Neuropathology 1 Flashcards
1) The Fasciculus Gracilis exist at _______of spinal cord and DOES contain ______ ____ from the ___
vs.
Fasciculus Cuneatus exist in {__-__} = ____ and ______ and contains _____ ____ from the ___
1B) Which Pathway are these Fasciculus columns associated with?
2) What happens to 2nd order neurons of this Pathway?
2B) Where are these 2nd order neurons located?
3) What happens to 3rd Order neurons of this Pathway?
4) How does [Proprioreception/Vibration/2-point discrimination] get to 2nd order neurons? [5]
**Position/Vibration/2-point discrimination travels from periphery in the ______ ______—–> passes ______—>passes ______ ______ Gray mater–>ultimately travels upwards using ______ ______ or ______ ______
—>travel up into [______ MEDULLA] to synapse 1st time in ______ ______ or ______ ______
1) The Fasciculus Gracilis exist at ALL LEVELS of spinal cord and DOES contain [ascending sensory fibers] from the LE
vs.
Fasciculus Cuneatus only exist in {C1-T6} = Thoracic segments (T1-T6) and Cervical segments (C1-C8) and contains [ascending sensory fibers] from UE
**DORSAL COLUMN PATHWAY**
2) 2nd order neurons in [nucleus gracilis] AND [nucleus cuneatus] decussate as [internal arcuate fibers] in LOWER MEDULLA—>cross midline to form [Medial Lemniscus]—>this travels to VPL nucleus of thalamus!
3) 3rd order neurons in [VPL nucleus of thalamus] travel in internal capsule and terminate in [Area 312 POSTcentral gyrus]
4) Position/Vibration/2-point discrimination travels from periphery in [Dorsal Root]—> passes DRG—>passes Dorsal Horn Gray mater–>bends in {Fasciculus cuneatus or gracilis}—>travel up into [LOWER MEDULLA] to synapse 1st time in {nucleus cuneatus or gracilis}
A) [Lateral Dorsal Root] Synapses in ____ _____ of ____ Horn and then becomes the _____ ______ . What sensations is this transmitting? [2]
B) SPINOTHALAMIC TRACT DECUSATES in _____ _______ and BEGINS ASCENT in the __________
—->It then travels ultimately travel up to [VPL nucleus of Thalamus] via the _____ _____ of spinal cord
C) Cutting STT in CORD will affect Pain on ____[same/Opposite] side of Body
A) [Lateral Dorsal Root] Synapses in Nucleus Proprius of [Gray Dorsal Lateral Horn] to become SPINOTHALAMIC TRACT= USED FOR PAIN and TEMPERATURE OF THE BODY
B) SPINOTHALAMIC TRACT DECUSATES in [ANT Commissure of Spinal Cord] and begins ascent in the [white Anterolateral Fasciculi] —->STT then ultimately travels up to [VPL nucleus of Thalamus] via [LATERAL FUNICULUS] of spinal cord
C) Cutting STT in CORD will affect Pain on OPPOSITE of Body

A: [Dorsal Spinocerebellar tracts] travel in ____ ______ and synapse either on _____(below C8) OR _____(Above C8). This tract is used for ____ ______ ______
B: Muscle Spindles use Sensory Affarent fibers (which bend in the [Fasciculus ______]) and transmit __ ______ ______ to the [____ _____ _____ nucleus] located in ___ ______
C: What is the [cuneocerebellar tract] ?
**A tract that receives ______ info from ______ nucleus & then ______[contralaterally/Ipsilaterally] sends this to the __ ___ ____ which relays info to ______ ______
D: [Dorsal Spinocerebellar tracts] AND [cuneocerebellar tract] use the__ ___ ____ to enter Cerebellum Vermis
A: [Dorsal Spinocerebellar tracts] travel in LATERAL FUNICULUS and synapse either on [Dorsalis Nucleus of Clarke] (below C8) OR lateral accessory cuneate nucleus for UNCONSCIOUS IPSILATERAL PROPRIORECEPTION
B: Muscle Spindles use Sensory Affarent fibers to bend in the [Fasciculus CUNEATUS] and transmit UE unconscious positioning to the LACN [lateral accessory cuneate nucleus] located in Lower Medulla.

C: [cuneocerebellar tract] = tract that receives UNCONSCIOUS positioning info from LACN [lateral accessory cuneate nucleus] & then ipsilaterally sends this to the ICP—> Cerebellum VERMIS
D: [Dorsal Spinocerebellar tracts] use the [inferior cerebellar Peduncle] to enter Cerebellum Vermis
A: How are the Bipolar Cells, Internueonrs & Ganglion cell bodies arranged near the Fovea? What about blood vessels?
B: How does Fovea and surrounding Macula receive metabolic supply?
C: Fovea is an _____[vascular/Avascular] retinal area with the ___[least/most] visual acuity. It has a __ ___ ____layer to prevent light barrier and is EXCLUSIVELY _____. There is a 1:1 ratio with [__:___] -which means ___ are more specific
D: Fovea is only __% of Retina and transmits __[least/most] of visual information to ________
A: Near Fovea, Bipolar Cells, Interneurons & Ganglion cell bodies are pushed LATERALLY–>makes a clear path for light = High visual acuity.
**Fovea is also Devoid of any blood vessels for same reason
B: Since Fovea is Devoid of any blood vessels, Fovea and surrounding Macula depend on diffusion from underlying choroid vessels for metabolic needs
C: The Fovea is an AVASCULAR retinal area with the MOST visual acuity. It has a laterally flat inner layer to prevent light barriers and is EXCLUSIVELY CONES. There is a 1:1 ratio with
[ganglion cell body: Cone receptor] –>Cones are more specific!
D: Fovea is only 5% of Retina but transmits MOST of visual information to [Lateral geniculate nucleus of thalamus]

A: What are the 7 Steps of Visual Pathway starting with light entering eye?
B: Light Entering Eye:
[TEMPORAL Field axons] pass _____ [crossed/uncrossed]
vs.
[nasal field axons] pass ____ [crossed/uncrossed], which means what for optic chiasm lesions?
A: Pathway of Visual Info from Retina [RN CT L DV]
“RN (use) CT (to) Learn Direct Vision”
1st: Light enters —> hits Retina
2nd: Travels in Optic N.
3rd: Optic Chiasm [Temporal Field Axons CROSS HERE]
4th: Optic Tract
5th: [Lateral Geniculate Nucleus of Thalamus]
6th: Optic RaDiations [Meyer’s Temporal Loop vs. Parietal direct path]
7th: [Area 17 -Calcarine Primary Visual cortex]
B: Light Entering Eye:
TEMPORAL Retina Fields pass CROSSED = [Temporal fields] decussaTe at Optic Chiasm
vs.
nasal retina fields pass UnCrossed @ Optic Chiasm = NOT AFFECTED BY Central OPTIC CHIASM LESIONS

A: [P-type] ganglion cell bodies are used by _____. [M-type ganglion cell bodies are used by ______.
B: Describe each of these
[2 each]
A: There are 2 MAJOR classes of [innermost ganglion cell bodies]
1. P-Type [USED BY CONES] “Pretty Colors”
ºsmall receptive fields –> BEST with [color/fine detail/high acuity]
ºtons of it near Fovea
- M-type[used by rods]
ºLARGE Bodies and many axons share 1 cell body –> LARGE Receptive fields
ºBEST with [rapidly transient adaptation] &response to mvmnt or large objects
A: Although Visual Perception begins in ______, collateral visual info enters ____ via Pretectal Area= for ___ _____ and _____ _____ for ________
B: Pretectal Area uses ___ nuclei of _____ for ___ _____ and projects both ipsilateral & contralateral via ____ _____
A: Although Perception of vision begins in [Area 17 CPVC-Calcarine Primary Visual Cortex] collateral visual info enters
- Brainstem via Pretectal Area=FOR PUPILLARY REFLEX and
- [SUP Colliculus]=For [head&eye movement]
B: Pretectal Area uses [Edinger-Westphal nuclei] of midbrain for PUPILLARY REFLEX and projects both ipsilateral & contralateral via POSTERIOR commissure
What would occur if there was a Lesion in …
1. R Optic N. —->
- *Optic Chiasm —–>
- R Optic Tract—>
- R [lower radiation meyer’s loop] –>
- R [Lateral Geniculate nucleus of thalamus]–>
- R [upper radiation fibers]
- R [Area 17 CPVC]
B: Which 2 lesions present the same Visual sx?
C: Which Visual Field Decussates at Optic Chiasm?
Lesion in … (using R side damage as example)
- R Optic N. —-> BLIND RIGHT EYE
- ——————————————————————————- - *Optic Chiasm —–> [Bitemproal Heteronymous hemianopsia] (both temporal fields knocked out) since Temporal fields decussaTe at Optic Chiasm
- ——————————————————————————- - R Optic Tract—>[CTL homonymous hemianopsia]
- ——————————————————————————- - R [lower radiation meyer’s loop] –> “Pie in the Sky Lesion’ = [CTL homonymous upper quadrantanopsia]
- ——————————————————————————- - R [Lateral Geniculate nucleus of thalamus]–>[CTL homonymous hemianopsia]
- ——————————————————————————- - R [upper radiation fibers]–>[CTL homonymous LOWER quadrantanopsia]
- ——————————————————————————- - R [Area 17 CPVC]–> [CTL homonymous hemianopsia with macular/fovea sparing]
- ——————————————————————————-

**Lesions of Optic Tract {4} and [Lateral Geniculate Nucleus of thalamus] {6} - PRESENT SAME VISUAL SX!
C: [Temporal fields] decussaTe at Optic Chiasm
CTL = Contralateral or (Left side in this case)
A: The Pupillary Light Reflex involves a ___ reflex and ____ reflex. Describe each?
B: After light is shone thru 1 eye, BOTH pupils constrict becuz ___ connections to [_____ nucleus] from ____ fibers traveling thru [___ ____]–> activates [Oculomotor CN3] fibers to synapse in the ___ganglion and constrict ____ _____ m.
C: What part of the brain does this test?
D: [Optic Nerve damage] presents how? Why is this?
vs.
E: [Oculomotor Nerve damage] presents how? Why is this?
A: DIRECT reflex = light is shone thru L pupil and the L pupil constricts
CONSENSUAL reflex= light is shone thru L pupil BUT R pupil constricts also
B: both pupils constrict becuz bilateral connections to [Edinger-Westphal nucleus] from optic nerve fibers traveling thru [SUP colliculus] activates [Oculomotor CN3] which travels to Ciliary ganglion ipsilaterally—>constrict [sphincter pupillae m].
C: Rostral Midbrain
D: Optic Nerve Damage—-> EQUAL PUPILS becuz signal is NEVER sent to [Edinger-Westphal nucleus]= NO REFLEX on either side
vs.
E: [Oculomotor CN3] damage—>[constricted pupil on 1 side and Dilated pupil on other]. Signal is sent from Optic N. but only 1 [Oculomotor CN3] is working = 1 sided constriction

A: Explain how the [Pupillary Dark Reflex] is transmitted?
B: Explain what causes Horner’s Syndrome and the 4 manifestations?
A: Darkness activates [Optic Tract] which –> terminates at hypOthalamus –> hypOthalamus sends its axons to descend in spinal cord and terminate at the [sympathetic preganglionic neurons of the T1-T3 lateral horn]–>sends its axons to [SUP cervical ganglion]–> Postganglionic axons in the [ciliary n.] –> Activate [iris Dilator pupillae m.]
B: Horner’s Syndrome= Damaged [SUP cervical ganglion]
1) loss of [Face Vasculature] –> flushing
2) loss of [Sweat/Lacrimal glands] –> (anhidrosis)
3) loss of [Eyelid Tarsal Muscles]—> (Ptosis)
4) loss of [iris Dilator pupillae m.] –> (miosis)

In order to change gaze & focus on very close objects you need the ____ REFLEX, which involves what 3 things?
In order to change gaze & focus on very close object you need the ACCOMMODATION REFLEX which involves..
1. eye convergence via [medial recti m.]
- Ciliary m. constriction —>Lens thicken
- Constriction of both pupils–>DEC light entering due to greater reflectance from close object

A: What are the 2 ways to Detect Motion?
B: *Motion Perpendicular to orientation axis can be detected by____ ___ ____ but___ ____is needed for more complex movements **
C: What test is used to test for Color Blindness?
2 ways to detect Motion
1. Image moves temporarily across retina while eye remains still = “temporal association”
- [Head & Eyes] move to fix the [object image] onto the fovea
B: *Motion Perpendicular to orientation axis can be detected by [Area 17 CPVC] but [V5 Temporal area] is needed for complex movements **
C: Ishihara Test
**DIFFERENCES BETWEEN RODS & CONES **
1. ____ are better for DAY Vision with ___[higher/lower] sensitivity to light. They Saturate only in _____ Light
- ____ Capture MORE light and are great for _____ Vision and ______ light. ___ have ___[FAST/slow] response time and long integration.
- Cones have Less photopigment AND Less amplification per cell
- ___ are AChromatic and ____ are Chromatic ! Explain this
- Which photoreceptor CAN’T do Bright Light?
- CONES are better for DAY Vision with Lower sensitivity to light. They Saturate only in INTENSE Light
- RODS Capture MORE light and are great for NIGHT Vision and Scattered light. Rods have slooow response time and long integration.
- Cones have Less photopigment AND Less amplification per cell
- Rods are AChromatic and Cones are Chromatic!
**Chromatic Cones = 3 types of photopigment in Cones (each sensitive to diff visible light spectrums –> Red/Blue/Green
**AChromatic Rods= ONLY 1 TYPE of photopigment in Rods
- RODS CAN’T DO BRIGHT LIGHT (since they capture more light)
A: In the OUTER ear the ___ & ______ direct sound/vibrations to tympanic membrane
B: Once in The MIDDLE ear _______ conduct sound from the tympanic membrane to the ___ _____
C: What does the EUSTACHIAN Tube do and where is it located?
A: In the OUTER ear the Pinna & [EAM Ear Canal] direct sound to the tympanic membrane
B: The MIDDLE ear [MIS ossicle bones]–>{Malleus/Incus/Stapes} conduct sound from tympanic membrane to the [Oval vestibular window]

EAM = External Auditory Meatus
A: [Bony Labyrinth] is the __-SHAPED CAVE of the ____ ear that surrounds a bony core called the _______. It’s housed in the ____ _______ bone and has a [_____ Snail Apex]. The [Bony Labyrinth] is divided into 3 canals.
B: These 3 Canals are separated by the ____ ___ _____ & ____ ___.
C: Describe These 3 Canals
A: [Bony Labyrinth] is the SNAIL-SHAPED CAVE of the INNER ear that surrounds a bony core called the [MODIOLUS]. It’s housed in the Petrous temporal bone and has a [Helicotrema Snail Apex]. [Bony Labyrinth] is divided into 3 canals.
B: 3 Canals: [Scala are separated by [Reissner’s Vestibular Membrane] & basilar membrane]
1. Scala Vestibuli (Contains perilymph & is continuous with bony labyrinth of vestibular apparatus)
- Membranous Labyrinth (contains _endo_lymph and is inbetween 2 Scala)
- Scala Tympani (Contains perilymph and separated from Cochlear Duct by Basilar membrane of the round window)

A: [Membranous Labyrinth] is filled with ______ & forms the ___ ____ (or ___ ____) which contains [________]. This is where __________
B: How far does the Cochlear Duct extend throughout the cochlea in the [Membranous Labyrinth]?
A: [Membranous Labyrinth] is filled with ENDOLYMPH & forms the COCHLEAR DUCT (or scala media) which contains [Organ of Corti]. This is where sound wave transduction—>nerve impulses occur.
B: Cochlear Duct extends throughout the cochlea, EXCEPT FOR HELICOTREMA

1) The [Organ of Corti] contains __inner row and __ OUTER rose of hair cells. Describe each of these rows (OUTER vs. inner row)
2) What are Stereocilia
3) Is hearing an Active or passive process?
[Organ of Corti] contains 1 inner row and [3 OUTER ROWS] of [hair cell cilia]
*OUTER ROW= contain Stereocilia that insert into tectorial membrane & can receive inhibitory inputs via olivocochlear n. fibers= amplifies/sharpens/suppresses responsiveness of inner row
*inner row= When cochlear fluid displaces Basilar membrane–>displaces Tectorial membrane—-> deflects [Stereocilia of inner row to move in endolymph]–> TRANSDUCTS MOST OF SENSORY AFFERENT VIA CN8
2) Stereocilia= [Tethered Hair cell cilia] arranged in a “V” and when 1 is bent –> causes neighboring Stereocilia to bend
3) Hearing is an ACTIVE PROCESS

•Cochlear nerve fibers enter brainstem at ___ _____ and terminate in ___________
B: Ventral cochlear nucleus is ___[smaller/Larger] and it projects to to the _______ nuclei in the _____. What is the TRAPEZOID BODY?
C: dorsal cochlear nucleus terminates in the ___ and ____ nuclei
D: [inferior Colliculus] relays ____ info (via ____) to_____ nucleus in the Thalamus —->sends ______ projections to _______ where it is interpreted
E: [T or F] Auditory Cortex is sensitive to lesions and can easily —> sound discrimination problems
•Cochlear nerve fibers enter brainstem at PONTOMEDULLARY JUNCTION and terminate in [Dorsal/Ventral cochlear nuclei]
B: Ventral cochlear nucleus is LARGER and it projects to ipsilateral & contralateral [SUP olivary nuclei] in Pons. **Midline crossing of the [Ventral cochlear nuclei] axons = TRAPEZOID BODY
C: dorsal cochlear nucleus terminates in the [inferior Colliculus] and [lateral lemniscus nuclei]
D: [inferior Colliculus] relays auditory info (via brachium) to [Medial Geniculate nucleus] in Thalamus —->sends auditory projections to [Area 41 Heschl’s Gyri]
E: FALSE! Auditory Cortex Lesions have to be EXTENSIVE in order to affect sound discrimination

C: Where is the Tensor Tympani m. & what is it innervated by?
D: Where is the Stapedius m. & what is it innervated by?
D2: What is the OVERALL PURPOSE of these 2 Middle ear muscles?
C: Tensor Tympani m.= Fast Striated m. (middle ear wall fibers) near eustachian tube that attaches to Malleus
{{Innervated by CN5B3}}
D: Stapedius m.= Fast Striated m. (middle ear wall fibers) tht attaches to [Stapes] near its connection with [Incus]
{{{Innervated by Facial CN7}}}
D2: Purpose of these MIDDLE EAR m. is to DEC amplification of sound oscillation—> protect us from LOUD SOUNDS & adjust loudness of voice b4 we speak[using Facial CN7]

A: Describe the Semicircular Canals
C: Utricle and Saccule are Dilations of the __ ___ that contain _____ which allows them to ______ . Why can they do this? How are they related to the Maculae?
D: What’s the difference between Utricle and Saccule in regards to Planes?
E: ºThe ______ [Utricle/Saccule] connects the [3 semicircular canals]
ºThe ______[Utricle/Saccule] is continuous with Cochlea
ºBOTH Utricle & Saccule have an ______ ______ for [______, ______ & ______ detection]
A: 3 interconnected tubes positioned at right angles to one another in 3 planes of space (1 horizontal, 2 perpendicular)

C: Utricle and Saccule are Dilations of the [Membranous Labyrinth] that contain [Ca+carbonate Otolithic granules]—>allows them to respond to gravity/acceleration because it Adds weight. They also EACH have a Maculae which contains the [Vestibular sensory Hair cells]
——————————————————————————
1. Utricle = sensory hair cells oriented in HORIZONTAL plane = sensitive to linear acceleration/deceleration in HORIZONTAL DIRECTION
-
SACcule =sensory hair cells oriented in vertical plane = sensitive to linear/acceleration/deceleration in VERTICAL DIRECTION. “We SAC those dudes Vertically”
- ——————————————————————————
E:
ºThe Utricle connects the [3 semicircular canals]
ºThe Saccule is continuous with Cochlea
ºBOTH have an Otolithic Membrane for [Gravity, Acceleration & position detection]
[PPRF] Paramedian pontine reticular formation
1. Where is this located?
- What happens when this is stimulated?
- Describe its projection
- ——————————————————————————- - Explain what the [mesencephalic reticular formation] does and is located?
- A: Vestibuloocular Reflexes (VORs) reflexly move eyes in Direction ____ of Head mvmnt. It uses ____ to get from ____ and ____ to the ____
B: Absent of (VORs) means there is ___ damage
[PPRF] Paramedian pontine reticular formation
1. Near abducens nucleus (so sometimes called parabducens nucleus)
- Stimulation = Horizontal Eye movement
- Receives multiple afferents and projects to Ocular nuclei 3, 4 and 6 using the [Ascending MLF]
- ——————————————————————————- - [mesencephalic reticular formation] = includes a [Cajal interstitial nucleus] and controls VERTICAL eye mvmnt . Is located in the ROSTRAL [PPRF]
- A: Vestibuloocular Reflexes (VORs) reflexly move eyes in Direction OPPOSITE of Head mvmnt. It uses [Ascending MLF] to get from [medial vestibular nuclei] and [SUP vestibular nuclei] —->PPRF—>[CN nuclei 3, 4 & 6]
B: Absent of (VORs) = brain STEM damage

What are the 3 ways we can get “Dizzy”?
- Vestibular input without vision (i.e. spinning in a chair with eyes closed–> constant motion that eventually results in cupola membrane returning to its baseline)
- [Motion detection from Visual system] but WITHOUT [Vestibular confirmation] (looking out car window when an adjacent car moves away= false sense of motion)
- [Motion detection from Vestibular system] but WITHOUT [Visual confirmation] (sitting in cabin of a boat during a storm= MOTION SICKNESS)
Nystagmus are __ ___ ___ that have both _ and __ components (but during test refers to ___ component only) *There are 3 types*
B1. SPONTANEOUS Nystagmus is ____[sometimes/always] pathological and is caused by ___ ____ 2º to ______
B2. What are the 3 sx?
Nystagmus are OSCILLATING EYE MOVEMENTS that have both slow and Fast components (but test refers to Fast component only) .
B1. SPONTANEOUS Nystagmus is ALWAYS PATHOLOGICAL and is caused by [Vestibular/ Brainstem/ Cerebellum] imbalance 2º to irritating or destructive lesions.
B2: Sx= [N/V] + [bp DEC] + Tachycardia
A: Tracking/Smooth Pursuit involves _____ using ______. Is Tracking/Smooth Pursuit voluntary and can it be done without Visual Stimuli?
B: What is the [Fixation Reflex]? Give example
C: [Optokinetic Railway Nystagmus]? Give example
A: Tracking/Smooth Pursuit involves “Locking” eyes onto perceived moving object using [Occipital Eye Fields]. Although These mvmnts are voluntary, smooth sweep of eyes CAN’T be done in ABSENCE of visual stimuli
B: Fixation Reflex = same as smooth pursuit mvmnt but allows us to fix on an object when BOTH person AND object are moving [Ex: Reading road sign while driving on bumpy road]
C: [Optokinetic Railway Nystagmus] = (to-and-from) oscillating eye mvmnts made when ur fixating on moving objects [Ex: Looking @ telephone pole out window of moving train]
A: Frontal eye fields are located in the __ __ ___ and are considered the _______. Frontal eye fields influence ____ nuclei using ___ and ____
B: Lesioned [Frontal Eye Fields] will lead to what?
A: Frontal eye fields are located in the MIDDLE FRONTAL GYRUS and are considered the [center for Voluntary eye Saccades]. FEF influence Ocular nuclei using [SUP colliculus] and PPRF
B: Lesioned FEF —->inability to look contralaterally (with reflex eye movements intact)
ASCENDING Medial Longitudinal Fasciculus (MLF)
1. Arises from what 2 nuclei?
- Describe where it projects to?
- what is its purpose? (2)
- Explain how CROSSED Ascending MLF Fibers are different than UnCrossed Ascending MLF Fibers?
**[ASCENDING Medial Longitudinal Fasciculus] (MLF)**
1. Arises from [medial vestibular nuclei] and [SUP vestibular nuclei]
- Projects BILATERALLY to CN3, 4 and 6’s nucleus!
- Coordinates
- [conjugate Eye mvmnts] (via reticular formation)
+/- [Head mvmnt = i.e. vestibuloocular reflex]
- ***CROSSED Ascending MLF = EXCITES XtraOcular m.
vs.
*UNCrossed Ascending MLF= inhibits xtraocular m.

Describe the 3 Vestibulospinal Tracts
- Lateral vestibulospinal tract Arises from [_____ nucleus] & descends ___ to ___ spinal cord levels to activate _____
- MEDial vestibulospinal tract is the MAJOR component of ___ __ and comes from [_____ nucleus] . Projects to ___ spinal cord levels to innervate ______
- Spinovestibular tract
- Lateral vestibulospinal tract
Arises from [lateral vestibular nucleus] & descends ipsilaterally to ALL spinal cord levels to activate EXTENSOR motor neurons - MEDial vestibulospinal tract
is the MAJOR component of DESCENDING MLF and comes from [medial vestibular nucleus] . Projects to CERVICAL spinal cord levels to innervate neck muscles - Spinovestibular tract = collaterals of spinoCEREbellar projections
A: _____ hair cells of the [Crista ampullaris] produce a gelatinous [_____] to cover and protect them.
B: How are the Semicircular Canals paired up?
A: Stereocilia hair cells of the [Crista ampullaris] produce a gelatinous [CUPULA] to cover and protect them.
B: ANT canal is parallel to POST canal from other side. Horizontal canals from both sides form functional pair together
A: Equilibrium is Maintained and Controlled by what 3 sensory inputs? How many is needed to maintain Balance
B: What are the Sx (3) of Vertigo?
B2: Causes of Vertigo (2)?
A: Equilibrium is Maintained and Controlled by
1. Vestibular apparatus of internal ear
2. Vision
3. Proprioreception
[It only requires 2 out of the 3! to maintain Balance]
——————————————————————————
B: Vertigo Sx = DNP = Dizziness, NV and Pallor
B2: Causes: [Degenerated Ca+ Crystal Otoliths] vs. [Acute Labyrinthitis]
What are the 6 Sensory Receptors that utilize the [Dorsal Spinocerebellar Tract] Pathway for ______ ______ ______.
5 Sensory Receptors that utilize the [Dorsal Spinocerebellar Tract] Pathway for UNCONSCIOUS IPSILATERAL PROPRIORECEPTION
MMM JRP
- Meissner’s Corpuscle
- Pacinian Corpuscle
- Merkels Disk
- Ruffini
- Joint Receptors
- Muscle Spindles

Describe This Receptor:
[Free Nerve Ending]
- Is it Encapsulated?
- Function (2)
- Distribution (2)
[Free Nerve Ending] Receptor:
- NOT Encapsulated (“Free Hairy Merkel”)
- Pain/Temp
- Deep skin & viscera

Describe This Receptor:
[Merkel’s Disk]
- Is it Encapsulated?
- Function
- Distribution [4]
[Merkel’s Disk] Receptor:
- NOT Encapsulated (“Free Hairy Merkel”)
- Touch
- Feet/hands/genitalia / lips

Describe This Receptor:
[Hair Follicles]
- Is it Encapsulated?
- Function
- Distribution
[Hair Follicles] Receptor:
- NOT Encapsulated (“Free Hairy Merkel”)
- Touch
- Anything with Hair

Describe This Receptor:
[Meissner’s Corpuscle]
- Is it Encapsulated?
- Function
- Distribution [4]
[Meissner’s Corpuscle] Receptor:
- Encapsulated !!
- 2 Point Discrimination
- [hairLESS Skin] / joints / ligaments / fingertips

Describe This Receptor:
[Pacinian Corpuscle]
- Is it Encapsulated? ]
- Function
- Distribution [4]
[Pacinian Corpuscle] Receptor:
- Encapsulated !!
- Vibration
- Fingers & Toes / mesenteries / peritoneum

Describe This Receptor:
[Ruffini Ending]
- Is it Encapsulated?
- Function
- Distribution
[Ruffini Ending] Receptor:
- Encapsulated !!
- Stretch / pressure
- Dermis

Describe This Receptor:
[Joint Receptor]
- Is it Encapsulated?
- Function
- Distribution [2]
[Joint] Receptor:
- Encapsulated !!
- Joint Position
- [Joint Capsules] & Ligaments

Describe This Receptor:
[Neuromuscular Spindle]
- Is it Encapsulated?
- Function
- Distribution
[Neuromuscular Spindle] Receptor:
- Encapsulated !!
- Limb muscle Stretch
- Muscles

Describe This Receptor:
[Golgi Tendon Organs]
- Is it Encapsulated?
- Function
- Distribution
[Golgi Tendon Organs] Receptor:
- Encapsulated !!
- MUSCLE Tension
- Muscle tendon Junctions

[Dorsal Posterior Horn] contains the [Substantia gelatinosa] and [Nucleus Proprius]
Describe the [Substantia gelatinosa] (3)
**[Substantia gelatinosa]**
ºIs “Pain Gate keeper” & filters sensory information by synapsing on dendrites in [Nucleus Proprius]
ºHomologous to [spinal trigeminal nucleus]
ºAxons ascend & descend 1 to 4 segments in [Dorsolateral Fasciculus /Zone of Lissauer]
- [Pain, temperature, position sense, vibration from skin/body wall and pressure] come from the ___ component
- [Motor projections to Viscera, Glands & blood vessels] = ____ component
- Pain, sensations of FULLNESS/STRETCH come from the ____ component
*Alar Plates derive into the ____/____ root
Basal Plates derive into the ___/_____ root
- [Pain, temperature, position sense, vibration from skin/body wall and pressure] come from the GSA component
- [Motor projections to Viscera, Glands & blood vessels] = GVE component
- Pain, sensations of FULLNESS/STRETCH from viscera come from the GVA component
*Alar Plates Derive into SENSORY/DORSAL ROOT
{Afferent and Alar = Sensory}
*Basal Plates derive into MOTOR/VENTRAL Root
A: What’s special about the CLOSED medulla?
B: What are the Corpora Quadragemini? How is it related to “SLOW AIM”
C: Describe the 3 Cerebellar Peduncles and what their attached to
D: Which Cerebellar Peduncle DECUSSATES in the Caudal Midbrain?
A: The CLOSED Medulla is the part of Medulla NOT UNDER 4th Ventricle
B: [Corpora Quadragemini] are 4 Colliculi tht sit on DORSUM of Midbrain and is AKA [TECUM OF MIDBRAIN].
**SLOW = SUP colliculi talk with [Lateral geniculate] for Optic “WVision”
**AIM = Auditory system uses Inferior Colliculi which talks with [MEDIAL geniculate]
————————————————————————————–
C:3 Cerebellar Peduncles
1- **SUP Cerebellar Peduncle = MOSTLY EFFERENT except [Ventral Spinocerebellar tract] and is in midbrain
2-MIDDLE cerebellar Peduncle= LARGEST, is afferent and attaches to Pons
D: **SUP Cerebellar Peduncle DECUSSATES inbetween [substantia nigra] of caudal MIDBRAIN …on its way to [Red Nucleus of midbrain]
A: [Crus Cerebri Cerebral Peduncles] are on the ______[Dorsal/Ventral] Midbrain and responsible ……
B: Where does the Infundibulum Stalk sit in relation to the [Crus Cerebri Cerebral Peduncles]? What does it suspend?
C: Cerebellar Peduncles would stain ____ with myelin stain. Why?
A: [Crus Cerebri Cerebral Peduncles] are on the VENTRAL Midbrain and responsible for connecting Cerebrum with brainstem/spinal cord
B: Infundibulum Stalk hangs Between [Crus Cerebri Cerebral Peduncles] of midbrain and suspends PITUITARY GLAND ventrally
C: Cerebellar Peduncles would stain BLACK with myelin stain because they’re white fibers lol
C: Describe the Pathway of [Spinal CN11]
————————————————————————————–
D: What happens when the _____ ______ ____ squishes [Oculomotor CN3] and why?
D: When the Temporal Lobe UNCUS squishes [Oculomotor CN3] —> LATERAL GAZE! (because CN6 Abducens just takes over)
- Which Artery perfuses the [LATERAL Medulla] and what Parent Artery does it come from?
- What’s the Name of Dz that occurs when this Artery becomes occluded?
- Name the Sx of this dz and what syndrome is causes? (5)
- The PICA (Daughter of Vertebral a.) perfuses Lateral Medulla
- Can Cause [Lateral Medullary syndrome of Wallenberg]
- causes ischmia and —> Lucy Has 2 VPN
Limb Dysmetria ipsilateral- from [inf cereberllar peduncle]
Horner’s Syndrome ipsilateral- from [descending sympathetic fibers]
2TVP loss Contralaterally-from [medial lemniscus involvement]
[Vocal Cord/Palatal Weakness] ipsilateral- from [nc. ambiguous]
[Pain & Temp] impairment ipsilateral face/Contralateral body (STT)- from [descending CN5, n & t] & STT
Nystagmus- from vestibular nc.

1) Where is the [Nucleus of Solitary Tract] [NST] located?
2) What is it responsible for? (2)
- [NST] Nucleus of Solitary Tract are in the [Medulla]
- Taste [upper NST] &; GVA Sensation [Lower NST]
B: What are these Structures PERFUSED By?
- Olive (2)
- Basal Bons
- [Middle cerebellar peduncle] (2)
- [Crus Cerebri Cerebral Peduncle]
- .[inf cerebellar peduncle] AKA ___ ____
PERFUSIONS!
6. Olive perfused by [PICA or actual Parent Vertebral a.]
- Basal Pons perfused by Basilar a.
- [Middle cerebellar peduncle] perfused by [AICA and Basilar a.]
- [Crus Cerebri Cerebral Peduncle] perfused by PCA {POST cerebral a.}
10 .[inf cerebellar peduncle] (AKA RESTIFORM BODY) perfused by PICA

A: [Lower Motor Neurons] are Motor neurons of the ___ & _____ They are arranged into 4 columns and release ____ onto _____ receptors of ____ _____ Lower Motor Neurons are recruited based on __ & ____
B: What are the 4 Column Arrangements and which muscles do they innervate?
A: Lower Motor Neurons are Motor neurons of the Brainstem & Spinal Cord.
They are arranged into 4 columns and release ACETYLCHOLINE onto nicotinic receptors of target m.
Lower Motor Neurons are recruited based on size & Force
B: 4 Column Arrangement:
- medial LMN–>axial trunk m.
- Lateral LMN—>Distal Limb m. (extremities)
- Dorsal LMN—>FLEXORS
- venTral LMN——->exTensors
Describe the Descending pathways for Lower Motor Neurons. These all act as 1 of the ___ ______ in the Spinal Cord
A: Corticospinal tract (lateral)
B: Vestibulospinal tract [2]
C: Reticulospinal tract [2]
D: Tectospinal tract
E: Rubrospinal tract
Descending pathways = CONTROL SYSTEM in spinal cord LMNs
A: Lateral CST=ALL Excitatory (Glutamate is the transmitter)
B: Vestibulospinal= Head mvmnt & postural adjustments
C: Reticulospinal= locomotion & postural control
D: Tectospinal = reflex of turning head in response to visual/auditory stimuli
E: Rubrospinal= no significance in humans
A: CorticoBULBar tract (AKA ___ tract) is an ____ MOTOR NEURON tht descends ANterior to _____ tract. It usually ends on ____ of the ___ _____ but sometimes ends on _____inside the ____.
B: Name the 3 CN nucleus that do NOT receive DIRECT CorticoBULBar innervation.
A: CorticoBULBar tract (AKA Corticonuclear tract) is an UPPER MOTOR NEURON that descends ANterior to Corticospinal tract. It usually ends on interneurons of [Reticular formation] but sometimes ends on [motor neurons of CN] inside the brainstem.
B: Oculomotor, Trochlear & Abducens nucleus does NOT receive DIRECT CorticoBULBar innervation.
Describe The Cortex Origin of Upper Motor Neuron for CN nuclei involving:
- Chewing ex. Upper Motor Neurons for Chewing (CN__) comes from ____[R vs. BOTH] side(s) of the Cortex before reaching the Nucleus
- Facial Droop vs. Bell’s Palsy
- [speaking & swallowing]
- tongue mvmnt
Cortex Origin of Upper Motor Neuron for CN nuclei involving:
- Chewing ex. UMN for Chewing (CN5) comes from [Both BUT More of 1 side] before reaching Nucleus
-
Facial Droop vs. Bell’s Palsy: UMN come from BOTH Cortex before reaching CN7 Nucleus –> ONLY 1 LMN Innervates Entire Face ipsilaterally
* Facial Droop= Lesion of Facial UMN*
* BeLLs Palsy= Lesion of Facial LMN = complete face droop* - tongue mvmnt: UMN comes from [Both BUT More of 1 side Cortex] before reaching CN12 Nucleus

What are Betz cells?
Make up 3% of [CST-Corticospinal Tract] and are concentrated there
Primary Motor Cortex makes up 50% of CST and the rest comes from [Adjacent Frontal motor and Parietal areas]
Area 44 = ______
Area 22 = ______
Area 41 = ______
Hearing is ______[unilateral/Bilateral] above the cochlear nucleus
**99% of hearing comes from ______[Outer/inner] row of hair cells
What is the Other row for?
Area 44 = Broca’s
Area 22 = Wernicke’s
Area 41 = Heschel’s Gyrus / Primary Auditory Cortex
Hearing is BILATERAL above the cochlear nucleus = why it’s hard to knock out
**99% of hearing comes from inner row
Outer row = displacement sensitive so controls tectorial membrane
A: The _____ Artery (_____ circulation) perfuses MOST of the CEREBRUM.
It bifurcates into the ______ and ______ artery
B: What are the 3 daughter branches of this Artery?
The INTERNAL CAROTID Artery (ANTERIOR circulation) perfuses MOST of Cerebrum (70%). (Vertebral a. perfuse 30%)
It bifurcates into….. [Anterior Cerebral a.]—->medial cortex and [middle cerebral a.]–>lateral cortex
B: Daughter branches: 1) ophthalmic artery 2) ANT Choroidal a. 3) POST communicating a.

A: The _____ system (______circulation) perfuses Brainstem, Cerebellum & Spinal Cord. It Bifurcates into ____ cerebral arteries.
B: Describe this system
C: What are the daughter branches for each of these Arteries?
The VERTEBROBASILAR system (POSTERIOR circulation) perfuses Brainstem, Cerebellum & Spinal Cord.
B: 2 Vertebral a. Join—> 1 Basilar ARtery–>Bifurcates into PCA [POST cerebral a.]
C:
*Basilar branches = [(AICA) ANT inf. cerebellar a.] & [(SCA)SUP cerebellar a.]
**Vertebral branches = PAP! (, ASA PSA, PICA) -ANT Spinal a. -POST Spinal a. -POST inferior cerebellar a.

A: 80% of Strokes arise from occlusion in the ____ a. which is a bifurcated branch of the ______ Artery. What part of the brain is perfused by this bifurcated branch?
B: What part of the Brain does the [POST cerebral a.] perfuse? [2]
80% of strokes<—–[middle cerebral a.] which is a bifurcated branch of INTERNAL CAROTID ARTERY.
[middle cerebral a.] perfuses lateral cortex
B: [POST cerebral a.] perfuses Occipital lobe & Temporal Lobes (memory lost)

A: The Circle of Willis Interconnects the ____ and ____ circulations. How does it do this exactly?
B: How is it related to perfusion of deep cerebral structures? (2)
C: What are the Anterior/Posterior Perforated Substance?
{Circle of Willis} Interconnects ANTERIOR and POSTERIOR circulations. It forms 1. [ANT communicating a.] between the two [ANT cerebral a.] and [POST communicating a.] between [Internal carotid] and [POST cerebral a.]
B: [Circle of Willis] surrounds brain base it gives rise to small perforating ganglion arteries (via MCA) called [lenticulostriate a.] –perfuse—> [deep cerebral structures (internal capsule/basal ganglia/thalamus)]
C: entry points of perforating a. on Brain Base

Blood Brain Barriers are formed by _____ ___ _____which use ___ junctions between ____ cells to filter blood coming from _______.
B: What are Pericyte? Where is it located (2)?
Blood Brain Barriers are formed by [ASTROCYTE GLIAL CELLS] which use TIGHT junctions between ENDOTHELIAL cells and [ENDOTHELIAL CELL LAMINA] to “gatekeep” blood coming from from CAPILLARIES(which never make direct contact with brain tissue)
B: Pleuripotent cell that gives rise to other blood vessels and regulates endothelial cells. Located [under basal lamina] but [ON TOP OF ENDOTHELIUM]

The Brain is ___% of Body weight BUT uses ___% Oxygen!
A: metabolic: INC neuronal activity—>________ released —>[______ _______ _______ activation]—>________ ________released at feet —> applied to vessels to ________ ________ in that area
B: How is Control of Blood Flow AUTOregulated?
C: How is Control of Blood Flow regulated neuronally?
D: What is the normal Flow of Blood and what happens when that number is low? [2]
Brain is 2% Body Weight BUT uses 25% Oxygen!
-Control of Blood Flow:
A: metabolic: INC neuronal activity—>Glutamate released —>[astrocyte feet receptor activation]—>VasoDIOLATES factors released at feet —> applied to vessels to DILATE VESSELS IN THAT AREA
B: AUTOREGULATION: Arterial & Smooth muscle cell mediated
C: neuronally: autonomic fibers innervate Cerebral vessels
D: Normally= [55 ml Blood/100 g in 1 minute]
20 ml = neurons stop electrically firing
10 ml = NECROSIS OF BRAIN!
Valveless Cerebral Veins —(drain into)—>___________—–(drain into)—–> _____ ______ ______ + [Basilar Venous Plexus]
B: The [Basilar Venous Plexus] drains mostly ____ _____ and communicates with +_____________
C: Where does the [Cerebellum and Brainstem] draiiin their veiiiinnns?
Valveless Cerebral Veins—(drain into)—>[DURA VENOUS SINUSES]—-(drain into)—-> [INTERNAL JUGULAR VEIN] + [Basilar Venous Plexus]
B: [Basilar Venous Plexus] mostly drains BASE OF BRAIN and communicates with [SPINAL CORD EPIDURAL VENOUS PLEXUS]
C: [Cerebellum and BrainSTEM] drain their veins into the [GREAT VEIN OF GALEN]! (along w/Deep Veins)
Describe the 2 Major Divisions of Cranial Venous Drainage -Superficial Veins (5) vs. Deep Veins (6)
****Superficial Veins*** 1. Superficial group = Dumps INto Superior/inferior Sagittal Sinuses 2. Inferior group= empties with transverse AND cavernous sinus —->[SUP/inf sagittal sinus]—-> **[SINUS CONFLUENCE]**—->Transverse sinuses—>IJV
vs.
Deep Veins = empty into [Internal cerebral Veins] —>[GREAT VEIN OF GALEN]—–>Straight Sinus—->**[SINUS CONFLUENCE]**—–>Transverse sinuses ——>IJV

What does the CT scan delineate?

SubArachnoid Hemorrhage going into the Cisterns

A: What type of Nystagmus does Drugs/Metabolic produce?
B: What type of Nystagmus does Anatomical lesions produce?
C: Give an example of Physiological Nystagmus
A: Symmetrical Nystagmus
B: Asymmetrical nystagmus
C: Rotating in a swivel chair and then suddenly stopping
A: MOD for Bell’s Palsy
B: Clinical Manifestation (3)
C: Cause
D: Short-term tx
A: BeLLs Palsy= Sudden and Non-traumatic Lesion of Facial LMN = complete face droop
+
[possible taste loss over ipsilateral ANT Tongue (chorda tympani branch)]
+
[possible ipsilateral hyperacusis (stapedius branch)]
C: [Facial CN7 inflammation in petrous bone (possibly viral)]
D: Steroids

List Clinical Manifestation for these Facial CN7 lesions
- [Facial CN7 LMN]
2a. [Petrous Bone: Chorda tympani fibers]
2B. [Petrous Bone: Stapedius fiber]
- [CAAN- Cerebellopontine Angle Acoustic Neuroma]
- [Pontine Lesion]
FTSDL

[Facial Paralysis ipsilateral / Taste loss / Sound sensitivity INC / Deafness&Tinnitus / Lateral Gaze impairement]
- [Facial CN7 LMN] = F
2a. [Petrous Bone: Chorda tympani fibers] = FT
2B. [Petrous Bone: Stapedius fiber] = FTS
- [CAAN- Cerebellopontine Angle Acoustic Neuroma] = FTSD
- [Pontine Lesion] = FTSDL
Brain Stem Synromes
Describe:
A: Brain stem lesions (2)
B: [R Pontine Infarct] (2)
A. Brain stem lesion –>
- ipsilateral CN deficit
- Contralateral UMN limb weakness
B: R Pontine Infarct–>
- [R LMN Facial Weakness from CN7 deficit]
- [L Hemiparesis from (Corticospinal Pyramidal tract) deficit]

Stroke - Brain Stem Syndromes
Describe:
[Medial Midbrain of Weber syndrome]
A. [Medial Midbrain of Weber syndrome]
**Occlusion of [POST Cerebral a.] –>
- ipsilateral CN3 lesion
- Contralateral hemiplegia (Cerebral Peduncle)

A: Explain the *Rinne Test* [3]
B: What two Auditory Defects does it differentiate between?
1st: Place vibrating tuning fork on mastoid process of suspected side. Pt should hear vibrations in that ear = Bone conduction route intact
2nd: While tuning fork is still vibrating move prongs of fork to [outside ear pinna]–> where *Airconductionis 100x more sensitive than bone*
3rd: Pt should still hear sound for 15 more seconds. If pt can’t hear sound for that long = air conduction deafness on that side
B: Differentiates between [Air and SensoriNeural: 2nd step] defects

A: Explain **WEBER’S TEST** [4]
B: What two Auditory Defects does it differentiate between?
A: WEBER’S TEST
1st: Tuning Fork placed on Skull midline
2nd: Normally sound is conducted simultaneously by both [ossicular air] and [bone] routes which are out of phase w/each other (1vibration up and 1vibration dwn)
3rd: Being out of phase—>Cancel each other out on both sides of head–>sound perceived as coming from midline
4th: If [ossicular air] route loses conduction, cancellation effect on tested ear is DEC and net vibration will be GREATER on the AFFECTED SIDE
* can also be caused by [CTL Ear has SensoriNeural defect]*
B: Differentiates between [Air and SensoriNeural defect: 1st step]

A: Clinical Course of Carbon Monoxide Poisoning
B: Tx
C: Which drugs cause Drug-related Stroke Syndrome (4)
1st: HA / vomiting / blurred vision
2nd: Coma / Seizures / Cardiopulm arrest (Amnesia / Parkinsonism)
B: [Hyperbaric O2 chamber]
C: [Cocaine (most common) / Amphetamine / PCP / LSD]–> vasoconstriction or abrupt HTN–>cerebral infarct/hemorrhage
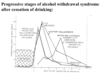
A: Describe the 2 stages of EtOH Withdrawal
B: What factors can be Fatal during EtOH Withdrawal (2)
C: When is a Brain Scan during EtOH Withdrawal warranted?
- [Early Hypersympathetic Stage] = tremors + sweaty + tachycardia + [limited convulsive Tonic–>Clonic seizures] tht occur 12 hrs-3 days post drinking]
- [Later (3-4 days post drinking) Delirium Tremen Stage] = [Fluctuating motor/autonomic activity] + confusion + hallucinations(visual and auditory)
B: Coexisting infectio vs. Trauma
C: If pt has [Partial / Focal Seizure] this suggest focal lesion
Chronic Alcoholism Syndrome
A: Causes (3)
B: What type of Head Trauma can it cause? (2)
C: Clinical Manifestations (4)
A:
- EtOH itself
- Malnutrition from EtOH
- Vitamin (B1) Deficiencies from EtOh
B: [Subdural vs. Cerebral Hemorrhage]
C:
- [Wernicke Encephalopathy] —> [Korsakoff Psychosis]
- [Alcoholic (ANT SUP Cerebellar vermis) Degeneration]
- Peripheral Neuropathy
- Dementia
Chronic Alcoholism Syndrome
A: [Wernicke Encephalopathy]
- Sx (4)
- Tx
B: [Korsakoff Psychosis]
-Sx of [Korsakoff Psychosis]
A: [Wernicke Encephalopathy]
- [Nystagmus vs. Ophthalmoplegia vs. (Gait ataxia) vs. Confusion]
- Tx = Thiamine B1 supplement
B: [Korsakoff Psychosis] = CHRONIC PHASE!
-Amnesia compensated with Comnfabulation

A: Brain uses _____ metabolism intaking [___% Cardiac Output] and [____% O2 consumption]
B: Describe pathogenic course once Cerebral ischemia occurs (2)
C: Which brain cells are most ischemia sensitive? (4)
D: Which brain cells have variable ischemia sensititvity (3)
A: Brain uses Aerobic metabolism intaking [20% Cardiac Output] and [15% O2 consumption].

Brain has NO O2 reserve = SENSITIVE TO ISCHEMIA
B: Post cerebral ischemia –> [Normal for 8-10 seconds] –> [Irreversible Damage AFTER 6-8 minutes!]
C: Neurons > Oligodendrocytes > [Endothelial Cells] > Astrocytes
D:
- Cerebellar Purkinje
- [(SHC-Sommer’s Hippocampus CA1) Pyramidal neurons (long term memory)]
- [Cortex Watershed Layers 3 & 5] Pyramidal neurons (–>Laminar Necrosis if pt survives Global ischemia longer than 3 days)
A: What type of pathology makes up the lesser porition of Stroke cause? Describe its etiologies (2)
A: Intracranial Hemorrhage makes up 15% of causes of Stroke (Cerebral Ischemia is most common)
- Intraparenchymal Hemorrhage (HTN vs. amyloid)
- SubArachnoid Hemorrhage (Saccular Aneurysms vs. AVM)
A: Brain Histology post Global Cerebral Ischemia (3)
B: When do these Histological changes occur?
A:
- [Red Dead Neurons] (neuronal cytoplasm appears red because necrosis attracts eosinophilia)
- DEC Nissl substance
- Dark Pyknotic nuclei
B: [6-12 hours post insult]
What type of Necrosis most likely occurs in the Watershed Areas of the Cortex?
B: Describe these Watershed Infarcts
Laminar Necrosis of
[Cortex Watershed Layers 3 & 5] Pyramidal neurons
—->Laminar Necrosis if pt survives Global ischemia longer than 3 days
B: Wedge-shaped areas of hyperemia and softening (particularly in ACA and MCA Watershed Zones)

A: Ischemic stroke –> what kind of neuro deficits?
A2: Where do [In-Situ Thrombotic strokes] typically occur?
B: [Small Vessel SubCortical infarct] occurs from _____ (embolism or thrombosis). What’s the MOD of Lacunar Stroke?
C: Describe Lacunar Syndrome (2)
A: Ischemic Stroke –> Focal neuro deficits (In-Situ Thrombotic vs. Embolic)
A2: Thrombotic= [Bifurcation of Internal Carotid and MCA]
B: [Small Vessel SubCortical infarct] occurs from [In-Situ Thrombosis] (Large Vessel Dz can be Thrombosis or embolism):
- lenticulostriate vessels perfuse [Be TIPC]*
1) Lacunar Stroke= ischemia of lenticulostriate vessels –> [cystic infarcts < 1.5 cm (mostly seen with MRI)] –> Lacunar Syndrome (listed below)
1A: [Internal Capsule/Pons/Corona Radiata] Stroke–> pure Motor stroke (ataxia vs. hemiplegia vs. clumsy hand)
1B: ThalamuS Stroke –> pure Sensory stroke
1C: Basal Ganglia - not included in Syndrome
Note: Lacunar lesions may be WITHOUT sx

A: Describe the Radiographic finding below
B: Clinical Presentation (3)

A: MRI Brain:
Ischemic hemispheric infarct of the [MCA territory] –> Midline shift
B:
1) CTL [Hemiparesis / Hemisensory loss/ Visual field deficits] affecting lower face and UE > leg
2) Hemisphere infarct will be associated with [CTL expressive aphasia]
3) [Non-involved hemisphere ipsilateral neglect syndrome]
A: What 2 factors are the Gross & Micro findings post Ischemic infarction dependent on?
B: Describe the Gross findings of the brain from an Acute Ischemc Infarct (3)
C: What pathology is shown in the image below? Describe its features (3)

A: [Time after insult (acute vs. subacute vs. remote)] and [Embolic(red) vs. Thrombotic(pale)]
B: Brain Image on L
1) Swelling / softening / pallor of brain parenchyma
2) Indistinct border
3) Blurring of Cortex/DEC White matter differentiation
C: SUBAcute Ischemic Infarct = [More Distinct Borders] + [Tissue Liquification] + [Early PMN & Late macrophages/vascular proliferation]

What type of Cerebral Infarct is depicted in image?

Remote MCA Infarct (will have cystic spaces)

A: What type of Cerebral Infarct is depicted in image?
B: Features of this infarct (3)
C: Which artery is most commonly responsible for this type of infarct?
D: MOD

Embolic Infarct

1) [Usually smaller & centered at gray-white jxn]
2) Can be single or multiple
3) May involve more than 1 vascular territory
C: MCA
D: Can occlude Large Artery at origin OR [occlude Large Artery and then embolize to [Distal Large A.]
A: What type of Infarct is depicted in image?
B: typical size of infarct
C: Where does this infarct (5)
D: Cause (2)

Lacunar Infarct

B: small (no more than 1.5 cm) and cystic
C: Be TIPC
[(Basal Ganglia) /Thalamus / Internal Capsule/ Pons / Corona Radiata which all = SubCortical White Matter)]
D:
1) HTN (Arterial Hyalinosis)
2) [small vessel dz]
A: Hemorrhagic Infarctions are usually ______ in nature
Intracranial hemorrhage
B: Name the common cause of [Above Arachnoid] Intracranial hemorrhage. List 2 examples.
C: List the 2 Types of [BELOW Arachnoid] Intracranial hemorrhage and what their caused by
A: Hemorrhagic Infarctions are usually Embolic in nature
Intracranial hemorrhage
B: Above Arachnoid: Traumatic causes (Epidural and SubDural Hematomas)
C: BELOW Arachnoid: Cerebrovascular Dz is cause
- SubArachnoid Hemorrhage (usually from Aneurysms)
- Parenchymal Hemorrhage (usually from HTN)

A: List the Common Locations for [Parenchyma HTN Hemorrhages] (4)
B: Which vessels contribute to [Parenchymal HTN Hemorrhages] and is associated with [Pseudoaneurysm Rupture]? (3)
What is the name of this particular phenomena?
A:
- Putamen
- Thalamus
- Pons
- Cerebellum
B: [Charcot Bouchard]:
- Lenticulostriate arteries
- Paramedial pontine vessels
- Short circumferential vessels of Cerebellum & white matter
* similar distribution as lacunar infarcts. Histo with minimal tissue necrosis but does have cystic spaces containing macrophage-laden hemosiderin*

Cerebral Ischemia manifestation varies based on Age Of Infarct: Describe…
ACUTE
A: Time period
B: Gross (2)
C: Micro (2)
A: 6 - 48 hours
B: [pale, soft , swollen] + [indistinct border/blurred grey-white junction]
C:
- 6-48 hours= [Dead Red Neurons] + Pallor Edema
- 1-3 Days= Neutrophil infiltration + Necrosis

Cerebral Ischemia manifestation varies based on Age Of Infarct: Describe…
SubAcute
A: Time period
B: Gross (5)
C: Micro (3)
A: [2 days - 3 Weeks]
B: Gelatinous / Friable / Distinct Border / [Tissue liquefaction] / [Glial Scar ( >2 weeks)]
C:
[early neutrophils]–> [macrophages in 3-5 days] —> [vascular proliferation & reactive gliosis in 1-2 weeks]

Cerebral Ischemia manifestation varies based on Age Of Infarct: Describe…
Chronic
A: Time period
B: Gross (3)
C: Micro (2)
A: [> 3 Weeks]
B: Cystic / [+/- Hemosiderin staining] / [2° Degeneration]
C:
- [Astrocytic Gliosis]
- [Residual Macrophages]

A: Causes of [SAH- SubArachnoid Hemorrhage] (4)
B: Labs
C: [SAH- SubArachnoid Hemorrhage] MOD
D: [Berry Saccular Aneurysm] MOD
E: What 3 Dz’s are [Berry Saccular Aneurysm] associated with?
”[AnTi AA] led me straight to the SAH”
A:
- Aneurysm (Berry Saccular Aneurysm) = COMMON NON-TRAUMATIC CAUSE
- Trauma = MOST COMMON OVERALL CAUSE
- AVM
- Anticoagulation
B: CSF with xanthochromia (yellow hue from bilirubin)
C: “Berry-like” thin-walled (no media) outpouchings from arterial branch points –> Rupture at the dome –> Global Vascular spasm –> Global cerebral ischemia
D: Outpouching of [Circle of Willis: ANT Communicating Artery] 2º to [Tunica media congenital defect]—> Rupture at the dome –> SubArachnoid Hemorrhage = 50% Fatality within first 24 hours, but most are asx until rupture
- [Auto Dom Polycystic Kidney Dz]
- [Ehlers-Danlos]
- Marfans

Intraventricular Hemorrhage
A: Demographic
B: Where does the Hemorrhage occur
A: Premature Infants (RARE IN ADULTS)
B: Germinal Matrix beneath ependyma(easily ruptures into ventricles)

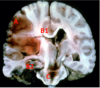
Duret Hemorrhage MOD (2)
A: Herniated [TUMTL-Transtentorial Uncal Medial Temporal lobe] from various mass lesions (hemorrhage/neoplasm) –>
- Pons Compression
- Perforating Arteriole stretching –> ischemia

A: What type of Cerebral Pathology is depicted in image?
B: MOD
C: Prognosis

Epidural Hematoma
B: [Temporal Bone Fracture] –> [Middle Meningeal Artery rupture]–> [Football/Lens shaped lesion from blood between dura & skull]
C: Pt may be lucid b4 any neuo signs manifest but Herniation is lethal complication
A: What type of Cerebral Pathology is depicted in image?
B: MOD
C: Prognosis
D: Demographic and Why them?

Subdural Hematoma

B: [Truama vs. Age] -> [Tearing of bridge veins between Dura & Arachnoid] –> [Crescent shaped lesion]
C: Progressive neuro signs but Herniation is lethal complication
D: Elderly (A**ge-related cerebral atrophy stretches bridging veins)
Describe:
A: Tonsillar Herniation
B: Subfalcine Herniation
A: [Cerebellar tonsils] –herniates into–> [Foramen magnum]–> Brainstem compression –> Cardiopulm arrest!
B: [Cingulate Gyrus] –herniates into–> [Falx Cerebri]–> [ACA compression] –> infarct

Describe:
A: Uncal Herniation (including which 3 vessels it affects)
B: What are the manifestation of each vessel affected
C: Which Letter in image below is associated with Uncal Herniation

[TUMTL-Transtentorial Uncal Medial Temporal lobe] –herniates under–> [Tentorium Cerebelli]–> Compression of [POP- PCA / Oculomotor CN3 / Paramedian Pontine vessels] –>
- [Occipital lobe infarct from PCA compression] ( —>CTL homonymous hemianopsia w/Macular/fovea sparing)
- [“Down and Out” Eye + Dilated Pupil]
- Duret Hemorrhage (with Pons compression)
C: {letter C}=Duret Hemorrhage

Identify
A- [Middle Cerebral Artery Infarct]
B1 - Subfalcine Herniation
B2 - [TUMTL-Transtentorial Uncal Medial Temporal Lobe] Herniation
C - Duret Hemorrhage (comes from TUMTL Herniation)

A: [Snellen Wall Chart] is used for Visual Acuity. What does 20/100 vision actually mean for a pt?
B: What does a Negative Pinhole Result (pt vision does not improve when looking through pinhole) possibly indicate?
C: Is the Optic Nerve lateral or medial? Identify the structures in the image

A: [Pt reads at 20 feet] what a [normal person would read at 100 feet] in that eye
B: Visual problem may be neurological
C: Optic Nerve is Medial.
So [R = [Optic Disc w/ Optic N.]] vs. [L = Macula]

Describe:
A: Physiological Blindspot
A2: What happens to this Blindspot during Papilledema
B: Pathological Blindspot (AKA ____ )
C: How do you differentiate [Glaucoma/Retinal Degeneration] from [Psychogenic Tunnel Vision] in pts with Constricted Visual Fields
A: Normal Blind spot that occurs due to Optic disc having no rods/cones (center of vision). This ENLARGES with papilledema from INC ICP
B: Pathological Blindspot (AKA SCOTOMA) occurs from [Ocular/Retinal/Optic N.] Disorder. Usually in 1 eye.
C:
- If Pt Visual Field enlarges once you move target away from them = [Glaucoma/Retinal Degeneration]
- If Pt Visual Field continues to be Constricted even as you move target away from them = [Psychogenic Tunnel Vision]
A: What type of Visual Defect would result from a Bilateral Outer Chiasm lesion?
B: What type of Visual Defect would result from [PCA-Post Cerebral Artery] dz (2)
B2: This defect would still have what things intact (2)
A: Heteronymous (Bilateral) Nasal Hemianopsia

B:
- Cortical Blindness from Bilateral Occipital lobe infarct
vs.
- [CTL homonymous hemianopsia w/Macular/fovea sparing] from Unilateral Occipital lobe infarct
B2: Normal [Pupillary light reflex] & [No Optic Atrophy]
A: Nystagmus are __ ___ ___ that have both _ and __ components (but during test refers to ___ component only) *There are 3 types*
B1: Describe the [IPNB- Induced Postrotatory Nystagmus of Barany]
B2: What does this test ultimately indicate
Nystagmus are OSCILLATING EYE MOVEMENTS that have both slow and Fast components (but test refers to Fast component only)
B1.[IPNB- Induced Postrotatory Nystagmus of Barany] = Rotation of Head by 45º (Dix-Hallpike maneuver) sets endolymph of [Post semicircular canal] in motion—>causes deflection of stereocilia hair cells.
B2: If Nystagmus occurs after this = overly sensitive [Post semicircular canal] on the side being lowered. = Positional Vertigo

Nystagmus are __ ___ ___ that have both _ and __ components (but during test refers to ___ component only) *There are 3 types*
B1. [Induced CALORIC Nystagmus] is when irrigation of the ____ ___ ____with warm/Cold water creates___ _____ in the ____ _____. This as a result stimulates ______ by ______
B2: What does [Cold water vs. Warm water] do during Nystagmus testing? What test is used for this?
C: What does the [Induced CALORIC Nystagmus] test for? (2)
Nystagmus are OSCILLATING EYE MOVEMENTS that have both slow and Fast components (but test refers to Fast component only) .
B1. [Induced CALORIC Nystagmus] is when irrigation of [External Auditory Canal] with Cold/Warm water creates convection currents in Vestibular labyrinths—>stimulates [crista ampullaris] by deflecting stereocilia
B2: COWS (ENG-Electronystagmogram)=
- *C**old Water—>Eyes move Opposite direction of irrigation
- *W**arm water –>eyes move in Same direction of irrigation
C: test function of individual semicircular canals (ESPECIALLY LATERAL CANAL) & [Brainstem normality]

A: Why is having a Complete Circle of Willis so important
B: Name 3 important Circle Of Willis collaterals
A:[Ischemic infarct] 2º to [Cerebral a. occlusion] can be circumvented if competent [Circle of Willis] collateral circulation detours inadequate blood flow.
B: Example: If Internal Carotid becomes occluded….Collaterals =
1) Basilar a. (via PCA and PICA)
2) [Ipsilateral External Carotid a.] (retrogradely from ophthalmic a.) perfusing [Intracranial Internal Carotid A.]
3) [CTL Internal Carotid a.] (via ACA and AICA)

A: Define [TIA-Transient Ischemic Attack]
B: What usually causes it?
C: [Carotid-area TIA] manifestation (2)
D: [Vertebrobasilar-area TIA] manifestation (2)
A: Reversible Stroke with sx that resolve in a [less than 24 hour period (usually 10-20 min.)] = 3rd leading Cause of Death in Developed countries!
B: Embolus (fibrin vs. platelets vs. cholesterol)
C:
- [Amaurosis Fugax monocular blindness] (lowered dark shade)
- Hemispheric syndromes (aphasia & hemiparesis)
D:
- [Brainstem vs. Cerebellar] ataxia & diplopia
- Homonymous Hemianopsia

Name the most common Cardiac sources of Emboli to Large Arteries (5)

A1: Radiographic evaluation of any Cerebral Ischemic Infarct (2). Why?
A2: Vascular evaluation of any Cerebral Ischemic Infarct (2)
A3: Cardiac evaluation of any Cerebral Ischemic Infarct
B: What else should be done to work this up (2)
C: List Other DDx with similar presentation (4)
(TIA vs. [Cortical Large Artery Ischemic Infarction]**)
A1:
1st Choice: [Brain MRI] = confirms suspected vascular territory involved if infarct occurred
2nd Choice: CT
A2: [Carotid US vs. MR/CT/Catheter Angiogram]
A3: Echocardiograph
B: Also Determine sources of emboli and other infarct causes
C:[Atypical tumor] vs. Hemorrhage vs. Abscess vs. Encephalitis
A: What pathology is depicted in image?
B: MOD
C: Describe the associated syndrome with this pathology (2)

A: Multiple Lacunar Infarcts
B: Lacunar Stroke= ischemia of lenticulostriate vessels –> [cystic infarcts < 1.5 cm (mostly seen with MRI)] –> Lacunar Syndrome
C: Lacunar Syndrome:
- lenticulostriate vessels perfuse [Be TIPC]*
1) Lacunar Stroke= ischemia of lenticulostriate vessels –> [cystic infarcts < 1.5 cm (mostly seen with MRI)] –> Lacunar Syndrome (listed below)
1A: [Internal Capsule/Pons/Corona Radiata] Stroke–> pure Motor stroke (ataxia vs. hemiplegia vs. clumsy hand)
1B: ThalamuS Stroke –> pure Sensory stroke
1C: Basal Ganglia - not included in Syndrome
Note: Lacunar lesions may be WITHOUT sx

A: [Acute Cerebral Infarction] 1st line tx (2)
B: What tx is used if 1st line tx is not available? (2)
C: What other management should be done (3)
A: Thrombolytic Drugs (tPA)
- [IV tPA within 3 hours of stroke onset]
- [intraArterial tPA] to break up clot in stroke center
B: Antiplatelet drugs (or anticoagulant drugs in RARE situations)
C:
- Control BP!!
- Control Hyperglycemia
- Control other complication (edema / sepsis)
A: Which Rx is given to prevent Cardiac Emboli (especially from aFib) (2)
B: Rx given to prevent [TIA/Small vs. Large cerebral ischemic infarct] (3)
C: What are 2 other good preventative Rx for Cerebral Ischemia. Which has caveots? Describe the caveot.
A: Heparin vs. Warfarin = AntiCoagulants
B: [ASA vs. Clopidogrel vs. Dipyridamole] = AntiPlatelets
C:
- Control Atherosclerosis
- Carotid Endarterectomy (only for symptomatic-flow limiting [NON-Cranial Internal Carotid A.] with 70-99% Stenosis)
Cerebral Hemorrhage
A: List Causes (6)
A2: Which is MOST COMMON and where does it affect (2)
B: Sx (3). Which Sx helps to differentiate Cerebral Hemorrhage from Infarct
C: Radiographic scan used to diagnose
High arterial pressure –>blood rupture into brain

A: “Can’t hear yo CHATTA, if I’m Bleeding in Ma Brain!”
1) [HTN-Uncontrolled] = MOST COMMON (can also be from illicit drugs). Affects basal ganglia & thalamus most commonly
2) Trauma
3) [Coagulopathy DEC] (usually accompanied with systemic bleeding)
4) [AVM rupture]-Use angiography to visualize
5) [Tumor vs. Ischemic Infarct]
6) [Amyloid Angiopathy in Elderly]
B: [Early impairment of consciousness] is not usually associated with infarct. + HA + [INC ICP/edema –> potential local ischemia]
C: CT Scan (since it’ll show location & severity)
A: What Afferents travel TO the Thalamic [Lateral Geniculate] nc. (2)
B: Where does the Efferent fibers of the Thalamic [Lateral Geniculate] nc. project to?
C: What type of Thalamic nucleus is the [Lateral Geniculate]
[Lateral Geniculate nc.] “L for Light! “
A: Aff= Optic Tract & [SUP colliculus] –> nc
B: Eff= nc—> [Area 17 CPVC]
C: [Specific Relay nuclei]
A: What Afferents travel TO the Thalamic [medial Geniculate] nc.
B: Where does the Efferent fibers of the Thalamic [medial Geniculate] nc. project to?
C: What type of Thalamic nucleus is the [medial Geniculate]
[medial Geniculate nc.] “M for Music”
A: Aff= [inf colliculus] –> nc
B: Eff= nc—> Primary Auditory Cortex
C: [Specific Relay nuclei]
A: [Lower Motor Neurons] are Motor neurons of the ___ & _____ They are arranged into 4 columns and release ____ onto _____ receptors of ____ _____ Lower Motor Neurons are recruited based on __ & ____
B: What are the 4 Column Arrangements and which muscles do they innervate?
A: Lower Motor Neurons are Motor neurons of the Brainstem & Spinal Cord.
They are arranged into 4 columns and release ACETYLCHOLINE onto nicotinic receptors of target m.
Lower Motor Neurons are recruited based on size & Force
B: 4 Column Arrangement:
- medial LMN–>axial trunk m.
- Lateral LMN—>Distal Limb m. (extremities)
- Dorsal LMN—>FLEXORS
- venTral LMN——->exTensors
A: Cells of Origin for [Area 4 precentral gyrus] are called the ____ ____ ____. So…Corticospinal Tract is AKA ____ Tract
B: CST starts in _______—>forms ___ ____—>which travels in _____ Capsule—-> _________ —>________ inside Pons —–> decusates in ___ _____—(travels in) –>____ ______ as the ________—> synapse on [ANT horn cells]
C1: 10% of CST fibers DON’T CROSS AT [___ ____] These are called the ____
C2: These ______ cross over at diff levels of the __ _____to still synapse on contralateral [ANT horn cells] like the _________
D: CST Fibers are ____[Upper/lower] Motor Neurons and is the ___[smallest/Largest] Descending Tract
E: CST is used for what type of movements?
A: Cells of Origin for [Area 4 precentral gyrus] = [Pyramidal Betz Cells]
So…Corticospinal Tract is AKA Pyramidal Tract
B: CST starts in [Area 4 precentral gyrus]—>forms [CORONA RADIATA]—>travels in [Posterior limb: Internal Capsule]—-> [Crus Cerebri Cerebral Peduncle] —>[Base of the Pontine Gray] —–> decusates in medullary pyramid—(travels in)–>[Lateral funiculus] as the [Lateral CST]—> synapse on [ANT horn cells]
C1: 10% of CST fibers DON’T CROSS AT [medullary pyramids= [ANT CST] .
C2:[ANT CST] crosses over at diff levels of [Ventral Funiculus] to still synapse on contralateral [ANT horn cells] like the [Lateral CST]
D: CST Fibers are Upper Motor Neurons and is the LARGEST Descending Tract
E: CST is used for [Fine motor movements] like piano playing/picking up pennies

A: Corticospinal Tract originates and terminates from ___origins and consist of __[#] fibers. 50% of it comes from ______ while other 50% comes from _______
B: CST projects to the __ ___&; _____. Its collaterals (both direct & indirect) travel to_____, ____, ______ and _____
C: CST Passes through the ____ limb of ____ _____
A: Corticospinal Tract has MULTIPLE origins and terminations and consist of ~1 million fibers.
50% of it comes from Primary motor cortex while other 50% comes from areas [Adjacent Frontal motor and Parietal areas]
B: The CST projects to [Brainstem & Spinal Cord]. Its collaterals (both direct & indirect) travel to basal ganglia, thalamus, [reticular formation of midbrain] and sensory nuclei
C: CST Passes through POSTERIOR limb of Internal Capsule

A: Define Coma
B: Coma prognosis (3)
C: [Irreversible Brain Death]
- cause (2)
- Dx
- caveot
A: Sleep like [unarousable (not alert/awake even after pain) vs. unresponsive] state where cortex is not functioning
B:
- Reversible (only if treated in time and after a reversible cause)
- Minimal Return = [Days-weeks post cerebral anoxia] pt may appear awake + [roving eyes] + [pain response] but still no real interaction = Persistent Vegetative State
- [Irreversible Brain Death]:
- mostly from progressive edema & neuron death and can be declared even with heart beat
* -Dx at least 6 hour observation of no imprvmnt + Absent Cerebral blood flow over 10 min on brain scan*)
- (Caveot: Muscle reflexes & Babinski can be present in Coma Dx)
A: [Ascending Reticular Activating System] or ARAS plays a role in _______, _______& _______. It helps to _______ the Cerebral Cortex.
B: Other “candidates” that Activate Cerebral Cortex are the…[3]
C: Why does the Cerebral Cortex project TO the [Reticular Formation]?
A: [Ascending Reticular Activating System] or ARAS plays a role in level of alertness, [sleep-wake] rhythms & “Startle” rxns. It helps to Activate the Cerebral Cortex.
B: Other “candidates” for activating Cerebral Cortex…
1. Basal forebrain—>[Basal nucleus of Meynert]—->ACH
- [Orexin of LAT Hypothalamus]—->tuberomammillary body and STABILIZES WAKE STATE
- Cholinergic neurons near [locus ceruleus]
C: Motor Cortex, influences alertness and allows focusing of attention
A: Orexin comes from the [_______ Hypothalamus] and is responsible for _______. It makes sure _______ states are TURNED OFF!
B: Narcolepsy occurs when _______
B2: What is Cataplexy?
C: What are these caused by?
D: The part of the Hypothalamus Orexin is synthesized in was previously considered the ____or ____ center
A: Orexin comes from the [Lateral Hypothalamus] and is responsible for STABILIZING WAKE STATE. It makes sure REM/Non-REM states are TURNED OFF!
B: Narcolepsy occurs when pt randomly falls asleep and IMMEDIATELY enters REM Sleep.
B2: w/ Cataplexy: sudden episode of REM-like muscle Weakness but during FULL CONSCIOUS AWAKEFULLNESS
C: Cataplexy is caused by Autoimmune dz: Body destroying Orexin Neurons
D: LATERAL Hypothalamus was previously considered the FEEDING or PLEASURE center
Name the common causes of Coma (2)
- [Upper Brain Stem lesions that interupt (ARAS-Ascending Reticular Activating System]
- [Bilateral Extensive Cerebral Cortex Damage]
a: Unilateral Cerebral lesion –> Edema which affects CTL hemisphere vs. herniation compresses ARAS
b: Toxic changes (Drugs vs. anoxia) –> DIFFUSE DAMAGE
A: How should you initially examine an Unresponsive pt (4)
B: Describe the MOTOR testing (5)
A: Examine [Brain Stem Reflexes] (ME then PB = Motor vs. Breathing vs. Pupils vs. Eye mvmnt)
Motor testing
- Withdrawal to pain = some cortical function
- [DecorTicate posturing (UE Flexion & LE Extension)] = Cerebral Hemisphere damage
- [Decerebrate posture (ALL EXTREMITIY EXTENSION)] = [Midbrain Red Nucleus lesion]
- [Myoclonic jerks & Asterixis] = [Toxic metabolic coma]
- [Spontaneous Nystagmus & Twitching] = [Coma 2° to electrical status epilepticus]
A: How should you initially examine an Unresponsive pt (4)
B: Describe the Eye Movement testing (2)
A: Examine [Brain Stem Reflexes] (ME then PB = Motor vs. Breathing vs. Pupils vs. Eye mvmnt)
Eye Movement testing = Both Test indicate Normal Brain Stem
- [Oculocephalic Doll’s Eyes Reflex] = eyes conjugately move in direction opposite from head rotation (normal brain stem response) - RULE OUT CERVICAL SPINE FRACTURE BEFORE DOING THIS
- [Induced CALORIC Nystagmus] is when irrigation of [External Auditory Canal] with Cold/Warm water creates convection currents in Vestibular labyrinths—>stimulates [crista ampullaris] by deflecting stereocilia
- COWS (ENG-Electronystagmogram)=
- *C**old Water—>Eyes move Opposite direction of irrigation
- W**arm water –>eyes move in Same direction of irrigation

A: How should you initially examine an Unresponsive pt (4)
B: Describe the PUPIL testing (5)
A: Examine [Brain Stem Reflexes] (ME then PB = Motor vs. Breathing vs. Pupils vs. Eye mvmnt)
Pupils testing
- Pupil Dilation (hypothalamus–>brain stem–>spinal cord–> sympathetic ganglia)
- Pupil Constriction (Oculomotor CN3 & Parasympathetics)
- Pupillary Light Reflex (Doesn’t rule out Metabolic Coma)
- Small Pupils ([Narcotics/Glaucoma Cholinergic Eyedrops] vs. [Normal in Awake Elderly]
- [Unilateral Large Pupil] (possible Oculomotor CN3 compression from uncal herniation) = EMERGENCY!!!

A: How should you initially examine an Unresponsive pt (4)
B: Describe the BREATHING testing (3)
A: Examine [Brain Stem Reflexes] (ME then PB = Motor vs. Breathing vs. Pupils vs. Eye mvmnt)
Breathing testing
- Cheyne-Stokes = alternating tachypnea & apnea from bilateral cortical lesions vs. HF vs. sleeping elderly
- Hyperventilation = mostly from pulmonary congestion
- [Irregular Ataxic] = Lesion at/near [medullary cardiopulmonary control] –> impending respiratory failure
Emergent Evaluation of a Comatose pt should include what 4 Steps
1st: ABC = Airway / Breathing / Circulation
2nd: Check Blood-glucose –> Give [50% IV Dextrose] if necessary
3rd: W/u for Toxi-metabolic coma (don’t forget CO poisoning and hypOthermia) - Myoclonic Jerks & Asterixis
4th: W/u for Structural Coma (hemorrhage / tumor / infarct) = hemispheric abnormalities
A: Describe the Persistent Vegetative State
B: Are Cranial Nerve Reflexes still intact?
C: In a Vegetative State, which neural structures are still intact? (2)
D: What does this progress from?
Pt is Arousable but not really responsive
A: [Days-weeks post Cerebral Cortex anoxia] pt may appear awake + [roving eyes] + [pain response] but still no real responsiveness = Persistent Vegetative State
B: Some CN reflexes may still be intact (Brainstem & Spinal Cord are still intact)
C: Brainstem & Spinal Cord
D: Coma –> Minimal Return
A: Describe the Demented pt
B: How do you approach Advanced Directives for these pts
C: What is their Nutritional Status (2)
A: Pt who is progressively becoming [unaware of problems] and [unable to understand/communicate], typically associated w/behavioral changes
B: Establish Directives early! (since family will eventually assume all decision-making)
C: [Olfactory Dysfunction] –> No Appetite, but pt will still have “basic need” to hydrate. Tx= [PEG-Percutaneous Endoscopic Gastrostomy] vs. feeding tube
A: The SCN [Suprachiasmatic Nucleus] is located Above _____ _______ and is used as our ___ ___ ____& ___ _____. It keeps us on a _______. This is 1 of the nucleus from the _____.
B: What type of EXTERNAL input does the SCN receive? [3]
C: What internal Output does it send out?
D: Biologic Rhythms by the SCN are not linked exclusively to the _____ and works together with ___ _____. Name the 4 Categories, describe their timing and give example
E: When does SCN secrete the MOST hormones?
A: The SCN [Suprachiasmatic Nucleus] is located Above Optic Chiasm and is used as our endogenous “biological clock” & CIRCADIAN Pacemaker. It keeps us on a 24 hour cycle, turning some systems on/off. This is a nucleus of the HYPOTHALAMUS.
B: Light (reason its near Optic Chiasm), Food & Temperature
D: Biologic Rhythms by the SCN are not linked exclusively to the HIPPOCAMPUS. It works together with Environmental Cues. These are the 4 Categories:
- Ultradian = less than 24 hours –>Resp/HR
- Circadian = 24 hours —>Corticosterone rhythm
- Infradian = More than 24 but less than 1 year–>menstrual cycles
- ## Circannual= every year—> HibernationE: Highest amount of SCN hormone secretion = When ur Sleep
A: Disconnection syndromes usually result from _______ matter damage interfering with ____ ___ or ___ ____
B1: Define Alexia
B2: Define Agraphia
B3: Lesions in [NON**-Dominant Hemispheres of cortical language center] –> ____
C: AWA is usually caused by _______ stroke to _______ Lobe. ___ ____ of this area is affected
A: Disconnection syndromes usually result from WHITE matter damage interfering with Corpus Callosum or ANT commissure.
B:
- Alexia = impaired reading (visual cortex is disconnected from language center)
- Agraphia= impaired writing (motor cortex for dominant hand is disconnected from language center)
3: [NON-Dominant Hemisphere lesions] in the [mirror image locations of cortical language center]–> Aprosody (inability to interpret the [TIP-Tone/Inflection/Pitch] of language)
C: [Alexia without Agraphia] is usually caused by PCA stroke to Occipital Lobe. Corpus Callosum of this area is affected—>Seeing object in L eye CAN’T be interpreted in the R brain like normal.
Describe**:
A: HemiBallismus
B: HuntIngtons
C: Parkinsons
A: Lesion of [SubThalamic Nucleus] –> less Stimulation of [Globus Pallidus: internal] –> HYPERKinesia (specifically VIOLENT limb flinging)
B: HuntIngton’s = [Auto Dominant Degeneration of ((_I)_ndirect Striatum) 2° to [Chromo 4 trinucleotide repeats]] “Hunter was way too excited”
C: Parkinson’s = [Degeneration of (Substantia Nigra:Compact) = Loss of All Dopamine]
DDEM = Dopamine & [Direct Path] Enable Movement

A: [Chorea and Dystonia] are SE of Dopamine _____ [blockers vs. agonist]
B: Name 4 Movement Disorders that are unrelated to Basal Ganglia
C: Name the 5 components of the Basal Ganglia
A: A: [Chorea and Dystonia] are SE of Dopamine AGONIST
B:
- Essential Tremor
- [Myoclonus vs. Asterixis (ToxiM**etabolic etiology)]
- Dystonia
- Tic
C: [Caudate / Putamen / [Globus Pallidus] / [Substantia Nigra] / [SubThalamic Nucleus]]

A: Primary Clinical Signs of Parkinsonism (4)
B: Secondary Clinical Signs of Parkinsonism (3)
A: PARK & ham
- [Pill Rolling Resting Tremor]
- [Rigidity Cogwheel]
- BradyKinesia
- [AReflexia posturally] –> Fall
B:
- hypOphonic speech
- Autonomic Dysfunction (constipation / bladder problems / orthostatic hypOtension)
- micrographia

A: Causes of Parkinsonism (4)
B: Age of onset
C: Dx (2)
D: Histology

A:
1) Parkinson’s Dz
2) [Rare Degenerative Disorders (progressive supranuclear palsy vs. multiple system atrophy)= NOT responsive to levodopa
3) [Dopamine Blocker (Haloperidol) SIDE EFFECTS]
4) [Manganese vs. Carbon Monoxide Poisoning]
B: onset between 40-70 y/o
C: [2 or more Primary Clinical Signs — typically worst on 1 side and progressive] + [Responds to Dopaminergic tx]
D: Lewy Bodies = [alpha synuclein cytoplasmic accumulations tht are eosinophilic]

A: Parkinson’s Dz Tx (5)
B: Describe the 3 aspects of Surgical tx specifically
“Eat a SALAD after you Park”
- [Levodopa (Dopamine Precursor)]
- Amantidine (weakly stimulates Dopamine release)
- Anticholinergics (WEAK effect)
- [Dopamine Agonist Post synaptic] (Ropinirole vs. Pramipexole): Also has ability to [DEC Long term Dyskinesia if given as monotherapy]
-
Surgical tx
- Used in Pts refractory to meds
- Pallidotomy: Intential Destructive Lesion of the [Globus Pallidus:internal]
- SubThalamic nuc. inhibition with implanted electrode
Levodopa
A: What is Levodopa co-administered with and why?
B: Describe How Long Levodopa has an effect. What can be given to mitigate this? (2)
C: Side Effects (4)
Levodopa = Parkinson’s Dz tx
A: Administered with Carbidopa (decarboxylase inhibitor), which prevents peripheral Levodopa catabolism before it has chance to enter brain
B: DEC over time since there will continue to be dopaminergic neuron death. [MAO-B and COMT-_inhibitors_] sustain effective Levodopa levels
C:
[Hallucinations vs. Psychosis vs. Chorea vs. DysTonia]
Lewy Body Dementia
A: Statistics
B: Clinical Course (2)
C: Describe the Histology. What parts of the brain is it found in (2)?
Lewy Body Dementia is the SECOND common type of neurodegenerative dementia
B: [Dementia + Visual Hallucinations] –> [Parkinsonian sx]
C: [alpha synuclein cytoplasmic accumulations tht are eosinophilic] - found in Cortex & Brainstem

Frontotemporal Degeneration
A: Statistics
B: Clinical manifestation
C: Genetic Cause
D: Dx (3)
A:[Frontotemporal Degeneration] is the THIRD common type of neurodegenerative dementia BUT MAY BE CONCOMITANT WITH ALZHEIMER’S. Typically worst on Left.
B: Change in personal/social conduct, associated with disinhibition and language changes
C: [Chromo 17 Tau gene mutation]
D: Immunohistochemistry against: [Tau vs. Ubiquitin vs. TDP43]
A: Categorize Pick’s Dz
B: Clinical Presenation
C: Histology
D: What 2 neural structures are associated
A: RARE SubType of [Frontotemporal Dementia]
B: Aphasia (minimal memory loss but may develop Dementia)
C: Pick Bodies = Globose neuronal cytoplasmic inclusions made of Tau.
D: Hippocamps and Cortex
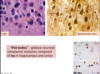
Huntington’s Dz
A: Genetic Cause
B: What effect does Caudate nc. degeneration have? (2)
C: In this Dz, what actually causes Neuronal Death?
A: HuntIngton’s = [Auto Dominant Degeneration of ((I)ndirect Striatum) 2° to [Chromo 4 trinucleotide repeats]] “Hunter was way too excited”
B: [Degeneration of Caudate nc.] –> [DEC GABA and ACh]
C: [NMDA-R binding and Glutamate]

[Multiple System Atrophy]
A: onset
B: Sx (3)
C: Histology
A: 40-60 (Parkinson’s Dz Onset = 40-70)
B: Atrophy of COPS
- Parkinsonism -Substantia nigra atrophy
- Cerebellar Ataxia - Cerebellar atrophy
- Autonomic dysfunction -[Olivary nc./Pons atrophy]
C: [GLIAL alpha synuclein cytoplasmic accumulations tht’s eosinophilic]
Friedreich’s Ataxia
A: Statistics
B: Genetic Cause
C: Clinical Manifestation (3)
[FriedreiCH’S Ataxia]

A: Most common Hereditary Ataxia
B: [Auto recessive GAA Trinucleotide repeat in Chromo 9 Frataxin gene] Frataxin is needed for mitochondrial iron
C: [FriedreiCH’S Ataxia]
- [Cerebellar Degeneration]–> Ataxia
- Heart Abnormalities –> 50% of deaths!
- [Spinal Cord Degeneration] –> [Loss of 2TVP] + [Muscle Weakness] + [Loss of Deep Tendon Reflex]
A: Mixed Dementia mostly consist of _____ & [Vascular Dementia]
B: What are Risk Factors for Mixed Dementia (2)
C: What is the most common form of [Vascular Dementia]
A: Mixed Dementia mostly consist of Alzheimer’s & [Vascular Dementia]
B:
1) [ApoE4 genotype] INC risk of Alzheimer’s AND CV Dz
2) Vascular Amyloidosis INC risk of hemorrhagic strokes –> [Vascular Dementia]
C: CADASIL = involves small arterioles & capillaries
[Ethanol Tox: Wernicke’s Syndrome]
A: Clinical Triad (3)
B: This syndrome is characterized by deficiency of what substance?
C: What supplement deficiency is this syndrome caused by?
TACO

A: Thiamine deficiency —>
- Oculomotor abnormalities (ophthalmoplegia vs. nystagmus)
- Cerebellar Dysfunction
- Altered Mental Status
B: [+/- Korsakoff Psychosis from mammillary body hemorrhage & atrophy (can’t recall recent memory so compensates with confabulation)]
C: Thiamine Deficiency
A: Toxicity of what compound causes
[Cortical Atrophy] and [Central Pontine Myelinolysis]
B: [Central Pontine Myelinolysis] Histology
C: What Electrolyte abnormality causes [Central Pontine Myelinolysis] ?
A: ETHANOL TOXICITY

B: Triangular lesion with myelin loss of the Pons
C: [Rapid Correction of Chronic hypOnatremia]
Methanol Toxicity
A: MOD (3)
B: Clinical Manifestation (4)
A: Hepatic oxidation of [Methanol –> (Formaldehyde & Formic Acid)]–>
- global hypoxia
- white matter necrosis & hemorrhage–> [Putamen & Claustrum hemorrhagic infarct]
B: [Vision loss vs. Delirium/Convulsions vs. Coma vs. Death]

Gross Histology of Carbon Monoxide Toxicity (3)
- [Bilateral Globus Pallidus Hemorrhagic Necrosis]
- [White Matter Hemorrhagic Petechiae]
- Cerebral Edema

A: Identify and Describe Histology of image
B: Cause

A: [Alzheimer Type 2 Astrocyte] = [Nuclei are large and appear clear]
B: liver Failure–> Hyperammonemia (Hepatic Encephalopathy)
A: Speech consist of ____ and ____
B: Describe each component of Speech
C: Define Aphasia
A: Speech = Phonation and Articulation
- Phonation: making sounds with vocal cord mvmnt (Vagus CN10) - (Dysphonia = Hoarse vs. whispery)
- Articulation: articulating sounds with [lips/tongue/palate/pharynx] (Dysarthria = slurred speech 2º to Articulation problems)
B: Disorder of [previously acquired language ability] due to [language center lesion in dominant hemisphere] –> all-around impaired communication (includes gestures & Braille)
A: Where are the Cortical Language Centers
B: what perfuses this center
C: Describe the Function of Wernicke and Broca area
D: Lesions around this Center leads to what guaranteed defect?
A: [Sylvian Lateral Sulcus] of the dominant (usually L hemisphere**) hemisphere
B: MCA
C:
1) Wernicke’s area = language comprehension
2) Broca’s area = language execution/expression
D: Imperfect Repetition
A: Paraphasia definition
B: Examples (3)
[Word or Syllable Substitutions]
- Phonemic or literal = Sully for Silly
- [Semantic or verbal]= blue for Green
- -*Neologism= nonsense word: scatifang
Broca’s Aphasia
A: Location of Lesion (2)
B: Clinical Manifestation (5)
A: [Area 44 Inferior Frontal Gyrus] + [involvement of adjacent motor cortex]
B:
- [Poor Repetition/Naming/Fluency ([telegraphic nonfluency ( “I…..up…..early”)]]
- R Hemiparesis
- Facial Weakness

Wernicke’s Aphasia
A: Location of Lesion
B: Clinical Manifestation (4)
C: What Dx is this sometimes confused with?
A: [Temporal Lobe (posterior vs. superior)]
B:
- [Poor Repetition/Naming/Comprehension (They don’t comprehend you and You can’t comprehend them)]
- Hemiparesis
C: Psychiatric disorders

Conductive Aphasia
A: Location of Lesion
B: Clinical Manifestation
A: [Arcuate Fasciculus (tract between Broca & Wernicke)]
B: [Intermediate version of Wernicke**’s Aphasia]

GLOBAL Aphasia
A: Location of Lesion (3)
B: Clinical Manifestation (3)
A: [Broca + Wernicke + Arcuate Fasciculus] = ALL!
B: [SEVERELY NONFLUENT / MUTE / poor comprehension]

A: Define Prosody
B: Lesions of which area –> AProsody
C: Name the 2 Types of AProsody
A: [Semantic & Emotional meaning] conveyed by the [TIP-Tone/Inflection/Pitch] of Language
B: [Nondominant Hemisphere lesions] in the [mirror image locations of cortical language center]
C:
- [Sensory Receptive Aprosodia] - [NonDominant Wernicke’s lesion]
- [Motor Expressive Aprosida] - [NonDominant Broca’s lesion]
[Sensory Receptive Aprosodia]
A: Location of lesion
B: Clinical Manifestation (3)
A: [NonDominant Wernicke’s lesion]
B: Speaks with Prosody but has [Poor prosodic comprehension when listening] and [unable to repeat prosody in others’ speech]
[Motor Expressive Aprosodia]
A: Location of lesion
B: Clinical Manifestation (3)
A: [NonDominant Broca’s lesion]
B: DOES NOT SPEAK with Prosody and [unable to repeat prosody in others’ speech] but has [Good prosodic comprehension when listening]
A: Describe Gait Apraxia
B: Describe Constructional Apraxia. What lesion causes this?
A: Pt are only unable to walk when commanded to walk, even though they have all the essentials to walk intact
B: PARIETAL LOBE LESION –> pt unable to draw when commanded to draw
Apraxia is not due to sensory/motor/language deficit
A: WhatType of Ataxic Gait is in image
B: Location of Lesion causing this (2)

A: [Broad-based Ataxic Gait]
B:
- [Dorsal Column and its associations]
or
- [Cerebellum (Gait is constantly bad regardless of eyes open/close)]
A: WhatType of Ataxic Gait is in image
B: Location of Lesion causing this

A: [Hemiplegic Ataxic Gait]
B: Stroke
UE: [Upper limb flexed at elbow + DEC armswing] on affected side
A: Describe [Tabetic Ataxic Gait]
B: Associated Diseases (2)
A: [Stomping foot gait] where pt forcibly plants feet down on ground to “feel” floor & compesnate for impaired sensation
B:
- [Tabes Dorsalis Neurosyphilis]
or
- [Severe Neuropathy]
A: WhatType of Ataxic Gait is in image
B: Causes (3)

A: [Steppage Ataxic Gait]
B:
- [peroneal n. lesion]
- [L5 root lesion]
- Peripheral Neuropathy
to prevent tripping over the toes, the hip is flexed even higher to elevate the drooping foot, which is lowered to the floor toe first
A: Describe [Waddling Ataxic Gait]
B: Associated Disease
A: [Pelvic vs. Hip muscles] can’t support body when on 1 leg so swaying/leaning when foot is raised helps = alternatively wadduling like a duck!
B: Myopathy
A: WhatType of Ataxic Gait is in image
B: Location of Lesion causing this
C: Disease Associated (2)

A: [Scissors Ataxic Gait]
B:
- CST lesions–> [spastic paraparesis]–>tightness in adductor muscles and knees–>legs cross over each other like scissor blades
C:
- Cerebral Palsy
- Multiple Sclerosis
A: WhatType of Ataxic Gait is in image
B: Disease Associated
C: Describe this gait

A: [Parkinsonian Ataxic Gait]
B: Parkinson’s
C: [Slow shuffling gait] with Stooped forward posture and festination (leaning more & more forward to walk and then runs to catch up with center of gravity). Falls a lot.

Cerebellar Function Test:How do you use….
A: Speech
B: Eye mvmnts
C: Limb (4)
A: Dysarthria = slurred speech 2º to Articulation problems
B: [Nystagmus with erratic, jerky mvmnt]
C:
- Kinetic Tremor (rhythmic oscillations during limb mvmnt)
- Dysmetria (overshooting/undershooting target)
- Mvmnt Decomposition (jerky and broken down)
- [Rebound Check response Deficit] (sudden release of contracted triceps from loss of check response from antagonist muscle–>pt hits himself)
A1: Describe Hemispheral Syndrome
A2: Cause
B1: Describe Vermal Syndrome
B2: Cause (2)
A1: Ipsilateral Limb [kinetic tremor/dysmetria/rebound check response loss]
A2: Any Bilateral lesion in degenerative dz (MS)
B1: TRUNK [truncal unsteadiness with standing / walking / gait ataxia]
B2:
- Alcoholic Cerebellar Degeneration (ANT SUP vermis atrophy)
- Any Bilateral lesion in degenerative dz
Spinocerebellar Degeneration
A: Most common type
B: Pgn
A: [Friedreich’s Ataxia]
B: No curative tx and Older pts become wheelchair-dependent
[Cerebellar and Spinal Cord Nc. and tract are affected]
A: Describe Choreoathetosis (2)
B: What areas are affected (3)
C: Causes (2)
A:
[slow continuing limb movements= Athetosis]
+
[Irregular dancelike movements = Chorea]
B: Limb, trunk and face
C:
- [Caudate nc. lesion (Huntington’s Dz)]
- [Dopaminergic medications]
A: Describe Tics
B: What disorder is this associated with?
A: Brief repetitive contractions of muscle groups (facial twitch vs. eye blink vs. sniffs vs. grunts)
B: Tourette’s (inherited with variable penetrance-mostly boys)
A: Describe Myoclonus
B: Causes (2)
A: Asynchronous rapid shocklike mvmnts of limbs or body bilaterally
B:
- Diffuse Encephalopathy (Creutzfeldt Jakob Dz)
- Medical Dz (Renal/Hepatic Failure vs. Anoxia)
A: Describe Asterixis
B: Causes (3)
A: Flapping Tremor of hand/foot from [postural tone loss] typically bialterally
B:
- Diffuse Encephalopathy (Creutzfeldt Jakob Dz)
- Medical Dz (Renal/Hepatic Failure vs. Anoxia)
- Structural brain lesions - will be Unilateral
Tx for…
A: Essential Tremor (2)
B: Dystonia (3)
A: [Beta blockers vs. Barbiturates]
B: [Anticholinergics vs. Benzodiazepines vs. Botox]
A: [Thalamic RETICULAR nucleus] projects ONLY to _____ and NOT the _____. Neurons of this nuclei are ___ _____.
B: Thalamic Axons passing thru (incoming & outgoing) give off ____ which travel to [Thalamic RETICULAR nucleus].
C: Main Purpose of [Thalamic RETICULAR nucleus] is to inhibit _____ and therefore Enhances activity of _______
[Thalamic RETICULAR nucleus] projects ONLY to other thalamic nuclei and NOT the Cerebral Cortex. Neurons of this nuclei are [inhibitory GABAergic].
B: Thalamic Axons passing thru (both incoming & outgoing) give off collaterals to [Thalamic RETICULAR nucleus].
C: Main Purpose of [Thalamic RETICULAR nucleus] is to inhibit random background sensory activity —> Enhances salient activity of 1 area of thalamic neurons.
A: What Thalamic Afferents travel TO the [ANTERIOR nc.]? [2]
B: Where does the Efferent fibers of the [ANTERIOR nc.] project to?
C: What type of Thalamic nucleus is the [ANTERIOR nc.]
[ANTERIOR nc.]
A: Aff= Mammillary body & Hippocampus —> nc
B: Eff= nc—> projects to Cingulate Gyrus
C: [Specific Relay nuclei]
A: What Thalamic Afferents travel TO the VA[VENTRAL Anterior nc.]?
B: Where does the Efferent fibers of the [VENTRAL Anterior nc.] project to?
C: What type of Thalamic nucleus is the [VENTRAL Anterior nc.]
[VENTRAL Anterior nc.] A: Aff= Basal ganglia ( [substantia nigra] ) —> nc
B: Eff= nc—> projects to PreFrontal Cortex
C: [Specific Relay nuclei]
A: What Afferents travel TO the Thalamic [VL>ant] nc. B: Where does the Efferent fibers of the Thalamic [VL>ant] nc. project to? C: What type of Thalamic nucleus is the [VL>ant]
[VENTRAL Lateral nc.]>ANT part (VL>ant)
A: Aff= Basal ganglia ([Globus Pallidus])—> nc
B: Eff= nc—> projects to Supplementary motor area C: [Specific Relay nuclei]
A: What Afferents travel TO the Thalamic [VL>PoST] nc.
B: Where does the Efferent fibers of the Thalamic [VL>PoST] nc. project to?
C: What type of Thalamic nucleus is the [VL>PoST]
[VENTRAL Lateral nc.]>PoST part
A: Aff= Cerebellum—> nc
B: Eff= nc—> MOTOR CORTEX
C: [Specific Relay nuclei]
A: What Afferents travel TO the Thalamic [VPM] nc. B: Where does the Efferent fibers of the Thalamic [VPM] nc. project to? C: What type of Thalamic nucleus is the [VPM] D: What type of info specifically is this Thalamic nucleus involved with?
[VENTRAL POSTEROMEDIAL nc.] A: (Somatic) Aff= Head –> nc B: Eff= nc—> Somatosensory Cortex C: [Specific Relay nuclei] D: Involved with relaying Vestibular information
A: What Afferents travel TO the Thalamic [VPL] nc. (2) B: Where does the Efferent fibers of the Thalamic [VPL] nc. project to? C: What type of Thalamic nucleus is the [VPL] D: What type of info specifically is this Thalamic nucleus involved with?
[VENTRAL POSTEROLateral nc.] A: (Somatic) Aff= [Trunk&Limbs] –> nc B: Eff= nc—> Somatosensory Cortex C: [Specific Relay nuclei] D: Involved with relaying Vestibular information
A: What Afferents travel TO the Thalamic [Lateral Geniculate] nc. (2) B: Where does the Efferent fibers of the Thalamic [Lateral Geniculate] nc. project to? C: What type of Thalamic nucleus is the [Lateral Geniculate]
[Lateral Geniculate nc.] A: Aff= Optic Tract & [SUP colliculus] –> nc B: Eff= nc—> [Area 17 CPVC] C: [Specific Relay nuclei]
A: What Afferents travel TO the Thalamic [medial Geniculate] nc. B: Where does the Efferent fibers of the Thalamic [medial Geniculate] nc. project to? C: What type of Thalamic nucleus is the [medial Geniculate]
[medial Geniculate nc.] A: Aff= [inf colliculus] –> nc B: Eff= nc—> Primary Auditory Cortex C: [Specific Relay nuclei]
A: What Afferents travel TO the Thalamic [Lateral Dorsal] nc. B: Where does the Efferent fibers of the Thalamic [Lateral Dorsal] nc. project to? C: What type of Thalamic nucleus is the [Lateral Dorsal]
[Lateral Dorsal nc.] A: Aff= Hippocampus–> nc B: Eff= nc—> Cingulate cortex C: [Specific Relay nuclei]
A: What Afferents travel TO the Thalamic [LP & Pulvinar] nc. (4) B: Where does the Efferent fibers of the Thalamic [LP & Pulvinar] nc. project to? C: What type of Thalamic nuclei are the [LP & Pulvinar]
[(Lateral POST) & Pulvinar nc.] A: Aff= [SUP colliculus]/[Area 17 CPVC]/ [Primary auditory cortex]/Somatosensory Cortex —–> nc B: Eff= nc—> {PPLTAC} “Posterior Parietal and Lateral Temporal Association Cortex” C: [Association nuclei]
A: What Afferents travel TO the Thalamic [Dorsomedial] nc. (3) B: Where does the Efferent fibers of the Thalamic [Dorsomedial] nc. project to?
C: What type of Thalamic nucleus is the [Dorsomedial]
[Dorsomedial nc.] A: Aff= [Prefrontal Cortex]/Olfactory/Limbic —–> nc B: Eff= nc—> PreFrontal Cortex
C: [Association nuclei]
A: What Afferents travel TO the Thalamic [Intralaminar] nc. (3) B: Where does the Efferent fibers of the Thalamic [Intralaminar] nc. project to?
C: What type of Thalamic nucleus is the [Intralaminar]
[Intralaminar nc.] A: Aff= [Reticular Formation]/[BasalGanglia]/limbic —–> nc B: Eff= nc—> Cerebral Cortex/[BasalGanglia]/limbic
C: [Non-Specific nuclei]
A: What Afferents travel TO the Thalamic [Thalamic RETICULAR nucleus] (2)
B: Where does the Efferent fibers of the Thalamic [Thalamic RETICULAR nucleus] project to?
C: What type of Thalamic nucleus is the [Thalamic RETICULAR nucleus]
D: What is Different of this Thalamic nucleus from the others?
[Thalamic RETICULAR nucleus]
A: Aff= Thalamus & Cortex—–> nc
B: Eff= nc—> ONLY other Thalamus nuclei
C: [Non-Specific nuclei]
D: Aside from this [Thalamic RETICULAR nucleus], All OTHER thalamic nuclei “decide” where info should go in Cerebral cortex
Intralaminar nc. and [thalamic reticular nuclei] are both types of the _______ functional group
Intralaminar nc. and [thalamic reticular nuclei] are both types of the NON-SPECIFIC functional group
Lesions of which structures typically produce Amnesia (Anterograde vs. Retrograde) (3)
“Amnesia comes from Having Memory Troubles!”
Bilateral lesions in:
-
Thalamus
2. Mamillary bodies (Thiamine deficiency-Wernicke Korsakoff)
3. Hippocampus (Herpes Encephalitis / Anoxia / Alzheimer’s)
Agnosia
A: General definition
B: Visual Agnosia
C: Tactile Agnosia
A: Failure to identify Object via 1 sensory modality, but can identify objects via others
B: Failure to visually recognize a bell but can identify when hearing or touching the bell
C: Failure to recognize bell from touch but can identify in other ways which also = [Severe Astereognosis]
Describe the Clinical Presentation of Frontal Lobe Syndrome (5)
A: Frontal Lobe has D&G on D&G
- [Disinhibition / Lack of concern]
- [Distractible motor and mental function (Poor planning & impaired creatitivity)]
- [Frontal lobe release signs in (Normal in infants only)]
- [Gegenhalten Paratonia (resistance to passive limb mvmnt)]
- Gait Apraxia

Temporal Lobe Syndromes
A: Name the Bilateral lesions (3)
B: Name the Unilateral lesions
A: Bilateral:
- Amnesia (hippocampal lesions)
- [Cortical Deafness from Auditory lesions]
- [Kluver Bucy Syndrome]
B: Dominant Hemisphere lesion: Wernicke’s Aphasia
Parietal Lobe syndromes
A: Clinical Manifestation for Nondominant Parietal lesions. List and describe 2 examples.
B: List and describe an example of Dominant Parietal Lesions. What structures are associated with this (2)?
A: Impairment of spatial relationships between body and its surroundings
- Anosognosia: Unawareness of hemiparesis or denial of an entire half of your body = Hemispatial Neglect
- Constructional Apraxia: Inability to write when commanded to
B1: “Gerstmann’s HAD a Syndrome”
Gerstmann’s Syndrome ([Hand disorientation + Finger agnosia] /Agraphia / Dyscalculia
-[Supramarginal vs. Angular Gyrus]
Occipital Lobe
A: Bilateral Lesion examples (3)
B: Unilateral Lesion examples
A:
- Anton’s Syndrome: Denial of Cortical Blindness
- Visual Agnosia
- Prosopagnosia: Inability to recognize previously known faces = subtype of Visual Agnosia
B: [Dominant TemporOccipital lesion] –> Color Anomia (inability to name colors)
