MSK/Joints Flashcards
polymyalgia rheumatica (PMR)
who is it common in? what are the lab tests like? what is commonly associated with this disease? what do you use to treat this disease? how soon can people come off it?
>50, northern european ancestry 2:1 females
abrupt onset of intense morning stiffness of neck, shoulders and hip girdle but muscle strength is normal, fatigure and anorexia also common
elevated ESR >50 mm/hr and CRP
15% can get great cell arteritis/temporal arteritis
low dose steroids 10-20 mg only drug that works, looks to normalize the CRP and ESR
usually self limiting 65% taper of steroids 1 year, 85% in 2 years
what can people develop from Polymyalgia rheumatica (PMR) and what percent of people does this happen in?
giant cell arthritis/temporal areritis
15%
what should you do if the ESR and the CRP values for polymyalgia rheumatica (PMR) don’t normalize with steroid use?
rethink the diagnosis
Systemic Lupus Erythematosis (SLE)
who is this common in? what happens? what are the four main body systems you worry about? what are the 11 presentations and how many do they need to have?
womens disease, 16-55, african american 15:1
debris from abnormal cell apoptosis promotes polyclonal B cels and autoantibodies, complexes deposit everywhere causing the symptoms
1. renal (nepthritis, nephrotic syndrome, tubulointerstitial disease)
2. neuro (seizures, psychosis)
3. hematologic (hemolytic anemia, leukopenia, lymphopenia ALL GO DOWN)
4. Immunological (vascular thrombosis) (antiophospholipid syndrome)
malar rash, arthritis without erosion just deformity, alopecia, raynauds, photosensitivity, positive ANA arthritis
must have 4/11 symptoms ANA is the only one that MUST be there
what are 8 lab tests seen in SLE?
- CBC (anemia/cytopenias)
- BUN/Cr (kidney involvment)
- UA (proteinuria/ casts)
- C3/C4 (decreased)
4. ESR ELEVATED, CRP NORMAL
5. positive ANA with all patterns EXCEPT centromere and SCL70
- dsDNA that is more specific than ANA, speckled or nucleolar
SLE treatment
- skin
- renal
- other
Skin/fatigue: hydroxychloroquine
renal: high dose corticosteroids and cyclophosphamadine (immunosuppressant)
other immuno:
azathioprine
mycophenalate
methotrexate
osteoarthritis
what is this? where is it most common? what are the two types? what would you expect to see on a xray?
joint disease with protective cartilage on the ends of your bones wears down over time and subchondral bone wears down over time >40 yrs olds THINK ELDERLY, slow developing joint pain
early onset and late onset OA, erosive
hands, hips and knees most common
primary or secondary causes
joint enlargement, red swollen PIP, DIP, weakness and wasting of muscles around joint, deformities
xray: see narrowed asymetric joint space, with osteophyte formation, bony sclerosis
what is a osteophyte? what disease is this commonly seen in?
a bony outgrowth associated with the degeneration of cartilage at joints.
osteoarthritis
what are the characteristics associated with early osteoarthrits? (4 things)
1-2 years
morning stiffness lasting
they’re ok, they say they just keep going
red, prominent PIP, DIP joints with normal radiographs
what are the characteristics associated with late osteoarthritis?
AM stiffness lasting
mechanical stiffness that gets worse with movement, more pain the more they do
claim not to have the same strength they used to (opening jars/doors etc)
little evidence of inflammation
ABNORMAL RADIOGRAPHS
get less symptomatic in non-weight bearing joints AKA many patients have extreme hand deformities but are asymptomatic (once they are deformed they don’t hurt anymore)
what is the treatment options for osteoarthritis? (7 things)
joint conservation
exercise
weight loss
NSAIDs (caution with ulcers)
COX-2 inhibitor (safer for people with history of ulcers, but still need to watch for cardiac complications)
cartilage replacement (15-55)
total joint replacement
primary osteoarthritis is…..
idiopathic, arises spontaneously
secondary osteoarthritis can come from….
- posttraumatic
- congentiral deformation
- endocrinopathy
- neuropathic arthropathy
- padgets disease
- avascular necrosis
- skeletal hyperostosis DISH
what is the most common joint disorder in the US?
osteoarthritis
Osteoarthritis of the hip
what is this? what will you see on the xray? what is the “definitive cure”? what other surgical interventions can you do in younger patients?
degredation of articular cartilage, thickening of the subcondral bone
progressive hip pain that often complain of groin pain, “crunching” noises aka crepitus
xray osteophyte formation, decreased joint space, sunchondryl sclerosis and cysts
conservative: same as always
definitive cure: total hip arthroplasty THA (replace joint)
surgical: arthroscopic debridement, femoral head resurfacing in younger patients
osteoarthritis of the knee

what is this? what are four presentations you see with this? what is a possible muscle presentation? what is the gold standard for diagnosis? what are the conservative vs surgical treatment options?
degredation of the hyaline cartilage of the knee
pain is worse in AM, giving away or locking
joint hypertrophy, and tendernous at the joint line, possivle quadricept atrophy
gold standard: xray…see osteophyte formation, decreased joint space so bone on bone, sunchondral sclerosis
treatment: conservative normals plus cortisone injections and hyaluronic acid injections
surgical: knee arthroscopy, tibial/femoral osteotomy, total knee arthroplasty

osteoarthris…explain what happens in this…
normal bone programming
“cartilage scenescence”–we outlive our chondrocytes around 25-30 years old, it frays and falls apart and the chondrocytes become hypertrophic and grow larger, however they produce enzymes MMP and aggrecanases that break down the cartilage and act like growth plate cells where THEY MAKE MORE collagen 1 and 9, BONE THAN BREAK IT DOWN…CARTILAGE CAN’T REGROW SO YOU JUST GET INCREASED BONE GROWTH!!
“progressive loss of articular cartilage and reactive changes at the joint margins from bone rubbing on sunchondral bone rubbing on bone “behaves like a fracture” and stimulates chondrocyte hypertrophy and increased bone growth

what are the common presentations of late osteoarthritis? (5)

morning stiffness lasting
mechnical stiffness, gets worse with movement, more pain the more they do
not the same strength they used to (opening jars, turning handles)
abnormal radiographs! deformities obviously present, bone hypertrophies
get LESS symtomatic in non weight bearing joints, asymatic once they are deformed because they aren’t able to move them

what are the treatment options for someone with osteoporosis?

Not much…its a natural bone programming
Its “supposed” to happen
- joint conservation
- exercise low impact
- weight loss to relieve load on joints
NSAIDS and COX-2, total joint replacement, autologous cartilage implantation (not many people qualify)
gout

what happens here? what do the crystal depositions look like? what is effected commonly as a strange presentation in most cases? what are the two ways these crystals accumulate and what are the percentages? what hardened structure can be found within joints of chronic gout? what labs do you do? what is diagnostic? what is the difference between the treatment for acute and chronic treatment?
most common form of inflammatory arthritis in m/w over 40
acute arthritis (usually at night) by sudden increase and deposition of uric acid crystals in the joint
great toe effected in 50% of cases, but can effect any joint in the body: ankles, knee, hands, wrists
cause: hyperuricemia, too much in circulation and in 90% of cases there isn’t enough secreted from the kidneys instead of overproduction (10%)
joints contain tophi, hardened nodules (chronic)
Labs: uric acid levels, may have elevated WBC, uric acid crystals in joints are diagnostic, xray to access joint damage
Acute TX: NSAIDS, colchicine
Chronic: Xanthine oxidase inhibitor, allopurinol (blocks production) or probenecid (increases uric acid excretion)

pseudogout
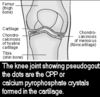
what is this caused by? what joint is the most commonly effected? what isn’t present that is seen in regular gout? where do you see the deposits? what do the crystals look like under the microscope?
acute inflammatory disease caused by calcium pyrophospate crystals
calcium pyrophosphate dihydrate disease
knees most commonly effected
*****no tophi present that differentiates from gout****
see calium deposits in the cartilage
aspiration see rod shapped crystals with blunt ends and befringement unlike gout
conservative and excision of chondrocalcinosis

Reactive Arthritis (Reiter Syndrome)

what is this join infection caused by? what are the two most common routes a person can contract this? what are the 4 symtoms that are included as a part of this tetrad? what do you want to make sure you do? and what test will be negative? what do you treat with?
joint inflammation that presents after PREVIOUS INFECTIONs commonly from sexually transmitted or gastroenteritis
chlamydia urethritis most common pathogen
Tetrad presentation:
- urethritis (difficulty urinating,
2. conjunctivitis (eye inflammation)
3. olioarthritis (1-4 joints)
4. mucosal ulcers (oral, balantitis*peeling of skin on penis*, stomatitis *inflammation of the mouth)
5. keratoderma blennhoragicum rash/ulcers on bottom of feet
CULTURES WILL BE NEGATIVE. STRONG HLB-27 relationship 80%
Treatment: PHYSICAL THERAPY NSAIDS, can give abx but not very helpful in sxs

herniated nucleus pulposus

what happens in a herniation? where does this most commonly occur in the vertebrae and in the spinal cord? what will the 3 main symptoms be and what are 3 things a patient will get pain with that are normal things? what do you do for treatment?
this is when the nucleus pulposus, the soft gelatinous center is herniated posteriorally since this is where the annulus fibrosis is the weakest!!!
usually occurs in lumbar spine since takes the most load
see motor and sensory manifestation
- tingling, numbness, or burning pain (seen in sagital and axial MRI images)
- pain with coughing, sneezing, and laughing
RICE, NSAIDs, surgery

spinal stenosis

what is this caused by? what two conditions for the risk of stenosis increase with? what unique thing makes this better, and what makes this worse? what can you see the in the lumbar region? what will you see on the MRI? what can you do for treatments for this?
compression of nerves of spinal cord caused by narrowing of the spinal cord and foramen
commonly seen in spondylosis and degenerative arthritis
pain increases with walking or axial loading (leaning back), and decreases with leaning forward, flexion!
back and leg pain, soft tissue and thecal narrowing, can see loss of lumbar lordosis
TX: acetaminophen, weight reduction, pelvic tilt, abdominal exercises….last choice decompressive surgery

osteoporosis

what is this? who is it most common in? what is the nickname for this disease? what imaging type do you want to preform? what 3 presentations might you find on physical exam?
abnormal bone remodeling, decrease in the total volume of bone making it less dense, since less strong it leads to increased fractures!
imbalance between bone formation and reabsorption
most common in menopausal women
“silent disease”
presentation: height loss, kyphosis, severe cervical lordosis dowagers hump
Dexxa scan of spine and hip

explain what happens in rheumatoid arthritis?
affects the lining of multiple joints synovitis, causing a painful swelling that can eventually result in bone erosion and joint deformity, autoimmune (not wear and tear like osteoarthritis)
hyperplastic synovial tissue called pannus erodes the cartilage, subchondral bone, tendons, and ligs “like a line of soldier marching to battle and destroying everything in their pathway. joint erosion

why is it important to always look at the feet of a rheumatoid arthritis pt? if suspicious they have it what is important to do?

see it on the feet before the hands so really important to get xrays of both the hands and feet!!
ALWAYS DO BOTH!!
if suspicious on physical exam, must feel joints because you will feel the difference between individual joints!

