
- Lung
- Breast
- kidney
C: MSG - [Multi vs. single] / Spherical / [Gray White Jxn]

Neurofibromatosis Type 1
A: Genetic Cause
B: Characteristics (6)
C: Which characteristic is Pathognomonic of NF1
D: Pgn

A: [17q11 mutation]–> [Neurofibromin-GTPase activating protein] dysfunction
B: “CLAP ON type 1!”
- Neurofibroma
- Acoustic Schwannoma
- [Optic n. Glioma]
- Lisch nodules
- [Cafe Au Lait Spots]
- [Plexiform Neurofibroma]
C: Plexiform Neurofibroma
D: HIGH chance of Malignancy

Neurofibromatosis Type 2
A: Genetic Cause
B: Clinical Manifestation (2)

A: [22q12 mutation of a tumor suppresor gene–> (Merlin cytoskeletal protein)]
B:
- [Bilateral Acoustic Schwannomas]
- Multiple Meningiomas
Tuberous Sclerosis
A: Genetic Cause and Manifestation
B1: Sx (5)
B2: Which are the triad?

A: ([Hamartin C1 9q] and [Tuberin C2 16p])–> [Cortical & Subependymal Hamartomatous lesions] such as [SEGA-SubEpendymal Giantcell Astrocytoma] which may –> hydrocephalus
B: SAM ASh
- Adenoma Sebaceum (Facial angiofibroma) = triad sx
- Seizures = triad sx
- Mental Retardation = triad sx
- [Ash Leaf hypOmelanotic macules]
- [SHagreen forehead patches]
(Note: TS affects multiple organs)
Front image: Red = Tubers /// Blue = SEGA nodules

Von Hippel Landau Dz
A: Genetic Cause
B: How does it manifest in the CNS

A: [Tumor cells lose [Chromo 3 VHL Tumor suppressor gene] –> [INC VEGF from Hypoxia Inducible Factor]
B: [CNS Cerebellar Hemangioblatoma]

A: Define Seizure
B: How is it associated with LOC? How is it associated with Epilepsy?
C: What 2 Neuron Types are responsible for the MOD in Seizure
D: Demographic (2)
A: Clinical Event consisting of Paroxysmal episodes of [excessive neuronal discharge] that manifest physically based on area of brain affected.
B: NOT always associated with LOC and is NOT the same as epilepsy
C:
-[INC excitatory NMDA Glutamate (propagates seizure)] + [DEC inhibitory GABA (terminates seizure)]
D: [Neonates/Kids] & [Older Adults] = Bimodal
A: Define Epilepsy
B: Is it provoked by anything?
A: Syndrome that includes Recurrent Seizures, in the absence of an extra-cerebral cause
B: NOT directly provoked by infection/drug withdrawal/metabolics/fever
Seizures can be grouped into Classifications:
A: Describe Partial Seizure Types (3)
B: What’s a good way to differentiate between pts with Seizure vs. Syncope
- Simple Partial= Focal onset but with NO change in consciousness
- Complex Partial= Focal onset with impaired consciousness
- [Grand Mal Tonic-Clonic Seizures] = Generalized onset that –> Bilateral convulsive seizure
B:
*pt last memory is waking up on floor = syncope
*pt last memory is ambulance/ER = seizure
Partial Seizures: Temporal lobe
Clinical Presentation (3)
- Epigastric Aura (fear / deja vu / olfactory & gustatory sensation)
- [Unresponsive Staring]
- CTL Limb posturing
* TEMPORAL LOBE IS MOST COMMON LOCATION*

Partial Seizures: Frontal lobe
Clinical Presentation (4)
” I NV JC for being in Front”
- Night onset
- Versive mvmnt (pt Frontal Eye fields turns their head & eyes away from the seizure location)
- [Jacksonian March + (Post-ictal Todd’s Paralysis)]
-
Complex mvmnts (bicycling/fencing)
* TEMPORAL LOBE IS MOST COMMON LOCATION*

A: Partial Seizures: Parietal lobe Clinical Presentation (2)
B: Partial Seizures: Occipital lobe Clinical Presentation
A: Uncommon seizures manifesting as [Lip/Finger/Toe] paresthesia + visual hallucinations
B: [Darkness with RED Light flashes] (easily confused with migraines)
Absence Seizures
A: Demographic
B: Clinical Manifestation
C: Dx
D: Tx
A: [4-10 y/o]
B: Brief ( < 10 seconds) but frequent ( >10/day) [unresponsive staring spells]
C: EEG with 3 Hz spike-and-wave pattern
Young child who does poorly in school and noted to be frequently staring off into space = Typical Presentation
D:
- ethoSUXimide (Silent seizures SUX)
- [AED Peds Tx] ONLY when benefits outweigh Side Effects from a 2nd seizure. “1st seizure is for free = no tx”
Myoclonic Seizures
A: Demographic
B: Clinical Manifestation
C: Precipitants (2)
D: Tx (2)
A: Teenagers (occurs in morning after waking up)
B: Myoclonic jerks (shock-like contractions of muscle groups)
C: [Alcohol vs. Sleep Deprivation]
D:
- Valproic Acid
- [AED Peds Tx] ONLY when benefits outweigh Side Effects from a 2nd seizure. “1st seizure is for free = no tx”
Atonic Seizures
A: Clinical Manifestation (2)
B: Body parts involved (2)
C: Tx
A: [Sudden loss of tone] + [brief LOC]
B: [Focal (Head Drop) or ALL MUSCLES]
D: Tx resistant :-(
[Grand Mal Tonic-Clonic Seizures]
A: Describe
B: Clinical Presentation (4)
A: Classic Seizure referred to as Grand Mal
- Tonic: extension & arching
- Clonic: Alternating contraction & relaxation
B: “FIME sounds Sublime and Grand!”
- [Flexion of trunk IMPROMPTLY]
- [Mouth opening]
- [Eye deviation upward]
- [Ictal cry at onset and post-ictal confusion]
PseudoSeizures
A: Description
B: What Clues may Hint you to this Dx vs. True Seizures? (4)
A: [NON-EPILEPTIC Seizures, psychiatric in nature but tht can occur in pts with true epilepsy
B: Pt exhibits….
- Pelvic Thrusting
- Absent [post-ictal confusion]
- [To-and-From movements and INC Respiratory Rate]
- Elevated serum prolactin 10-20 min post event
- TYPICALLY DX OF EXCLUSION*
Seizures
Dx (4)
- EEG (brain wave test)
- [CT / MRI]
- Labs (glucose / electrolytes / prolactin / CBC)
- Spinal Tap (if concerned for infection)
FEBRILE Seizure
A: MOD
B: Characteristics of Seizure (Location/Freq./Duration)
C: Demographic
D: Pgn (4)
E: Tx
A: Pace of Temperature development (Fever > 38.4 C)–> [Simple Febrile Seizure]
B:
- [Generalized & non-focal]
- Freq. = [less than 2/ day]
- Duration= [less than 15 min. episodes]
C: [3 months - 5 y/o (most before age 3)]
D: Typically outgrown BUT does INC risk for Adult Epilepsy if at least 2 factors are present:
[Fam Hx of non-febrile seizures] / [Abnormal neuro exam] / [Focal seizures +/- Todd’s paralysis] / Prolonged seizures
E: DO NOT NEED TO TREAT but can give [Rectal Diazepam]
STATUS EPILEPTICUS
A: CLINICAL PRESENTATION
B: CAUSES (2)
C: EVALUATION OF THE PT (4)
NEUROLOGICAL EMERGENCY!
A: Continuous Seizure (>5 min) that has long term consequences if > 30 min. Pt fails to regain consciousness in between episodes!
B:
- Med Non-compliance
- New-onset from [infection/trauma/SAH/Drugs/stroke]
C: AGLI the pt!
1st: ABC (Airway / Breathing / Circulation)
2nd: Check Blood Glucose and give Thiamine
3rd: IV [Lorazepam & then–> Phenytoin]
4th: ICU admission for propofol vs. [IV midazolam]
* DO NOT STICK THINGS IN [STATUS EPILEPTICUS PT] MOUTH!*
Describe the Treatment Approach for Seizures

Delirium
A: General Definition
B: Cause
C: Clinical Presentation (3)
A: Abrupt Acute Confusional state which alternates between agitation & obtundation.
B: CNS damage (Direct vs. Indirect)
C:
- [fluctuating attention and consciousness]
- memory/mood/language impairment]
- [Tremors/Dysarthria/Myoclonus]
Alzheimer’s Dz
Tx (2)
No Curative Tx!
- Acetylcholinesterase inhibitors (Donepezil / Rivastigmine / Galantamine)
- Memantine (Aspartate Blocker)
