HTC (COMBINED) Flashcards
I combine all topics here, but I also have them seperately. Study all here or sperately by topic names
Odontogenic Cysts can be two types
Inflammatory
or
Developmental
Inflammatory cysts
List ( 4 cysts)
- Periapical (radicular)
- Residual periapical
- Buccal bifurcation
- Paradental
Developmental Cysts
List ( 9 cysts)
‐ Dentigerous
‐ Eruption
‐ Gingival cyst of newborn
‐ Gingival cyst of adult
‐ Lateral periodontal
‐ Glandular odontogenic
‐ Odontogenic keratocyst
‐ Orthokeratinized odontogenic
‐ Calcifying Odontogenic
The following cysts are histologically the same in which way
-Periapical (radicular)
‐ Residual periapical
‐ Buccal bifurcation
‐ Paradental
‐ Dentigerous
‐ Eruption
‐ Gingival cyst of newborn
‐ Gingival cyst of adult
all lined by squamous epithelial
What are the
Sources of epithelium
within the jaw bone
▪ Epithelial rests of Malessez
▪ Reduced enamel epithelium
▪ Fissural cysts – when 2 pieces of bone come together
▪ Odontogenic cysts
▪ Epithelial component of odontogenic tumors
▪ Salivary gland inclusions – rare, incorporated in development
radicular cyst, inflammatory cyst are other names for ?
Periapical Cysts
The most common cyst of the jaws ?
Periapical Cysts
Periapical Cysts
Demographic and location
▪ Any age (peak in 3rd ‐ 6th decades, rare in 1st decade)
▪ No sex predilection
▪ MX > MD (anterior MX most common)
Tooth vitality and Periapical Cysts
- Involved tooth usually non‐vital/non‐responsive with thermal and electric pulp testing
- Should test vitality of tooth if see radiolucency in apex\
- If tooth vital, and still see radiolucency ► should do biopsy
Periapical Cyst
(Radiographic)
- Usually appears as well‐circumscribed periapical radiolucency with widening of the PDL space and/or loss of lamina dura
- Typically small (< 1 cm) but can grow to large dimensions if left untreated
- Radiographic findings can NOT be used for definitive diagnosis
Why the Radiographic findings of Periapical Cyst can NOT be used for definitive diagnosis?
‐ similar appearance with:
- periapical granuloma
- odontogenic tumors
- early COD {Cemento Osseous Dysplasia}
Lateral radicular cyst appears on the lateral surface of the root of a non‐vital/non‐responsive tooth
‐ A differential for which cyst?
lateral periodontal cyst

Periapical Cysts
►Would need to test both teeth for vitality.

Periapical Cyst

Periapical cyst
shows inflammation at site
abscess developed fistula tract thru
soft tissue. Pt will have pain until
pressure is released
Periapical Cyst
treatment
- endodontic therapy or extraction of involved teeth
- larger lesions may require biopsy along with endodontic therapy
- lesions which fail to resolve should be biopsied
- follow-up at 1-2 years
Residual Cyst
Etiology
- After tooth extracted, not properly cleaned ► the residual cells of the cyst lining and inflammatory cells continue to proliferate
- Has to be at site where tooth was previously removed
Residual Cyst
Radigraphically
- well defined round to oval radiolucency in the site of a previous extraction
Residual Cyst
Histologically is identical to which cyst?
- identical to the radicular cyst (periapical cyst)
- Should biopsy to rule out other causes
Residual Cyst
Treatment
-Removal
- Enucleation if small
- Marsupialization if large
- Note:*
- Enucleation* means: removal of an organ or other mass intact from its supporting tissues
Marsupialization means: surgical technique of cutting a slit into an abscess or cyst to empty its contents and suturing the edges of the slit to form a continuous surface from the exterior surface to the interior surface of the cyst or abscess.
Promotes Decompressing and shrinkage.

Residual Cysts

Residual Cyst
Paradental Cyst
Etiology
Some controversy over this designation
‐ some think they are inflammatory cyst
‐ some think they are developmental cysts
▪ Etiology: remains unclear
Paradental Cyst
Radiographically
- Radiolucent area noted
- most frequently, along the distal aspect of an impacted or partially erupted third molar
Which cyst has been associated w/ enamel extensions into furcation areas of the
involved teeth?
Paradental Cyst
Paradental Cyst
Treatment
Extraction of the tooth along with the lesion

Paradental Cyst

Paradental Cyst
Buccal Bifurcation Cyst
is similar to what Cyst ?
Similar to a paradental cyst
‐ EXCEPT: location is central on the buccal of mandibular first molars
Buccal Bifurcation Cyst
Etiology
unclear
Buccal Bifurcation Cyst is most commonly seen with eruption of what tooth?
The eruption of the permanent first molar
Buccal Bifurcation Cyst
Clinically
seen as
- swelling
- tenderness of soft tissue over involved area
Which
Radiograph type is best to see
Buccal Bifurcation Cyst?
▪ Radiolucency best seen with an occlusal radiograph

Buccal Bifurcation Cyst
as seen in occlusal radiographs

Buccal Bifurcation Cyst
as seen in occlusal radiographs
Buccal Bifurcation Cyst
Treatment
▪ Enucleation of cyst; tooth extraction unnecessary
▪ Some cases resolve w/o surgery
▪ Some resolve w/ daily irrigation of buccal pocket with saline/hydrogen peroxide
Dentigerous Cyst
also known as ?
Follicular Cyst
What is most common type of developmental odontogenic cysts?
20% of all epithelial lined cysts of the jaw
Dentigerous Cyst
Dentigerous Cyst
Origin & Etiology
Originates: by the separation of the follicle from the crown of an unerupted tooth
Pathogenesis: accumulation of fluid between the tooth and the reduced enamel epithelium
Dentigerous Cyst
Clinically
▪ Small cysts typically asymptomatic and picked up
on routine radiographic exam
▪ Large lesions may show expansion of bone
▪ Cysts may become infected, especially if partially erupted
tooth
Dentigerous Cyst
Demographics & Location
- Mostly mandibular 3rd molars (rarely unerupted deciduous teeth)
- Most commonly present in 2nd and 3rd decades
What is a key characteristic of Dentigerous Cyst location?
- Attached to the tooth at the CEJ
Small Dentigerous Cyst
are hard to differentiate radiographically from —?
enlarged/hyperplastic follicle
Rule of thumb:
- If 4‐5mm or more of radiolucency ► dentigerous cyst
- If <4mm of radiolucency► can be hyperplastic follicle
dentigerous cyst or
follicle ?

_dentigerous cys_t
b/c *attachment at CEJ

Dentigerous Cyst

dentigerous cyst

dentigerous cyst

dentigerous cyst

Grossly image of
Dentigerous Cyst
Dentigerous Cyst
Treatment

- Decompression: Try to open window in the jawand put tube into cyst lumen and have pt irrigate a few times a day for a few weeks ► release pressure and allows bone to grow back ► cyst will shrink
- If get rid of whole area surgically► c_an risk_ fracturing the jaw
What is the Soft tissue counterpart of a dentigerous cyst?
Eruption Cyst
Eruption Cyst also known as
eruption hematoma
Eruption Cyst
Etiology
- Results from accumulation of fluid in the follicular space when the tooth has erupted over the alveolar bone *NOT in bone*
Eruption Cyst
Demographic & Location
▪ Usually seen in 1st decade (children)
▪ Most often involves 1st permanent molar and maxillary incisors
Eruption Cyst
Clinically
Frequently normal mucosal color, BUT surface trauma (ex. chewing) may result in bleeding into the cystic space► may look purple or blue
▪ Usually soft or fluctuant(like a balloon) upon palpation
Eruption Cyst
Treatment
- Unless symptomatic, no treatment required, cysts resolve upon eruption of teeth

Eruption Cyst

Eruption Cyst
Cysts of the Newborn
can either be — or —
Palatal cysts
or
Gingival cyst
Palatal cysts
Types
&
Location
‐ Bohn’s nodules: scattered over HP (hard palate), often junction of HP and SP (soft palate)
‐ Epstein’s pearls: along median palatal raphe
Cysts of the Newborn:
Palatal cysts
Demographics
- Seen in 60‐80% of neonates
Cysts of the Newborn:
Palatal cysts
Clinically
- 1‐3 mm cream to white papules (keratin filled cysts)
*NOT in bone*
Cysts of the Newborn:
Palatal cysts
Treatment
No treatment is required
‐ Resolve (degenerate or rupture) on their own in a
few months
‐ Once baby eats solid foods, will go away

Cysts of the Newborn:
Palatal cysts
Cysts of the Newborn:
Gingival cyst of the Newborn
Also known as
Dental lamina cysts
Gingival cyst of the newborn
demographics & Location
- Found superficially on the alveolar ridge mucosa
- MX > MD
- Rarely seen after 3 mos. of age
Gingival cyst of the newborn
Treatment
▪ No treatment is necessary
▪ Spontaneously resolve (degenerate or rupture)
Gingival cyst of the newborn
Clinically
- 1‐3 mm creamy white papule (keratin filled cysts)
- *NOT in bone*

Gingival cyst of the newborn/ Dental lamina cysts/Cysts of the Newborn-gingival
What is the soft tissue counterpart of the lateral periodontal cyst ?
Gingival Cyst of the Adult
Gingival Cyst of the Adult
Origin
Derived from dental lamina rests
‐ Rests of Serres
Gingival Cyst of the
Adult
Demogrophic & Location
▪Uncommon lesion
▪ 60‐75% mandibular canine/premolar area
‐ most common location on the facial or buccal aspect
▪ 5th and 6th decade most common
Gingival Cyst of the
Adult
Clinically
- Painless, dome‐like swellings up to 5 mm in diamete
- Often with a bluish or grayish hue
Gingival Cyst of the
Adult
has similar histology to which cyst?
lateral periodontal cyst
Gingival Cyst of the
Adult
Treatment
- simple surgical excision
- Unlikely to recur/come back

Gingival Cyst of the
Adult

Gingival Cyst of the
Adult

Gingival Cyst of the
Adult
notice the bluish hue
Lateral Periodontal Cyst represents the intrabony counterpart of which cyst?
gingival cyst of the adult?
Lateral Periodontal
Cyst
Origins
- Developmental cyst believed to arise from dental lamina rests
Lateral Periodontal cyst is diagonsed when cysts occur in the lateral periodontal region and after what have been excluded?
- an inflammatory origin cysts or the diagnosis of odontogenickeratocyst have been excluded
Lateral Periodontal Cyst
Charcterstics and tooth vitality
▪ Commonly asymptomatic and found on routine radiographic exam
▪ Associated teeth tests vital/responsive with electric pulp test
Radilucency Lateral to a teeth
how would you know if it’s
Lateral Periodontal Cyst
or
Lateral Radicular Cyst
or
Lateral OKc
‐ If pulp alive► lateral periodontal cyst or Lateral Okc ( if huge lesion)
‐ If pulp dead► lateral radicular cyst
Lateral Periodontal Cyst
Demographic and Location
▪ Most likely found after age 30
▪ Males>Females
▪ ~65% mandibular canine/premolar area
‐ Can also be seen between canine and lateral incisor
Lateral Periodontal Cyst
Radiographically
Present as well circumscribed, unilocular radiolucencies between 2 teeth, located lateral to tooth root
▪ Most often 0.5‐1.0 cm in diameter
▪ Radiographic features are NOT diagnostic
Which is here is
Lateral Periodontal Cyst
Lateral Radicular Cyst
Lateral Odontogenic Kertocyst

- Could be differential for lateral Odontogenic keratocyst, except this does not grow in size
- Lateral radicular cysts from an accessory canal if tooth is non vital
- or it could be Lateral Periodontal Cyst if tooth is vital!


Lateral Periodontal
Cyst

Lateral Periodontal
Cyst
Lateral Periodontal
Cyst
Treatment
- consists of conservative enucleation
What cyst is a variant of lateral periodontal cyst?
Botryoid Odontogenic
Cyst
Botryoid Odontogenic
Cyst
Grossly and Microscopically
shows a grape‐like cluster of small
individual cysts
Botryoid Odontogenic
Cyst
Radiographically
▪ Either unilocular or multilocular on radiographs, depending on size of the lesion
▪ Cyst lining similar to lateral periodontal cyst

Botryoid Odontogenic
Cyst
well circumscribed, between 2 teeth (similar to
lateral odontogenic cyst), multilocular

Botryoid Odontogenic
Cyst
Glandular Odontogenic
Cyst
Charcterstics
- A rare odontogenic cyst which exhibits features of glandular differentiation within the epithelium
- Presumably represents the pluripotentiality of odontogenic epithelium
Glandular Odontogenic
Cyst
Demographics
▪ Wide age range from 2nd to 9th decades
‐ mean age 49
▪ ~ 80% of cases in mandible
▪ Anterior lesions
‐ More common
‐ May cross the midline
Glandular Odontogenic
Cyst
Radiographically
▪ Uni‐ or (more often) multilocular radiolucency
▪ Well‐defined with a sclerotic border
Glandular Odontogenic
Cyst
reccurance rate
(~ 25% recurrence rate)
Can be locally aggressive
Glandular Odontogenic
Cyst
Clinically
▪ Usually asymptomatic unless inflamed
Histologic differential diagnosis of Glandular Odontogenic
Cyst includes –?
mucoepidermoid carcinoma (salivary gland tumor)

“Primordial” Cyst
Assuming histologically it is different from OKC
“Primordial” Cyst
is not a true ——-
- lesion, was actually some other type of cyst
- it is now thought that most of the reported Primordial cysts were actually OKCs
Odontogenic
Keratocyst
OKC
Also known as
keratocystic odontogenic tumor (KOT) -2005 WHO
but now it’s back to OKC
Odontogenic
Keratocyst (OKC)
Etiology
- Growth and expansion of this lesion due not only to osmotic effects/pressure, but to unusual gene expressions
Which unusal gene expression causes growth and expansion of OKC ?
- Expresses Ki‐67 (high rate of cell proliferation)
- O_verexpression of Bcl‐2_ (antipoptotic protein)
- Overexpression of MMP’s 2 and 9 (thought to allow growth into connective tissue)
-
Mutation of PTCH, a tumor suppressor gene
- when PTCH is non‐functional → cell proliferation
Odontogenic
Keratocyst (OKC)
Demographic & Location
- ~ 60% present in 2nd and 3rd decade, but can occur at any age
-
Mandible affected in 60‐80% of cases
- tendency to occur in posterior mandible and ramus
- 25‐40% of cases involve an unerupted tooth
- ‐ 5% of patients have multiple cysts
Odontogenic
Keratocyst (OKC)
differes from
Meloblastoma
in its growth pattern
Odontogenic Keratocyst (OKC) :grows in anterior to posterior manner before causing cortical expansion
while
Meloblastoma: causes cortical expansion early
Which cyst make up ~10‐15% of all odontogenic cysts?
Odontogenic
Keratocyst (OKC)
5% of Odontogenic
Keratocyst (OKC) are associated with which syndrome?
nevoid basal cell carcinoma
syndrome(Gorlin syndrome)
What are the site distribution of OKC?
Most of OKC in
posterior region

Odontogenic
Keratocyst
Reccurance Rate
- HIGH Recurrence Rate
- Benign, but locally aggressive biologic behavior
- Solitary OKCs have ~10% recurrence rate with appropriate treatment
- _Multiple OKCs hav_e ~ 30% recurrence rate
Odontogenic
Keratocyst
(OKC)
Reccurance Rate Order
from highest to lowest reccurance rate
Syndrome OKC > Multiple OKC > Solitary OKC > Conventional odontogenic cysts
Odontogenic
Keratocyst
OKC
Radiographically
- Usually a well‐circumscribed radiolucency with smooth, often corticated margins
▪ Cysts may be
‐ Unilocular (most common)
‐ Multilocular (larger lesions)
Odontogenic
Keratocyst
OKC
clinically
▪ Small cysts are typically asymptomatic and picked up on routine radiographic exam
▪ Larger cysts may or may not be asymptomatic
▪ *Cysts tend to grow in an antero‐posterior direction prior to lateral growth ►therefore cysts are usually quite large when they start to expand the cortical plate
Odontogenic
Keratocyst
OKC
Has similar Radiographic findings with ?
- dentigerous cyst
- ameloblastoma
- and others
Odontogenic
Keratocyst
OKC
Treatment
▪ Marsupialization (decompression)
▪ Peripheral ostectomy
‐ Carnoy’s solution
▪ Resection
▪ Medications targeted to PTCH
▪ Long term follow‐up

Odontogenic
Keratocyst
OKC

Odontogenic
Keratocyst
OKC

Odontogenic
Keratocyst
OKC

Odontogenic
Keratocyst
OKC

similar to
lateral
periodontal cyst
but is actually
OKC
Nevoid Basal Cell Carcinoma
Syndrome
is also known as —– ?
Basal Cell Nevus or Bifid Rib Syndrome
or
Gorlin syndrome
Which cyst is assoicated with
Nevoid Basal Cell Carcinoma
Syndrome
?
Odontogenic Keratocyst
“OKC”
Nevoid Basal Cell Carcinoma
Syndrome
(Gorlin syndrome)
_modes of inheritanc_e
Autosomal dominant inheritance
Nevoid Basal Cell Carcinoma
Syndrome
Which Gene mutation and pathway
associated with
Nevoid Basal Cell Carcinoma
Syndrome
(Gorlin syndrome)
- Mutation of PTCH (tumor suppressor gene)
- in the Sonic Hedge Hog pathway
Nevoid Basal Cell Carcinoma
Syndrome
Prognosis
■ Prognosis depends on progression of skin tumors
Nevoid Basal Cell Carcinoma
Syndrome
Treatment
✎Surgery (typically MOHS)
✎Sometimes curette them
✎ Radiation therapy (RT) is typically not the first line of therapy with small lesions RT
✎Cryotherapy which means they just use a little liquid nitrogen and freeze them
✎Photodynamic therapy with photosensitizer and topical medications
■ New medication: Vismodegib inhibits sonic hedgehog pathway by binding smoothened (SMO)
- suppressive rather than curative cause it seems to work for short time and after ~7-8 months ..may also helps suppress growth of OKC

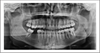
✎A patient who has Nevoid Basal Cell Carcinoma
Syndrome
✎We can see multiple cystics areas and lesions in
the jaws, maxillary and mandible
✎Both 3rd molar displaced in the maxilla because of
the cyst

✎Multiple lesions, impacted 3rd molar in mandible
and displaced 3rd molar up into the sinus,
✎These too many lesions hard to manage the issue
with a surgery
✎This large area on the left mandible – good example of why we do
decompression because if you just remove this lesion
and the entire area is left open, this would be an area
risk for fracture
What is this called
which can be seen with
Nevoid Basal Cell Carcinoma
Syndrome

✎An example of the pitting that can be seen palmar
and plantar
~ This is a side of a hand
✎This is an early stage of basal carcinoma which
never goes on (like it is aborted)
What are these findings that is associated with

Nevoid Basal Cell Carcinoma
Syndrome?
- thousands of basal cell carcinoma is developing on the skin
-very difficult to manage with surgery,
~ That’s why they remove
the larger ones, the deeper ones ~ They leave the one
that’s less as an issue until they get to a larger size to
be removed
Why Basal Cell Carcinoma is very problematic ?
It’s not the lesion themselves causing metastasis
that’s the issue, it’s the lesion growing deeply and in affecting adjacent structures that really is the
issue with basal carcinoma
What is the Most common type of skin cancer?
Basal Cell Carcinoma
(BCC)
Basal Cell Carcinoma
(BCC)
Demographics
- 2-3 million cases a year
- About 3 out of 4 skin cancers are basal cell carcinomas
Basal Cell Carcinoma
Growth and location
(BCC)
- Develop in the lowest layer of the epidermis, called the basal Layer
- Develops on sun-exposed areas: cumulative DNA Damage
- Slow-growing
• If not treated, basal cell cancer can grow into nearby areas
and invade the bone or other tissues beneath the skin
Basal Cell Carcinoma
Progrssion
(BCC)
within 5 years of being diagnosed with
BCC►35%-50% of people develop a new skin cancer
Calcifying Odontogenic Cyst
COC
also known as
?
- Calcifying Cystic Odontogenic Tumor
- Gorlin Cyst ( don’t confuse it with Gorlin syndrome)
- Ghost Cell Tumor
*
Calcifying Odontogenic Cyst
(COC)
can present in 3 types
-
■ Cystic Unilocular COC
- COC with odontoma (~ 20%)
- Extraosseous/peripheral – present in older patients
-
■ Solid COC (odontogenic ghost cell tumor)
- Often demonstrate a more aggressive behavior
- WHO once considered them all CCOT now back to COC
- ■ Odontogenic ghost cell carcinoma
- very rare lesion
Collision Tumors is a term used to describe lesions involving Calcifying Odontogenic Cyst (COC), what does that mean?
- where you see both features of ameloblastoma with COC or adenomatoid odontogenic tumor with COC
Calcifying Odontogenic Cyst
(COC)
may occur in association
with
which tumors or cysts?
- Odontomas (a benign tumour linked to tooth development)
- Ameloblastomas (rare, noncancerous (benign) tumor)
- Adenomatoid odontogenic tumor (rare tumor of epithelial origin that is benign, painless, noninvasive, and slow-growing)
Calcifying Odontogenic Cyst
(COC)
Demographics & Location
■ Peak in second decade, most before age of 40
■ Frequently presents anterior to molars
■ ~ 20% extraosseous (peripheral), found in older age group (~ 50 years of age)
■ Female > Male
■ ~ 70% occur in MX
■ One third are associated with unerupted teeth, usually a canine
Calcifying Odontogenic Cyst
Radiographically
(COC)
■ Usually a well-circumscribed unilocular radiolucency, infrequent multilocular cases
■ One third to one half show radiopaque structures within the radiolucency
■ When you see calcifications within a lesion, you don’t use the term uni or multi locular anymore, but they are called mixed radiolucent/radiopaque lesions
■ May cause resorption or displacement of roots
■ One third are associated with unerupted Canine

**Calcifying Odontogenic Cyst (COC)**
- in the mandible and you can see it well circumscribed radiolucency
- a little bit of blunt root resorption in this area
- No calcifications in this one yet ►so this is still unilocular radiolucency
What are the clinical and radiographic findings here?
What is this lesion?

- Clinical finding for this patient was Obliteration of the vestibule space, because the mandible is showing expansion
- radiographically:we see radiolucency going as far as the first molar
- This is a mixed radiolucent radiopaque lesion in developing calcifications.
- This is an example of Calcifying Odontogenic Cyst (COC)
The hallmark of Calcifying
Odontogenic Cyst COC Histology is
Ghost cells
They have that sort of polygonal shape or roundish shape with the pink that looks like the cytoplasm, but in
the location where the nucleus would have then, there’s an empty spot
Histologically speaking, Calcifying
Odontogenic Cyst COC, basically
looks similar to what epithelium?
ameloblastic epithelium
Calcifying Odontogenic Cyst COC
Treatment
■Enucleation with peripheral ostectomy ~ Very similar to odontogenic keratosis
■ Follow up is long term because s_ome of the solid tumors have a more aggressive behavior_
■ Peripheral lesions are treated with excision
When COC is associated with another tumor, ameloblastoma, how would you treat?
■ the treatment is based on the more aggressive tumor
~ So you would treat the ameloblastoma.
~You wouldn’t treat conservatively the COC though
Fissural Cysts
(6)
❑ Nasolabial cyst
❑ Globulomaxillary cyst (historic)
❑ Nasopalatine (incisive canal) cyst
❑ Incisive papilla cyst
❑ Median palatal cyst
❑ Median mandibular cyst (historic)
Nasolabial Cyst
also known as
aka Nasoalveolar cyst
where a number of the visual cysts would develop

(1) That’s the nasopalatine, which is sort of up in the labial nasal fold and it’s in the soft tissue.
(2) Sort of where the nasal alveolar cyst would occur.
(3) Where the globular maxillary cyst would occur between the canine and the lateral sometimes between the lateral and the first premolar
(4) The nasopalatine in the cyst of the nasopalatine papilla
(5) Is the median palatal
Nasolabial Cyst
Etiology
■ Thought to be caused by:
- either epithelial remnants of the nasolacrimal duct
- or cells left after fusion of the maxillary, medial and lateral nasal processes during development of the midface
Nasolabial Cyst
Location
Rare soft tissue cyst of the upper lip, lateral to the midline (right under the ala of the nose) *NOT in bone*
■ Clinically see a swelling which can cause elevation of the ala of the nose ■ Intraorally see a swelling in the maxillary vestibule lateral to the midline (usually sort of in the canine area or just a little bit distal to the canine area) ■ Pain is uncommon, unless cyst becomes infected
Nasolabial Cyst
Clinically & Intraoray
■Clinically we see a swelling which can cause elevation of the ala of the nose
■ Intraorally see a swelling in the maxillary vestibule lateral to the midline (usually sort of in the canine area or just a little bit distal to the canine area)
■ Pain is uncommon, unless cyst becomes infected
Nasolabial Cyst
Demographics
■ Peak in 4th and 5th decades
■ 3 to 4 times more common in females
■ ~ 10% of cases are bilateral
Nasolabial Cyst
Treatment
- Surgical Excision via intraoral approach,
- usually do not recur ~ very low risk of occurrence

Nasolabial Cyst
The lesion here just below the nose and you can tell that it’s sort of raising the edge of the nose slightly

Nasolabial Cyst
the lesion raising the edge of the nose slightly
_Nasolabial Cys_t has a a respiratory type epithelium and so it’s very similar to what you would see in ?
either in the sinus or in the nasopalatine ducts
Is this

Globulomaxillary Cyst
lateral granulomas
OKCs
COCs
- we can see the displacement of the root
- A teardrop or pear shaped radiolucency between the lateral and the canine
- Well circumscribed maybe leaving a little sclerotic edge up here
- ended up being in a odontogenic keratocyst (OKC)
Is this Globulomaxillary Cyst , lateral granuloma or OKC?

~ it is kind of a teardrop or pear shaped size
~Little less well differentiated in this particular instance but again unilocular radiolucency between the roots of two teeth
This one ended up being an OKC
“Globulomaxillary Cyst”
Origin controvesy
why the name in quotations?
- it’s in quotations, because really there is no such thing as a globulomaxillary cyst
- because it was thought that this was remnants after fusion of the globular portion of the nasal process with the maxillary process, and now we know that these two processes are always united from the start and that there is no fusion
- When biopsied these cysts are odontogenic in origin
what does it mean for Globulomaxillary Cyst to be odontogenic in origin?
✎This is term used to describe a cyst in a particular anatomic location it is not a diagnosis
✎An odontogenic cyst (inflammatory cyst, lateral periodontal or even sometimes OKC) that forms in the area between the maxillary lateral incisor and the canine roots
~ It’s really associated with a_n anatomic location not with any particular cyst._
✎So it can be any of the odontogenic lesions such as lateral granulomas or cysts, OKCs, COCs, etc.
Globulomaxillary Cyst
Radiographically
✎Presents as a “inverted pear” shaped well-circumscribed radiolucency
✎Frequently causes displacement of the roots
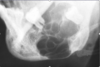
What are two different ways nasopalatine duct cyst arise?

- *A**. It can either be the cyst totally within bone
- *B**. It can actually cause widening of the orifice and causing the soft tissue expansion in this way
Most common non-odontogenic cyst of the oral cavity
Nasopalatine Duct Cyst
Nasopalatine Duct Cyst
also known as
incisive canal cyst
nasopalatine canal cyst

Nasopalatine Duct Cyst
✎This person is edentulous
✎ an inverted pear shape
✎The nasal spine is superimposed
on your radiolucency ► a heart shape

Nasopalatine Duct Cyst
✎Between the roots of the two teeth, a well circumscribed
radiolucency, not showing any changes to the adjacent structures
✎could be an enlargement of the incisive canal due to variation in size ~ early lesions can be hard to diagnose
✎the treatment in such cases: a follow up with another radiograph in six months to see if there’s been any change in size
✎ No surgical intervention until you see the cyst expanding

This is showing you the how the
papilla can be enlarged if it’s only
in soft tissue or if there’s a partial
soft tissue partial bone expansion
Nasopalatine Duct Cyst
Nasopalatine Duct Cyst
Origin
- arise from epithelial remnants of the nasopalatine duct which, embryologically, connects the oral and the nasal cavities

Median Palatine Cyst
Nasopalatine Duct Cyst
Demographic and Location
- Peak presentation in the 4th to 6th decades, but can occur at any age ~ because it takes a little bit of time for the cyst to grow within the bone
- commonly found on the anterior palate ~ typically in the nasal area of the papilla.
Is this Median Mandibular Cyst
Or something else

Remember
Median Mandibular Cyst is a term used to describe a cyst in a anterior mandible not a definitive diagnosis
So, this turned out to be an early ameloblastoma. It wasn’t a cyst
The lesion radiolucency in the anterior mandible and again
Nasopalatine Duct Cyst
Clinically
■ present with swelling o_f the anterior palate_ (in the nasal area of the papilla)
■ Most are asymptomatic, but they may have pain or drainage
Nasopalatine Duct Cyst
Radiographically
■ a well-circumscribed unilocular radiolucency on the midline of the anterior hard palate
between and apical to the central incisors
■ The radiolucency often have an oval or inverted pear shape with a sclerotic border
■ Superimposition with the nasal septum can create an appearance of the classic “heart” shape
Cysts of the incisive papilla
Incisive papilla cyst
Is a soft tissue cyst (no bone involvement) located in
the same area as the Nasopalatine Duct Cyst
on the midline of the anterior hard palate
between and apical to the central incisors
. They may be symptomatic or asymptomatic and usually are not seen radiographically.
some consider them to be uncommon variants of the nasopalatine duct cysts

Surgical Ciliated
Cyst of the Maxilla
In this premolar shot (middle image) you can see a well-circumscribed lesion
✎Because the maxillary sinus is radiolucent, it almost looks like this is radiopaque but it’s not
✎ If you did a CBCT you would see that it’s an empty space within the bone of the maxilla. It’s not actually radiopaque
Nasopalatine Duct Cyst
Treatment
- surgical excision
- recurrence is rare
Median Palatine Cyst
is
a variant of which cyst?
nasopalatine duct cyst
- it represents a more posteriorly placed nasopalatine duct cyst
- ~ It’s probably due to some sort of anatomic variation in the patients; that their palatine duct is just placed more posteriorly
- So instead of being between the roots of these two teeth, it’s placed more posteriorly
Median Mandibular Cyst
- A controversial cysts whose existence is questioned ~ similar to the globulomaxillary cyst
■ Originally thought to arise from the fusion of the “halves” of the mandible, but current embryology finds that
the mandible forms from a single bilobed process, therefore, no epithelial remnants would be found
■ Now, it is thought that cysts in this area represent odontogenic cysts or tumors
-
Median Mandibular Cyst is a term used to describe a cyst in a particular anatomic location not a definitive diagnosis
- ~ It is other lesions that occur in that particular location
- The Anterior Mandible
Surgical Ciliated
Cyst of the Maxilla
Etiology
■ Occurs after trauma or sinus surgery (iatrogenic - reactive not neoplastic)
Surgical Ciliated
Cyst of the Maxilla
Formation
■a portion of the sinus lining is separated from the sinus and forms an epithelial lined cavity in bone
■ Cavity fills with mucin produced by the mucous cells of the cyst lining
■ These cysts enlarge as the intraluminal pressure increases, causing destruction of bone
Surgical Ciliated
Cyst of the Maxilla
occurs frequently
after
which procedures?
- after a Caldwell-Luc procedure
- sometimes with difficult maxillary extractions
In which country Surgical Ciliated
Cyst of the Maxilla
are reported with higher frequency ?
Japan

Surgical Ciliated
Cyst of the Maxilla
In this premolar shot (middle image) you can see a well-circumscribed lesion
✎Because the maxillary sinus is radiolucent, it almost looks like this is radiopaque but it’s not
✎ If you did a CBCT you would see that it’s an empty space within the bone of the maxilla. It’s not actually radiopaque
What are pesudocysts?
- They have no epithelial lining.
- They’re called cysts by convention just because that’s what everybody is used to
- They’re not true cysts.
pesudocysts
List
(5)
- Aneurysmal Bone Cyst
- Antral Pseudocyst
- Simple Bone Cyst
- Osteoporotic Bone Marrow Defect
- Stafne Bone Cyst
Aneurysmal Bone Cyst
Demographics
■ Most common site in the body is long bones or vertebrae
_■ In the jaw_s, most frequently seen in the 1st and 2nd decade
■ MD > MX
it’s a pesudocyst
Aneurysmal Bone Cyst
Clinically
- swelling, frequently a rather rapid swelling
- often with pain and/or paresthesia (signs which can be suggestive of the presence of a malignant or aggressive lesion)
Aneurysmal Bone Cyst
Etiology
- Etiology is unclear, may result from trauma or a vascular malformation
- most agree that it is a reactive and *not* a neoplastic lesion
Aneurysmal Bone Cyst
Radiographically
■ a radiolucency which can be either unilocular or multilocular in appearance
■ Borders are variable, often irregular in shape and may be ill-defined (again, giving the suggestion of malignancy)
■ Teeth may be displaced
■ we may see cortical expansion and thinning ~ the cortex itself can become quite thin
What does this person have?

- you might think that he has an odontogenic infection but he didn’t. You can see that there’s
a pretty significant swelling on the left side of his face
This is a Aneurysmal Bone Cysts

Aneurysmal Bone Cyst
you can see that there is kind of a
multilocular radiolucency in this particular area

Aneurysmal Bone Cyst
✎ There’s a radiolucency involving the second molar
that’s going as far anterior as the first molar and back
to the third molar
✎ There is a little bit of spiking root resorption and
that’s one of the signs that we associate with
malignancy
✎ It’s a little bit ill-defined ~ hard to say exactly
where it begins and ends

Aneurysmal Bone Cyst
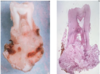
✎ It looks like a blood soaked sponge
✎ There’s these open sinusoidal spaces and then fibrous connective tissue surrounding them.
✎The sinusoidal spaces can vary in size; some of them are fairly small and others are large
Wall of the aneurysmal bone cyst can have a histology similar to the following
✎ Central giant cell granuloma
✎ Cherubism
✎ Brown tumor of hyperparathyroidism
Aneurysmal Bone Cyst
Treatment
■ Treatment is surgical enucleation and curettage
■ lesions can recur ~ Usually the recurrence is because
you didn’t get the entire thing out the first time around
■ Some surgeons follow enucleation with cryotherapy
■ Irradiation is contraindicated
Is bleeding a concern during surgical removal of Aneurysmal Bone Cyst?
■ No, vascularity is predominantly “low flow”, therefore not as much concern for bleeding upon surgical removal
■ As compared with central hemangioma where there is a concen for bleeding

Antral Pseudocyst
- a Dome-shape swelling on the floor of the sinus.
- They can sometimes be fairly subtle
Antral Pseduocyst are NOT Mucoceles
Mucoceles would have more of meniscus-like
appearancewhere it would come up tothe edge of
the sinus
Antral Pseudocyst
They are different than surgical ciliated cyst
in their lining, etiology, location and appearance!

Aneurysmal Bone Cyst
✎ A dome shape swelling on the floor of the sinus that’s associated with some _sort of inflammation of tooth of t_he premolar caused inflammation underneath the apex of the bone (right) and then that leads to accumulation of fluid which causes the sinus lining to elevate off the bone and fill with fluid
✎ After root canal therapy and once the infection gets under control, these will typically resolve on their own
As opposed of surgical ciliated cysts, Antral psuedocysts are not —-
( in term of their lining)
Not epithelial lined spaces
As opposed of surgical ciliated cysts, Antral psuedocysts are not —-
( in term of location)
Not within the bone but are in the sinus
As opposed of surgical ciliated cysts, Antral psuedocysts Develop as —-
( in term of etiology)
develop as an accumulation of an inflammatory exudate (often serum) between the sinus epithelial lining and the bone
-It develops because of an inflammatory event in the jaw, usually the maxilla, often from the roots of the maxillary teeth that cause inflammation
As opposed of surgical ciliated cysts, Antral psuedocysts appear as —-
( in term of Radiology)
Appears as a dome shaped elevation of the floor of the sinus
Simple Bone Cyst
also known as
aka traumatic bone cyst

Simple Bone Cyst
✎A well-circumscribed with cortication in the body of the
mandible, affecting the posterior aspect (premolars and the molars )
✎Note the scalloping that happens up between the roots. It
doesn’t cause root resorption and actually the lesion will grow up between the roots of the teeth

Simple Bone Cyst
- A well-circumscribedshowing the scalloping up between the roots of the teeth radiolucency

Simple Bone Cyst
✎Big lesion example: It’s going back to the molar area here.
✎You can see that the lesion extends over to the canine on the other side
✎Most lesions are usually in the anterior mandible
Simple Bone Cyst
Charcterstics
- A benign, empty or fluid filled, cavity in bone which is devoid of an epithelial lining – a pseudocyst
- Thought to be reactive, NOT neoplastic
Simple Bone Cyst
Etiology
Etiology ununcertain, theories include:
- trauma
- ischemic necrosis of medullary space
- cystic degeneration of a primary bone lesion
Simple Bone Cyst
Demographics
- In jaws, most likely in the 2nd decade
- Almost exclusively the mandible
- Twice as common in males
Simple Bone Cyst
Radiographically
- a well-circumscribed radiolucency with an irregular outline
- Tendency to “scallop” around and between roots (highly suggestive, but not diagnostic of this lesion)
Simple Bone Cyst
Treatment
- exploration and curettage of space to create bleeding. Clot will organize and allow bone repair
- Recurrence is rare

- You can see there’s a little bit of radiolucency.
- There happened to actually still be teeth in the area, but
- when it was biopsied it showed that it was a
- hematopoietic or osteopoietic bone marrow defect
Stafne Bone Cyst
Charcterstics

■ An asymptomatic focal concavity of the cortical bone on the lingual aspect of the MD
■ A pseudocyst, not a true cyst
Osteoporotic Bone Marrow Defect
Demographic
■ Uncommon finding
■ > 75% of cases are in females
■ ~ 70% occur in the posterior MD, often in an edentulous area
it’s a pesydocyst
Osteoporotic Bone Marrow Defect
Etiology
- Etiology unclear
- may be hyperplasia of marrow due to need for RBCs or
- abnormal regeneration of bone after an extraction or persistence of fetal marrow

Stafne Bone Cyst
This is the classic look.
- a well-circumscribed corticated radiolucency
- below the inferior alveolar nerve, away from the teeth.
- They can be either oval, like this, or round in appearance

Stafne Bone Cyst
Less common location
Check if the teeth were vital with vitality test
Get a CBCT in that area
to see what was going on first and then once you saw
the CBCT you’d be able to make the diagnosis.
Osteoporotic Bone Marrow Defect
Charcteristics
- it’s a pesydocyst
- a radiolucency in an area typically
where tooth has been removed. Instead of filling in with bone, it fills in with marrow. - When we biopsy it, you’re seeing the hematopoietic elements. (fat, early stages of (the -blasts of) red cells,
white cells. - We see basic bone forming marrow content

Stafne Bone Cyst
What we see on biopsy:
✎It’s just salivary gland tissue b_ecause the salivary glands grow into that space_
✎ It’s an empty space that they can grow into and that’s what they do; they just expand into that location. It’s not that the salivary gland is causing it
Osteoporotic Bone Marrow Defect
Hematopoietic bone marrow defect
Osteoporotic Bone Marrow Defect
Clincalally
■ Typically asymptomatic and found on routine radiographic exam
Osteoporotic Bone Marrow Defect
Radiographically
- Irregularly shaped radiolucency with either a well-defined or ill-defined border (It can be in the differential diagnosis with malignancy)
Osteoporotic Bone Marrow Defect
Treatment
■ Must biopsy to make a definitive diagnosis
■ No further treatment is then necessary
~ You don’t have to remove it; you can just leave it as it is
Stafne Bone Cyst
also known as
static bone cyst, Stafne defect
Stafne Bone Cyst
Demographics and Location
- Most commonly found near the angle of the mandible below the inferior alveolar nerve (but also seen in the anterior MD)
- > 80% in Males
- usually noted only in adults
Stafne Bone Cyst
Radiographically
Oval round well-circumcribed radilucency
Below the Inferior Alveolar Nerve
Stafne Bone Cyst
Etiology
- Believed to be developmental in origin, but usually noted only in _adults_
Stafne Bone Cyst
Treatment
- lesions in the posterior MD are usually pathognomonic
- no further treatment is necessary
Dermoid Cyst
Charcterstics
- Benign developmental cystic lesion
- Considered a form of teratoma
Remember: Teratomas have
all four embryologic layers and so you can see these cysts that have teeth, bone, hair, muscle, and nerves.
Dermoid cyst is sort of a lesser version of a teratoma in that it just has dermis, rather than all the other layers
Dermoid Cyst
Clinically
- Depending on whether the cyst is above or below the mylohyoid muscle►the lesion will cause swelling into the oral cavity elevating the tongue or under the chin in the submandibular area, respectively
- Usually found on the midline
- Painless and slow growing, if not infected
- Upon palpation, cyst feels doughy or rubbery
- Usually roundish to oval-ish swelling
Dermoid Cyst
demographic and locations
- Most common in the 1st and 2nd decade ( young pts)
- Can be found anywhere, but in the oral cavity they are ususally located in the anterior floor of the mouth (FOM) - usually on the midline
Dermoid Cyst
Treatment
- surgical excision
- recurrence is rare

Dermoid Cyst
a dome shaped
swellingin the floor of the
mouth.
If these were left long
enough, they could cause issues
with swallowing

Dermoid Cyst
✎This is a larger lesion on the floor of the mouth, causing
elevation of the tongue
✎If you let this go/grow, it would be similar to Ludwig’s angina where you would basically eventually obstruct the airway
✎The difference is this is very slow growing while Ludwig’s happens rather quickly. with fever and other symptoms.

Dermoid Cyst
- This is showing you when they occur below the mylohyoid muscle.
- You get an elevation under the chin.
- This is a fairly small one but they can get much larger
Epidermoid Cyst
also known as
infundibular cyst
epidermal inclusion cyst
“sebaceous” cyst (laymen’s term, not really sebaceous) ~
Epidermoid Cyst
Charcterstics
- A very common skin cyst
The epidermoid cyst is similar to which cyst?
similar to the dermoid cyst, except we don’t see those adnexal structures
Epidermoid Cyst
Etiology
- Often occur after _inflammation of a hair follicl_e
Epidermoid Cyst
Demographics and Location
■ Males > Females
■ Young adults more likely to have cysts of the face
■ Older adults have cysts of the back
Epidermoid Cyst
Associated with which
syndrome?
Associated with Gardner’s syndrome
Gardner syndrome is associated with polyps
in the intestine.
Gardner syndrome is associated with epidermoid cysts.

Epidermoid Cyst
A dome-shaped swelling.
There’s no change in the
overlying skin color, no redness, no pain
Epidermoid Cyst
Clinically
■ Subcutaneous nodular, firm to fluctuant, papule
~ It tends to be a subcutaneous, dome-shaped nodule that
can be either firm to fluctuant, depending on how much stuff is within the lumen
What is the key difference between a dermoid and epidermoid cyst?
- The key difference between a dermoid and
- epidermoid cyst, is that there’s no adnexal structures in an epidermoid cyst. There are adnexal structures in a dermoid cyst.
- The adnexal structures are: sebaceous glands, sweat glands, hair follicles, etc.
Epidermoid Cyst
Treatment
■ Treatment is excision
■ Recurrence is rare

Thyroglossal Duct Cyst
This is NOT a goiter.
It looks like an enlargement of the thyroid, but this ended up being just
a cyst, so they had a thyroglossal duct cyst
Thyroglossal Duct Cyst
Etiology/Origin
- A developmental cyst that develops from epithelial remnants of a tract which forms when the thyroid anlage descends into the neck from an area that later forms the foramen caecum
- Follows a path that goes anterior to the hyoid bone and ends below the thyroid cartilage
Thyroglossal Duct Cyst
Clinically
■ Cysts are typically painless fluctuant swellings, unless infected
■ If the cyst remains attached to the hyoid bone or the tongue ► i_t will move up and down when swallowing or protruding the tongue_
■ ~ 1/3 will present with a fistulous tract ~ so they’ll be draining.
Thyroglossal Duct Cyst
Treatment
■ surgical excision
■ recurrence are not uncommon
■ Rare cases of thyroid carcinoma developing in these cysts have been reported
Thyroglossal Duct Cyst
Demographics and locations
■ 60-80% of cysts are below the hyoid bone
■ Most commonly present in the first 2 decades (~ 50% prior to 20 years of age)
■ Cyst classically forms at the midline
■ The most common developmental cyst of the neck
What is the most common
developmental cyst of the neck?
Thyroglossal Duct Cyst

Branchial Cleft Cyst
a small one in a child.
You can see that
there’s a small cystic lesion here on the neck

Branchial Cleft Cyst
Then you can see it in an older person; this is getting
to be maybe 4-5 centimeters at least in size. He left
his for a little bit longer
Branchial Cleft Cyst
Also known as
cervical lymphoepithelial cysts
Branchial Cleft Cyst
Demographic and location
■ Most commonly presents in the 3rd to 5th decades
■Located on the lateral aspect of the neck, usually anterior to the sternocleidomastoid muscle
■2/3 of the reported lesions have been on the left side
■Although cyst are uncommon in the parotid gland, can see multiple lymphoepithelial cysts bilaterally in HIV positive patients
■These cases present as painless uni- or bilateral swellings of the parotid glands
Branchial Cleft Cyst
Clinically
- presents as a soft fluctuant swelling ranging from 1 to 10 cm in diameter

Oral Lymphoepithelial Cyst
A pale dome-shape swelling in the floor of the mouth. because the lesion is so close to the surface; you’re seeing little capillaries of the mucosa lining the lesion
Branchial Cleft Cyst
Etiology
Etiology is disputed
- Some think it is from remnants of the branchial cleft
- Others think it is cystic change of parotid gland epithelium which became entrapped in a cervical lymph node during development
Branchial Cleft Cyst
&
HPV patients
We can see multiple Branchial Ceft cysts bilaterally on the parotid gland
Painless swelling bilaterally or unilaterally on the parotid gland
Branchial Cleft Cyst
Treatment
surgical excision, recurrence is rare
Oral Lymphoepithelial Cyst
Demographics and Location
■ Uncommon lesion
■ The Most frequent location is the floor of the mouth (FOM) (> 50%)
Oral Lymphoepithelial Cyst
Clinically
■ Usually less than 1 cm in diameter
■ May feel firm or soft on palpation
■ Typically creamy to yellow in color
■ Painless unless infected
Oral Lymphoepithelial Cyst
Treatment
- Surgical Excision
- Reccurance is Rare

Oral Lymphoepithelial Cyst
A pale dome-shape swelling in the floor of the mouth. because the lesion is so close to the surface; you’re seeing little capillaries of the mucosa lining the lesion
What is the relationship between lesion’s agrressivness, rate of reccurance and follow up duration ?
the more aggressive the biologic behavior, the higher risk of
recurrence, and the longer the follow up needed for the patient
What is the spectrum of benign and malignant lesions

Which lesions are considered benigns
Things that have a very low rate of recurrence when you do a conservative excision or a nucleation ►they’re going to be very benign and they’re not going to be likely to be recurrent:
▪ Odontoma and radicular cysts are way down here near the benign side
▪ AOT (Adenomatoid Odontogenic Tumor) is benign.
▪ COCs (Calcifying odontogenic cyst) are benign.
▪ OKCs (Odontogenic keratocyst) ‐ they’re benign.
▪ Even Ameloblastomas are benign
which lesions are on the malignant side?
But eventually you get over to the side over here where you can have something like an Ameloblastic carcinoma ‐ truly malignant –> We know that it can metastasize and it can lead to death
▪ Lesions like Ameloblastomas and CEOTs will need to be managed more aggressively. (Not just curettage, aka surgical scraping or cleaning)
o You have a resection ‐ either a portion of the mandible is
removed or a segment of the mandible is removed.
What are the 3 Classification of
benign tumors?
- Epithelial
- Mesenchymal
- Mixed
What are the list of Epithelial Benign Tumors?
(5)
▪ Ameloblastoma
▪ Adenomatoid odontogenic tumor
▪ Calcifying epithelial odontogenic tumor
▪ Squamous odontogenic tumor
▪ Odontogenic keratocyst (aka Keratocystic odontogenic tumor)
What are the list of Mesenchymal Benign Tumors?
(5)
▪ Odontogenic myxoma
▪ Central Odontogenic fibroma
▪ Cementifying fibroma
▪ Cementoblastoma
▪ Granular cell odontogenic tumor
What are the list of Mixed Benign tumors?
5
▪ Odontoma (complex and compound)
▪ Ameloblastic fibroma/odontoma
▪ Primordial odontogenic tumor
▪ Dentinogenic ghost cell tumor
▪ Calcifying cystic odontogenic tumor(aka COC, ghost cell tumor)
Ameloblastoma
Charcterstics
- An epithelial odontogenic neoplasm (Tumor of Epithelial Origin)
- with a close histologic resemblance to the enamel organ
Ameloblastoma
Origin
Potential sources of epithelium include:
o Enamel organ – look like they’re about to deposit a
substance but never do
o Odontogenic rests (Malassez, Serres)
o Reduced enamel epithelium
o Epithelial lining of odontogenic cysts ‐ can actually have an ameloblastoma arise within a dentigerous cyst
Ameloblastoma
Radiographically
-Osteolytic tumor (radiolucent – no hard tissue formed)
- Well-circumscribed uni- or multilocular radiolucency
- Often with sclerotic or corticated borders
- May see blunt root resorption and displacement of teeth
- Frequently seen in association with unerupted teeth
Ameloblastoma
Clinically
- Rather slow growing tumor
- Larger lesions present as painless expansion or swelling of bone
- Smaller ones are asymptomatic, can be seen on routine imaging
- Buccal and lingual cortical expansion is common
- May perforate cortical plate and invade surrounding soft tissue
- Can arise in a dentigerous cyst (see transition from stratified
- squamous to ameloblastic epithelium)
Ameloblastoma
Types
Conventional/multicystic/solid/ (~ 80%)
- Unicystic (~6-15%) need entire specimen (excision) to know
- Desmoplastic
- Peripheral
- Malignant
Ameloblastoma
Demographics
▪ 11‐18% of non‐cystic lesions of the maxillofacial bones
▪ 4th and 5th decade most common, but occurs over a broad age range (rare in first decade)
o Usually starts 2nd decade, can go up to 80‐90s. Late 30s/early 40s are usually the peak
▪ > 80% occur in the mandible (most in molar/ramus area)
What is
the second most common
odontogenic neoplasm?
Ameloblastoma
(after odontoma)
o although odontomas are more like hamartomas
Which tumor can arise in a dentigerous cyst?
Ameloblastoma
(we see transition from stratified squamous to ameloblastic epithelium)
ameloblastoma
location
▪ Almost 80% or a little over 80% (of ameloblasts) are down in the mandible.
▪ And the vast majority are in the posterior mandible
▪ Do occur in maxilla but at lower rate


Unilocular and unicystic ‐ An example of a unilocular ameloblastoma that is
not associated with an impacted tooth
▪ Is between roots of two teeth, may be confused with lateral
periodontal cyst. Well‐circumscribed radiolucency
▪ Typical appearance for ameloblastoma
Multilocular, very well‐circumscribed, associated with impacted tooth.
Can see bowing of inferior aspect of mandible
lateral oblique radiograph.was used here

Ameloblastoma
clinically: Have expansion of the buccal plate, obliterating the vestibule in this area.
Radiographically: Root resorption of molar, unilocular radiolucency in mandible

Ameloblastoma
- Small lesion distal to impacted tooth.
- Unilocular radiolucency with elevation of alveolar ridge + some expansion of soft tissue

Ameloblastoma
▪ Well‐circumscribed radiolucency with a sclerotic or
corticated margin.
▪ If you had a CBCT, it would probably show you that there
was a thin septa in this area of residual bone trabeculae.
▪ Fracture could be caused by very large cysts.
▪ Resolve by decompressing unless with odontogenic tumor – need to remove the mandible 1cm+ on either side of lesion
Ameloblastoma
Etiology
▪ Over expression of Bcl‐2 (anti‐apoptotic protein)
▪ Expression of fibroblast growth factor (FGF)
▪ Over expression of matrix metalloproteinases (MMPs 9 and 20) – like in OKC, allowing tumor to grow into surrounding area
▪ Surprisingly, no significant increase in Ki‐67 expression (cell
proliferation marker) – ameloblastomas do NOT turn over rapidly
Case
16yo female
Describe the lesion and what is the diagnosis?

▪Left mandible, multilocular radiolucency associated with impacted tooth
▪ It’s well circumscribed, edge may be a little bit sclerotic or corticated
▪ It has displaced an impacted tooth down towards the inferior
aspect of the mandible
▪ Appears to be expanding the cortex of the mandible in areas
▪ There’s blunt resorption of the teeth adjacent (PMs and molar)
Ameloblastoma
Case

▪ Well‐circumscribed radiolucency, no impacted tooth
▪ But notice that it’s coming up to posterior aspect of first molar
▪ Surgery done to remove lesion, left inferior aspect of mandible
Follow‐up image: conservative surgery but still removed bone up to mesial aspect. Less conservative would be removing entire mandible
▪ Concern with that is paresthesia (from removing the nerve as well)
Conventional/Solid Ameloblastoma
Unicystic
ameloblastoma
types
Subgroup of
ameloblastomas
▪ Unicystic (Simple or luminal)
- lumina- confined to the surface lining of the cystic space
▪ Plexiform (intraluminal)
- intralumina-one or more areas of the ameloblastic epithelial lining, proliferate into the lumen of the cystic space
▪ Mural – hard to distinguish from conventional,
so pathologists think they should NOT be treated the same as unicystic (which would be a more conservative treatment)
▪ Ameloblastoma arising in a cyst ‐ can usually be treated in a similar way as unicystic ameloblastoma.


Unicystic Ameloblastoma
but could be
Dentigerous Cyst
based on clinical presentation!
So radiograph is not diagonstic

Desmoplastic
Ameloblastoma
- Spherical growth. Within it, has both radiodense and radiolucent areas (is
- mixed radiolucent‐radiopaque)– similar appearance to benign fibro‐osseous lesions.
- Well‐circumscribed, corticated.
Conventional/Solid Ameloblastoma
Treatment
- Resection (treatment depends on extent of the lesion and anatomy of involved bone)
- Segmental
- Composite
- Long term (decades) follow up is needed for these patients

Peripheral
Ameloblastoma
Unicystic Ameloblastoma
Demographcics and Locations
▪ Younger initial presentation (~ 50% in 2nd decade)
▪ 90% in MD (mandibular)
▪ Typically asymptomatic and found on routine radiographic exam
Unicystic Ameloblastoma
Radiographically
- Commonly a well‐circumscribed radiolucency that surrounds the crown of an unerupted tooth
- Commonly accompanied by root resoprtion
Unicystic Ameloblastoma
radiographically can be confused with which cyst?
- Radiographically can be confused with dentigerous cyst
- Presence of root resorption should increase your suspicion of ameloblastoma
Unicystic Ameloblastoma
Treatment
- Treatment is typically enucleation and curettage
- Reports of lower rate of recurrence (10‐20%) than conventional ameloblastoma (50‐90%) with similar treatment
- Some recommend decompression prior to surgery
- Use of Carnoy’s solution after enucleation- resulted in a recurrence rate lower
Desmoplastic
Ameloblastoma
Location
- Anterior jaws (particularly maxilla)
Desmoplastic
Ameloblastoma
Radiographically
- looks “fibro‐osseous” due to mixed radiolucentradiopaque appearance
- Mineralization of dense collagen
- Well‐circumscribed, corticated.
case

Calcifying Epithelial Odontogenic Tumor
(CEOT)
Clinically: we see a little expansion on inferior aspect of mandible + lingual too
Radiographically: we see well‐circumscribed, a little corticated/sclerotic edge, impacted tooth
▪ we can see bowing of inferior aspect of mandible
▪ Within areas of radiolucency, see areas of opacity (calcified lesions = classic CEOT)
▪ When smaller► could have looked *unilocular*

Calcifying Epithelial Odontogenic Tumor(CEOT)
- flecks of calcifications.
- Calcifications all around crown is common

Calcifying Epithelial Odontogenic Tumor(CEOT)
- Multilocular radiolucency with calcifications.
- an expansion up to PMs and back to 2nd molar
- as well as bowing of mandible.

Calcifying Epithelial Odontogenic Tumor(CEOT)
- Fewer calcifications here, well‐circumscribed and corticated, impacted tooth.
- periosteal reaction causing elevation at the bottom of image!

Calcifying Epithelial Odontogenic Tumor(CEOT)
- well‐circumscribed radiolucency with calcifications in lower anteriors
Peripheral
Ameloblastoma
Origin and Charcterstics
- Thought to arise from epithelial rests or basal cells in the gingiva
- Uncommon
- Does not invade underlying bone
- Histology is the same as conventional type
Peripheral
Ameloblastoma
location
- Found on gingiva or alveolar mucosa (*that’s why it’s named peripheral or extraosseous)
What are the two types of “Malignant”
Ameloblastomas ?
- Malignant ameloblastoma
- Ameloblastic carcinoma
▪ Malignant ameloblastoma
o Primary lesion and metastasis have normal welldifferentiated
ameloblastic (benign) histology
o Most commonly to lung
▪ Ameloblastic carcinoma
o Primary lesion has atypical poorly‐differentiated
neoplastic(malignant) histology, may metastasize
Adenomatoid odontogenic tumor
(AOT)
Origin
- thought to arise from remnants of the dental lamina in the gubernacular cord /canal

What is Ameloblastic carcinoma?
- a primary lesion has atypical poorly‐differentiated
- neoplastic(malignant) histology
- may metastasize
What is the DD?

well‐circumscribed radiolucency at crown of an impacted canine
Hard to tell if attaches at CEJ.
If further down, less likely a dentigerous cyst and more likely AOT, ameloblastoma, or OKC

we see calcifications forming, with both radiolucent and radiolucent areas.
▪ Dentingerous cyst, ameloblastoma, and OKC are NO LONGER in the differential diagnosis.
This is clearly AOT
_(_Adenomatoid odontogenic tumor)

Adenomatoid odontogenic tumor
(AOT)
Swelling in maxillary vestibule

Adenomatoid odontogenic tumor
(AOT)
fibrous capsule of AOT is at least partially encapsulated.
Easy to remove; “popped right out”.

Adenomatoid odontogenic tumor
(AOT)
An expansion into lingual area as well as into vestibule

Adenomatoid odontogenic tumor
(AOT)
Snowflake‐like calcifications within mixed, well‐circumscribed radiolucency

Adenomatoid odontogenic tumor
(AOT)
- Teardrop shape / inverted pear between roots of teeth.
- Well-circumscribed, corticated margin & snowflake‐like calcifications within
What is a malignant ameloblastoma?
▪ Malignant ameloblastoma
o Primary lesion and metastasis have normal welldifferentiated
ameloblastic (benign) histology
o Most commonly to lung
CALCIFYING EPITHELIAL ODONTOGENIC TUMOR
CEOT
also known as ?
Pindborg Tumor
Calcifying Epithelial Odontogenic Tumor
(CEOT)
▪ Uncommon (~1% of odontogenic tumors)
▪ Does not have inductive effect
Calcifying Epithelial Odontogenic Tumor
(CEOT)
Demographics and Location
o 2nd to 10th decades, peak ~ 4th decade
o MD (mandibular) 2 : 1 MX (maxillary)
o Usually posterior mandible
Calcifying Epithelial Odontogenic Tumor
(CEOT)
Clinically
- Presents as painless slowly expanding swellings
- sessile swellings of the gingiva or alveolus ( 2 times more on mandible than maxilla
- Peripheral lesion may be seen, but are rare
Calcifying Epithelial Odontogenic Tumor
(CEOT)
Radiographically
- May be unilocular, but most commonly as a multilocular lesion
- May be entirely radiolucent or a mixed radiolucent-radiopaque lesion
-
Often associated with an unerupted tooth
- MD third molar most common
- Calcifications in the lesion, if present, are typically prominent around the crown of the impacted tooth.

In addition to fracture, there is semilunar loss of bone around the molars ► (SOT)
Squamous Odontogenic Tumor

SOT
Squamous Odontogenic Tumor
- Semilunar loss of bone.
- Alveolar bone is gone due to impacted canine that is visible
Calcifying Epithelial Odontogenic Tumor
(CEOT) have clinical presentation similar to what lesion?
- CEOT clinically is similar to ameloblastoma
- Also, CEOT has potential to be locally invasive, if in the right anatomic location, but has a less aggressive biologic behavior compared to ameloblastoma
Calcifying Epithelial Odontogenic Tumor
(CEOT)
Treatment
▪ Enucleation _with peripheral ostectom_y
▪ Resection with rim of normal bone
▪ Recurrence rate is ~12%
▪ ~ 2% demonstrate malignant transformation

Central odontogenic fibroma (COF)
- well‐circumscribed radiolucency posterior to molar

Central odontogenic fibroma (COF)
round mass of opacity due to FCT. Ground glass‐like appearance
Adenomatoid odontogenic tumor
(AOT)
Demographics and Location
▪ 2/3 anterior jaws
▪ 2/3 females
▪ 2/3 associated with an impacted canine
▪ 2/3 MX
▪ 2/3 2nd decade – kids and teenagers\
That’s why it’s known as the tumor of two thirds
▪ ~ 3‐7% of all odontogenic tumors
New research showing more in _ant md_ though
Adenomatoid odontogenic tumor
(AOT)
Clinical charcterstics
- Frequently asymptomatic, discovered upon routine radiographic exam or when lesion becomes large enough to expand bone
- Tumor of Epithelial Origin
Adenomatoid odontogenic tumor
(AOT)
Radiographically
▪ ~ 75% are well‐circumscribed unilocular radiolucency involving the crown of an unerupted tooth
o less often, they are found between the roots of teeth
▪ Mixed radiolucent/radiopaque appearance is likened to “snowflake” calcifications
▪ May be totally radiopaque in some cases
▪ Divergence of roots is frequently seen
If an Adenomatoid odontogenic tumor (AOT) is not showing any calcifications yet, it’s in the differential
diagnosis with —— ?
a dentigerous cyst.

Odontogenic Myxoma
- Classic example of enlargement of the mandible caused by multilocular radiolucency.
- Enlarged into oral cavity ‐ alveolar ridge elevated

Odontogenic Myxoma
Case

Clinically: obliteration of vestibule on patient’s left mandible
Radiographically:lesion running from posterior by third molar all the way anterior to canine. Well‐circumscribed, multilocular radiolucency is scalloping up
between teeth, causing some root divergence
Grossly: gelatinous appearance of myxoma makes it hard to remove
After treatment: post‐surgery; had excised all the way to right 2nd PM
This is Odontogenic Myxoma
Adenomatoid odontogenic tumor
(AOT)
Treatment
- Treatment is usually enucleation
- recurrence is rare

CEMENTOBLASTOMA
(True Cementoma)
- First molar has tumor attached to the root.
- Mostly radiopaque but has some less radiodense areas within = classic for cementoblastoma.
- Radiolucent halo around region.
Cementoblastoma
Grossly continuous growth from tumor to the root of the tooth. Brownish
areas were more vascular.
Histologically: tubular dentin in tooth, attached to mass of tissue with calcifications
Squamous Odontogenic Tumor
(SOT)
Demographics and Location
▪ Typically involves alveolar ridge
▪ Anterior > Posterior jaws
▪ Seen from 2nd to 7th decade (mean 40 years of age)
Squamous Odontogenic Tumor
(SOT)
Clinical charcterstics
- Tumor of Epithelial Origin
- Rare
- Usually asymptomatic, but may present with tooth mobility and slight pain
-
Multiquadrant ~ 20-25%
- A couple reported cases in families
Squamous Odontogenic Tumor
(SOT)
Radiographically
-
Well‐circumscribed radiolucency , often a semilunar radiolucency of alveolar ridge
- Can mimic periodontal disease
Squamous Odontogenic Tumor
(SOT)
Origin
- Thought to arise from epithelial rests (Malassez) in the periodontal ligament space
Squamous Odontogenic Tumor
(SOT)
Treatment
- Treatment is conservative local excision
- Recurrence is rare
Squamous Odontogenic Tumor SOT
Histologically may be mistaken for what other lesions?
- Ameloblastoma
- Squamous cell carcinoma (SCCa)
Compound Odontoma
Vs
Complex Odontoma
Compound Odontoma
- Mature normal appearing pulp, enamel and dentin
- Organization like teeth, with enamel surrounding dentin which surrounds pulp ( Well developed rudimentary “tooth” forms)
- appear as small tooth‐like structures in the Anterior jaws (esp. MX)
Complex Odontoma
- Mature pulp, enamel and dentin
- No organization, mass of dentin and enamel matrix and pulp tissue (**Poorly developed mass of calcified deposits)
- appear as masses of radiopaque material with
- variable densities in the Posterior jaws (esp. MD)


Classic appearance of Odontoma
- multiple tooth‐like shapes aggregated together
- Typically with some sort of radiolucent halo around them

Compound Odontoma
little teeth‐like structures blocking canine eruption

Complex Odontoma
- 2‐2.5cm mass overlaying the molar.
- radiolucent rim/halo that is mixed, mostly radiopaque
Central odontogenic fibroma (COF)
also known as ?
- *Odontogenic Fibroma
(central) **
Central odontogenic fibroma
(COF)
Origin
- Tumors of Mesenchymal Origin
- Some believe represents the counterpart to the peripheral ossifying (odontogenic) fibroma (in soft tissue)
Central odontogenic fibroma
(COF)
Location
- MX ≈ MD
- lesions in MX tend to be anterior to first molar
- those in MD anterior ≈ posterior
- 1/3 associated with an unerupted tooth
Case

Primordial
Odontogenic Tumor
(POT)
unilocular radiolucency
Central odontogenic fibroma (COF)
Clinically
-Small lesion tend to be asymptomatic
-Larger lesions can cause cortical expansion and tooth mobility
Central odontogenic fibroma
(COF)
Radiographically
-
Small lesions tend to be well-circumscribed unilocular radiolucencies
-
often periradicular
- can mimic periapical granulomas and cysts
-
often periradicular
- Larger lesions tend to be well-circumscribed multilocular radiolucencies
- Borders are usually sclerotic
- Root resorption or divergence may be seen
- ~ 10- 15% will show radiopaque flecks within the radiolucency
Central odontogenic fibroma
(COF)
Treatment
- Enucleation with curettage or excision
- usually don’t recur

Ameloblastic Fibroma
(AF)
1‐3 potential locules, no impacted tooth associated
What is the Microscopic Differential Diagnosis of Central odontogenic fibroma (COF)?
o Desmoplastic fibroma ‐ a more aggressive lesion
o Fibromyxoma ‐ variant of odontogenic myxoma with
abundant collagen
o Hyperplastic tooth follicle ‐ typically loose immature stroma, but when hyperplastic can have abundant collagen

Ameloblastic Fibro-odontoma (AFO)
- well‐circumscribed radiolucency
- corticated edge + calcification

Ameloblastic Fibro-odontoma (AFO)
has expansion into oral cavity. Flecks of calcification
in lesion with impacted tooth = odontoma
Odontogenic Myxoma
Origin
- Tumors of Mesenchymal Origin
- Thought to arise from the tooth follicle or dental papilla
Odontogenic Myxoma
Demographics and Location
- ~3-5% of all odontogenic tumors
- Wide age range, but 3rd decade most common
- Found anywhere in the MD or MX
Odontogenic Myxoma
Radiographically
- Small lesions present as asymptomatic radiolucencies found upon routine exam
- Larger lesions can cause painless expansion of bone
- All are radiolucent lesions, but the appearance can vary from well‐ circumscribed to irregular and diffuse
- Unilocular to, more commonly, multilocular (“soap bubble” or “honeycomb”) radiolucency
-
Borders are often scalloped, can see sc_alloping around the roots of teeth_
- But can cause displacement of teeth and resorption of the roots of teet
Odontogenic Myxoma
Grossly
- the tumor is described as loose, soft and gelatinous
Ameloblastic Fibrosarcoma
in the mandible developed after two years from AF
Odontogenic Myxoma
Treatment
- Surgical excision or resection
- Because the lesion is not encapsulated and has a gelatinous loose consistency► it is difficult to remove completely
- this is thought to be why myxoma has a fairly high recurrence rate
- Maxillary posterior lesions should be treated more aggressively
CEMENTOBLASTOMA
Origin
(True Cementoma)
- Tumor of Mesenchymal origin
- Benign tumor of cementoblasts
CEMENTOBLASTOMA
Demographics and Location
(True Cementoma)
CEMENTOBLASTOMA
(True Cementoma)
Clinically
- 2/3 of cases have pain and swelling
- Can cause cortical expansion if large enough
CEMENTOBLASTOMA
(True Cementoma)
Radiographically
- Radiopaque mass fused to the root of the affected tooth
- Usually has a thin radiolucent halo or rim surrounding the radiopacity
CEMENTOBLASTOMA
Treatment
(True Cementoma)
- surgical extraction of the involved tooth with attached tumor
- Root amputation (with attached tumor) and endo is an option for smaller lesions
- Recurrence is unlikely
CEMENTOBLASTOMA
(True Cementoma)
Cementoblastoma has similar histologic presentation to what?
osteoblastoma
Difference is Osteoblastoma is NOT a_ttached to the root of a tooth_ (whereas cementoblastoma must be)
What are Odontogenic Tumors
of
Mixed Origin
(Epithelial and
Mesenchymal)
They are tumors in which the _odontogenic epithelial componen_t causes induction of the mesenchymal component to produce a product
Examples:
- Odontomas
- Ameloblastic fibroma
- (and Ameloblastic fibrosarcoma)
- Ameloblastic fibro-odontoma
Odontoma
Origin
- Odontogenic Tumors of Mixed Origin (Epithelial and Mesenchymal
- They are hamartomas rather than true neoplasms
- They are masses of enamel and dentin with variable amounts of pulp and cementum
What is the most common odontogenic “tumor”?
Odontoma
Odontoma
Demographics and Locations
▪ First 2 decade most common (mean age of 14)
Location is based on the type of Odontoma
-
Compound Odontoma
- Anterior jaws (esp. MX)
- **Well developed rudimentary “tooth” forms
-
Complex Odontoma
- Posterior jaws (esp. MD)
- **Poorly developed mass of calcified deposits
Odontoma
Charcterstics
- Often associated with an unerupted tooth
- Lesions may prevent eruption of teeth
- Usually small in size, but rare cases of > 6cm reported
- large lesions can cause bone expansion
Odontoma
Radiographically
▪ Radiographically see a radiopaque structure(s) surrounded by a radiolucent rim
▪ As with any calcified lesion, those found early in development may appear totally or predominantly radiolucent
▪ Compound odontomas appear as small tooth‐like structures
▪ Complex odontomas look like masses of radiopaque material with variable densities
Odontoma
Treatment
▪ Simple excision or enucleation
▪ Unlikely to recur
Primordial
odontogenic tumor
(POT)
Origin
- Tumor of mixed origin
- Very rare! first reported in 2014 -less than 30 cases so far
Primordial
odontogenic tumor
(POT)
Demographics and Location
- Most common in 1st and 2nd decades
- Mean age 12.5 years
- MD:MX 6:1
Primordial
Odontogenic Tumor
(POT)
Clinical Charcterstics
- Asymptomatic found on routine imaging
- Can cause tooth displacement and cortical expansion
Primordial
Odontogenic Tumor
(POT)
Radiographically
-
Well-defined radiolucency associated with an impacted tooth
- Most commonly a third molar
Primordial
Odontogenic Tumor
(POT)
Treatment
- conservative excision/enucleation
- So far no recurrence
Ameloblastic fibroma (AF) and ameloblastic fibro-odontoma (AFO)
Charcterstics
- Uncommon benign mixed odontogenic neoplasms.
- Considered together because it is thought they are variations of the same process
Ameloblastic fibroma (AF) and ameloblastic fibro-odontoma (AFO)
demographics and location
- Typically presents in first 2 decades
- mean is 12 years of age
- ~ 70% occur in the posterior mandible
- ~ 75% associated with unerupted teeth
Ameloblastic Fibroma (AF)
clinical and radiographic presentations
- Small lesions are asymptomatic and found on routine exam
- Large lesions can cause bone expansion
- Smaller lesions are unilocular Radiolucencies
- Large ones are multilocular radiolucencies
- Border is well defined and often sclerotic
- Untreated, can grow to very large size
Ameloblastic Fibro-odontoma (AFO)
Clinical and Radiographic features
- Clinical features similar to Ameloblastic Fibroma AF (Small lesions are asymptomatic and found on routine exam
& Large lesions can cause bone expansion)
Radiographically, we see a mixed radiolucent/radiopaque lesion because of the formation of odontomas
Ameloblastic fibroma (AF) and ameloblastic fibro-odontoma (AFO)
Treatment
-
Conservative surgical excision or curettage,
easily removed from surrounding bone - Prognosis is excellent, recurrence is unusual
- ▪ Rare cases reported of development of ameloblastic fibrosarcoma in area of AF or AFO
Ameloblastic
Fibrosarcoma
Charcterstics & Origin
- _Malignant counterpar_t of ameloblastic fibroma
- Rare lesion which may arise in the site of a previous AF/AFO or arise de novo
Ameloblastic
Fibrosarcoma
Demographics and location
- 1.5 times more common in males
- ~ 80% MD
Ameloblastic
Fibrosarcoma
Clinically
- Pain, swelling and rapid growth are common presenting signs
Ameloblastic
Fibrosarcoma
Radiographically
- presents as an ill-defined destructive radiolucency with irregular borders
Ameloblastic
Fibrosarcoma
Treatment
- Radical surgical excision as the tumor is very aggressive and infiltrative
- Prognosis is dependent on complete removal of tumor
Odontogenic carcinomas
List them (5)
-Ameloblastic carcinoma
-Primary intraosseous carcinoma, NOS
-Sclerosing odontogenic carcinoma
-Clear cell odontogenic carcinoma
-Ghost cell odontogenic carcinoma
All fairly rare lesions!
What is the Differential Diagnosis D/D of Multilocular Radiolucency
MOCHA
- M odontogenic Myxoma
- O Odontogenic keratocyst
- C Central giant cell granuloma
- H Central Hemangioma
- A _A_meloblastoma
Others:
- Aneurysmal bone cyst
- early CEOT
- ameloblastic fibroma AF
- central MECa
Key Concepts of
Malignant Lesions on
Imaging

Rapidly growing and infiltrative
–finger-like extensions into surrounding anatomy
Remember: in some instances, a benign lesion can mimic a malignant
one.
Therefore we should be wary of all the information that is available.
Key Concept of
Malignant Lesions on
Imaging

ill-defined invasive borders followed by bone destruction
Key Concept of
Malignant Lesions on
Imaging

Destruction of the cortical boundary (floor of maxillary antrum) with an adjacent soft tissue mass (arrows)
Key Concept of
Malignant Lesions on
Imaging

Tumor invasion along the periodontal membrane space causing irregular thickening of this space
Key Concept of
Malignant Lesions on Imaging

Multifocal lesions located at root apices and in the papilla of a developing tooth destroying the crypt cortex and displacing the developing tooth in an occlusal direction (arrow)
Key Concept of
Malignant Lesions on Imaging

Four types of effects on cortical bone and periosteal reaction, from top to the bottom:
•cortical bone destruction without periosteal reaction
•laminated periosteal reaction with destruction of the cortical bone and the new periosteal bone
•destruction of cortical bone with periosteal reaction at the periphery forming Codman’s triangles
•a spiculatedor sunray type of periosteal reaction
Key Concept of Malignant Lesions on Imaging

Bone destruction around existing teeth, producing an appearance of teeth floating in space.

Chondrosarcoma
- its consistent widening as opposed to seen in periodontitis and inflammatory disease
Case
CC of loose teeth wanted extractions and a
denture

Chondrosarcoma
- Ill defined lesion of anterior maxilla
- Areas of radiolucency
- Classic area of moth‐eaten look
- Circular area of radiolucency with trabecular
- pattern
- Patient left without surgery, not heeding medical advice
Then patient came back
▪ Someone was willing to do the dentures for her
▪ CC‐ denture was not fitting
▪ Expansion of cortical plate
▪ Hyperkeratotic because of denture rubbing
▪ Still has malignancy
▪ Advise for surgery
▪ Refused again
Then the lesion kept on Lesion still growing
▪ Metastasize to lungs
▪ Admitted to breathing issues
▪ About 5 ½ years from initial dx to
pt passing away

Chondrosarcoma
- Alveolar process and floor of mouth affected
- Limitations of movement of the tongue
Case
- 83 year old female with nodular areas under denture on anterior mandibular ridge
- ▪ c/c of her denture rocking

Can see in the anterior region there’s an
elevation
histology shows it’s not chondrosarcoma
because it contained Cutright lesion
papule or nodule on alveolar ridge
- Osseous and/or chondromatous metaplasia within the soft tissue of the gingiva
o Lesion is NOT central in bone or connected to bone
▪ NOT a malignant lesion
o Thought to be reactive metaplasia due to a poorly fitting denture
Chondroma & Chondrosarcoma
- *Chondroma –** benign
- *Chondrosarcoma**‐ malignant
- Both are listed here because
- a benign cartilaginous tumor central In the jaw is extremely rare (or may not exist)
- Lesions tend to recur many times and eventually metastasize ( Basically chondromas are not really benign)
Chondrosarcoma
Charcterstics
- Malignant tumor that forms cartilage
- 10% of all primary bone tumors, but rare in the jaws

Osteosarcoma
▪ Swelling on left side of face
▪ Difficult opening

Osteosarcoma
- See something in the operculum
- Infection in third molar?

Osteosarcoma
- AP Plain Film
- Most of jaw was missing
- Radiolucency affecting entire ramus and condyle

Osteosarcoma
- Classic sunburst pattern
- Fuzzy appearance on outer edges of cortex

Osteosarcoma
- cloudy bone formation on surface of cortex on facial and lingual aspect

Osteosarcoma
a patient with swelling with side of face

Osteosarcoma
▪ Lytic lesion
▪ Slightly ill defined
▪ Loss of bone in the inferior aspect of mandible
Chondrosarcoma
Clinical presentations
- Patient’s chief complaint is painless swelling, may be associated with tooth mobility
-
Symmetric widening of the PDL space
- Can be initial presentation with chondrosarcoma and osteosarcoma
-
Along radicular surface of the tooth there is the same rate of widening all the way down the tooth
- In contrast to periodontal disease, where there is a triangular shaped loss of space
Chondrosarcoma
Radiographically
-
Poorly defined radiolucency, often with scattered radiopaque foci
- Radiopaque foci can be seen since the cartilage in the tumor can ossify
Chondrosarcoma
Treatment
-
Radical surgical excision on initial treatment
-
Maxillectomy/Mandibulectomy
- If anterior region they remove the entire anterior portion of the jaw
-
Maxillectomy/Mandibulectomy
- These lesions don’t respond to radiation or chemotherapy
- Although used as adjuncts for lesions that can’t be treated surgically
-
For example a posterior sinus lesion since that is the base of the skull
- These patients have poorer prognosis than those with more accessible sites such as the mandible
- Prognosis is poorer than for osteosarcoma (which contrasts with the prognosis in extragnathicsites)
- Treatment failure (and mortality) is usually due to uncontrolled local disease not metastasis
Why any diagnosis of chondroma in the jaws should be viewed with suspicion?
- Since 20% of chondrosarcomas of the jaw are initially misdiagnosed as chondromas ► any diagnosis of chondromain the jaws should be viewed with suspicion
-
All cartilaginous tumors arising in the jaws should be excised widely
- (>60% of cartilaginous tumors of the jaw recur and ~7% metastasize to the lung and/or bone )
Osteosarcoma
_Demographics & Location_MD > MX, Male > Female
- Most common malignant bone tumor in the jaws is metastatic disease
-
Most commonly primary (meaning started at this location) malignant bone tumor in patients under 40 years old
- 2nd most common overall after multiple myeloma
-
Mean age at presentation for jaw lesions is 33 years old, 10‐15 years older than that for long bones
*
Osteosarcoma
Clinically & Radiographically
- Swelling and pain are the common presenting symptoms (25% have “toothache”)
- Can also have loosening of teeth,** **paresthesia of lip** and **nasal obstruction
- Symmetric widening of the PDL is often an early radiographic change
- Lesions vary from dense sclerotic, mixed sclerotic and radiolucent to all radiolucent
Osteosarcoma
Treatment
- Important to distinguish from chondrosarcoma as treatments are different
- Osteosarcoma is currently treated with pre-op multi-agent chemotherapy followed by surgery
-
Radiation therapy alone is insufficient for cure
- Favorable jaw site – MD symphysis
- Worst site – MX sinus
- 5 year survival is ~ 20% (up to 80% if caught early and treated with radical resection)

Langerhans Cell
Disease
Infant with Acute disseminated type
▪ See lesions on head/ear

Langerhans Cell
Disease
we see lesions on maxilla

Langerhans Cell Disease
▪ Older child
▪ Chronic disseminated form
▪ Alveolar ridge involvement
▪ Lot of bone loss and mobility
▪ Painful to brush

Langerhans Cell Disease
Torus and molar involvement

Eosinophilic
Granulations
Erythematous area

▪ Child with disseminated form
▪ Punched out radiolucency in the skull

▪ Child with bone loss surround the teeth
▪ Floating teeth
disseminated form

▪ Floating teeth
▪ Only attached by soft tissue due to extensive bone loss
disseminated form

Eosinophilic granuloma
Peripheral (juxtacortical) Osteosarcoma
Location
- Arise on the surface of the bone (vs. medullary site for usual forms of osteosarcoma)
- Usually long bones
What are the two types of Peripheral (juxtacortical) Osteosarcoma ?
parosteal – well differentiated, but will recur with less than an en bloc or radical surgery
periosteal – higher grade with prominent cartilaginous component
Parosteal Peripheral Osteosarcoma
Charcterstics
o Mushroom like growth on bone surface
o No elevation of periosteum
o No new bone formation
o Low grade
Periosteal Peripheral Osteosarcoma
Charcterstics
o Usually sessile growth on bone surface
o Elevation of periosteum
o New bone fills in space under periosteum
o Prognosis is better than medullary osteosarcoma but worse
thanparosteal type
Langerhans Cell
Disease
also known as
?
- Histiocytosis X (old name)
- Langerhans cell granuloma
- Eosinophilic granuloma
- Langerhans cell histiocytosis
Langerhans cell histiocytosis
Etiology
Etiology unclear
o Demonstration that LCH cells are clonal, along with the recent discovery of activating BRAF mutations in LCH cells, ►strongly suggests that LCH is a neoplastic disease
Langerhans cell histiocytosis
Demographics & Location
- Males>>> Females
- More than half of cases seen under the age of 10
- Jaw affected in 10 ‐20% of cases
Langerhans Cell
Histiocytosis
Clinically & Radiographically
Clinically:
Common sites: skull, rib, vertebrae, and mandible
▪ Often have associated pain or tenderness
Radiographically:
▪ In jaws we see loss of alveolar bone in molar area
o Mimics severe periodontitis

- Punched out radiolucency
- Lytic radiolucency without cortication
MM
Multiple Myeloma

- more punched out radiolucency in iliac crest in the image
- Bone marrow biopsy usually done in this area since it’s frequently involved
multiple Myeloma
MM

Multiple Myeloma
▪ Radiolucency without sclerotic border
▪ Multiple and separated

Swelling of gingiva
▪ Plasmacytoma
Types of Langerhans Cell
Disease
List 3
▪ Acute disseminated form (Letterer‐Siwe disease)
▪ Chronic disseminated form (Hand‐Schuller‐Christian Disease,
▪ Eosinophilic Granuloma (chronic localized)
Acute disseminated form (Letterer‐Siwe disease)
charcterstics
- Multisystem (bone, skin, liver spleen and lymph nodes)
- Infants
- high mortality
- rapidly progressive
Chronic disseminated form (Hand‐Schuller‐Christian Disease, Multifocal Eosinophilic Granuloma)
Charcterstics
- Unisystem (frequently bone, but also skin and viscera)
- Children
- fairly high mortality
- more chronic progression
Eosinophilic Granuloma (chronic localized)
Charcterstics
- Solitary or multiple bone lesions without visceral involvement
- Adults
- very low mortality
- Some reports of association with smoking marijuana
- In these cases the lungs are involved

Ewing Sarcoma
▪ Long bone
▪ Large expansion

Ewing Sarcoma
- an _expansion of tissu_e
- Dissolution of bone in that area
The site of invovelement of Langerhans Cell
Disease depends on ?
Site of involvement depends on clinical form
- Neoplastic proliferation of Langerhans cells
- Langerhans cells
- Dendritic mononuclear cells normally found in the epidermis and mucosa
- Antigen presenting cells to T lymphocytes
- Langerhans cells

Metastatic Carcinoma to Jaw Bones
▪ A. Metastatic breast carcinoma surrounding the apical half of the second and third molar roots and extending inferiorly. It has destroyed the inferior border of the mandible.

Metastatic Carcinoma to Jaw Bones
B. Bilateral metastatic lesions from the lung destroying the mandibular rami.

Metastatic Carcinoma to Jaw Bones
D. Destruction of the left mandibular condyle (arrows) from a thyroid metastatic lesion

Metastatic Carcinoma to Jaw Bones
A. Partial panoramic image of prostate metastatic lesions involving the body and ramus; note the sclerotic bone reaction (arrows).

Metastatic Carcinoma to Jaw Bones
B. Occlusal image of prostate lesions causing sclerosis and spiculated periosteal reaction (arrows)

Metastatic Carcinoma to Jaw Bones
C. Periapical image of a metastatic lesion of breast carcinoma; note the irregular widening of the periodontal membrane spaces and patchy sclerotic bone reaction, especially around the roots of the molars
Chronic disseminated form (Hand-Schuller-Christian Disease, Multifocal Eosinophilic Granuloma)
Has a classic Triad?
- Exophthalmus
- Diabetes insipidus
- Lytic defects of bone
Chronic disseminated form of Langharan Disease
Clinically and radiographically
Clinically:
- we see mobility of teeth
Radiographically:
- picture of child with “teeth floating in air”
- Sharply punched out radiolucent lesions, ill- defined radiolucency in some cases
Eosinophilic Granuloma
Charcterstics & Demographics
- Elderly men often present with lung lesions (increased incidence with smoking)
- Localized lesions, usually affecting one bone
- If found to be an accessible solitary lesion, treatment is usually curettage and possibly low dose RT
- in some instances it can be initial presentation of systemic disease – but that would typically be in children or young adults
What is the Differential Diagnosis
for
Langerhans Cell
Histiocytosis
Histology
It contain rod shape called
Birbeck granules
What is the differential diagnosis for Alveolar Bone Loss in Children?
o Juvenile periodontitis
o Langerhans cell histiocytosis
o Papillon‐Lefevre syndrome
o Cyclic neutropenia/agranulocytosis
o Burkitt’s Lymphoma
Multiple Myeloma
charcterstics
Monoclonal Expansion of malignant plasma cells
- Plasma cells make a lot of immunoglobulin ► So we will see a lot of immunoglobulin
Multiple Myeloma
Demographics and Location
- Most common in 40‐70 year old
- Means 63 years old
- Bones most commonly involved include ribs, vertebrae and skull
- 70‐90% will have jaw involvement at some point
Multiple Myeloma
Clinically
- Present with bone pain (>70%) and pathologic fractures
- Anemia, thrombocytopenia and neutropenia due to crowding out of normal cells within bone marrow by proliferating malignant cells
- 50‐60% have Bence‐Jones proteins in urine (light chains, usually kappa)
▪ Solitary plasmacytoma Vs Extramedullary plasmacytoma Vs Multiple myeloma – multifocal disseminated disease
▪ Solitary plasmacytoma
-
Individual lesion in bone
- When affecting oral cavity, ~95% of the cases are ramus and angle of the mandible
- In many cases p_rogress to more systemic disease_
Extramedullary plasmacytoma
- individual soft tissue lesion (not central In bone)
Multiple myeloma
- multifocal disseminated disease
Multiple Myeloma
Radiographically
- “punched out” radiolucencies (no sclerotic margin) often with an irregular outline
Multiple Myeloma
Lab findings
- Elevated M spike in serum
- Elevation of immunoglobulin in serum (hyperglobulinemia) most commonly IgG
- Deposition of amyloid in tissues (macroglossia)
Multiple Myeloma
Treatmet
Treatment can include :
- chemotherapy with or without Radtiaion Therapy
- bone marrow transplant
- interferon
- antibodies made against tumor cells
- thalidomide
- Even with treatment, many patients do not survive more than 18‐24 months, however treatment modalities are improving
- Older patients are treated less aggressively
Ewing Sarcoma Ewing’s family of sarcomas
Charcterstics
▪ Highly malignant, undifferentiated, small round cell tumor/small blue cell tumor
o The cell of origin is in question, may be of neural crest origin
Ewing Sarcoma
Demographics and Location
- Primarily a disease of children and adolescents (90% of patients are between 5 and 30 years old) ▪ >60% males ▪
- Twice as common in mandible
- Caucasians>>>>Blacks and Asians
- Make up ~6% of primary malignant bone tumors
- In the jaws, the ratio of primary tumor to metastasis is 14 to 1
- 50% of cases in the femur and pelvic bones
- ~1% occur in the jaw bones
Ewing Sarcoma
Clinically
- Patients often present with pain, swelling, fever and elevated ESR (similar to signs of inflammation)
- May be misdiagnosed as an infection or osteomyelitis
- Paresthesia and loosening of teeth are common findings with jaw lesions
Ewing Sarcoma
Radographically
- an irregular lytic lesion with ill‐defined margins
- Root resorption may be seen
- May see thickening of the periosteum with a characteristic “onion skinning” pattern (like with peripheral periostitis)
- seen more in long bones
Ewing Sarcoma
Treatment
- Combined therapy with multi‐agent chemotherapy, radiation therapy and surgery has led to 40% ‐ 80% survival rates
- Gnathic Ewing sarcoma has a lower mortality rate than all other primary sites
What are the most common carcinomas that metastasize to the jaw
The most common carcinomas to jaw: Breast Lung Thyroid and Colon Kidney Prostate ▪
“B. L. T. and Cold Kosher Pickle”
Malignant tumors of jaw
Review
Metastatic tumors to the jaw are more common than primary lesions
● Think osteosarcoma, chondrosarcoma, or osteoblastic metastasis (breast or prostate) if lesion radiographically looks malignant and has radiopaque internal pattern
● Ewing’s sarcoma is clinically accompanied by signs of inflammation
●Multiple myeloma characteristically presents as multiple, well‐ defined, punched‐out radiolucencies
● Bone affected by Non‐Hodgkin’s lymphoma radiographically appears to be dissolving
● Langerhans cell histiocytosis characteristically presents as scooped‐ out radiolucencies at the mid‐root level
● Remember to include metastatic carcinoma to jaw as a radiographic differential diagnosis for malignant lesions
Hyperparathyroidism
What is it?
What are its types?
What is it?
- Excess of circulating parathyroid hormone important in formation of osseous structures
- Increase bone remodeling but tips the balance of osteoblastic and osteoclastic activity in favor or osteoclastic resorption
- it’s a systemic endocrine disease
What are its types?
o Primary hyperparathyroidism Type 1
▪ Uncontrolled parathyroid hormone production by
parathyroid neoplasm (adenoma >> hyperplasia >
adenocarcinoma)
o Secondary hyperparathyroidism Type 2
▪ Continuous parathyroid hormone production in
response to chronic low serum calcium levels
▪ Renal osteodystrophy
Which systemic disease is this?

Hyperparathyroidism
Here we see we see
- a granular appearance of the max and mand bone everywhere, it is not localized.
- There is a loss of bone density and the loss of definition of cortical bone.
- Here we see a loss of definition of lamina dura as well because it is now granular, and is not as clear.
Which systemic disease shows radiographically like this ?

Hyperparathyroidism; this is the brown tumor which is sometimes well or ill defined, multi or unilocular radiolucency with granular septation.
If you have a patient that is younger than 15-20 years old that has a central giant cell granuloma ► you have to check that patient for hyperparathyroidism, because it could be a brown tumor.
Which systemic disease shows radiographically like this ?

This is another medical CT scan. You see the granular appearance of
the maxilla, skull, and well-defined multilocular radiolucency with
granulation. We call this a brown tumor because it is associated with
hyperparathyroidism.
( systemic endocrine diseases)
Which systemic disease shows radiographically like this ?

Hyperparathyroidism
On our intraoral radiographs, we see loss of definition of lamina dura because the bone now has a granular appearance which extends to the lamina dura.
The teeth are usually normal, but there is a loss of lamina
dura around the teeth. These teeth are not mobile.
Which systemic disease shows radiographically like this?

a medical CT scan of a patient with secondary hyperparathyroidism.
We see a lack of cortical bone – no normal cortical bone. Inside the skull
we have a granular appearance, with radiolucent and radiopaque dots, we call this a salt and pepper dots.
This is why we call this a salt and pepper appearance, there is no normal cortical bone.
( systemic endocrine diseases)
Which systemic disease shows radiographically like this?

we have 2 Pas of patients
with pseudohypoparathyroidism.
- hypoplasia of enamel, tooth material
- hypoplastic tooth bud ( hypoplastic means arrested development)
- delayed eruption,
- external root resorption.
Which systemic disease shows radiographically like this?

Acromegaly (Hyperpituitarism)
- enlargement of the mandibular bone with a high degree of enlargement
- a class III appearance
- enlargement of sella tursica because of the pituitary gland enlargement
Which systemic disease manifests radiographically like this?

Dwarfism
- hypopituitarism*
- We see* multiple dental anomalies: hypodontia, radicular fusion, fused roots of left lateral incisor and left canine and impacted permanent teeth.
- (from google)*
Hyperparathyroidism
Radiographic features
▪ Stones, bones, moans, and groans
▪ Radiolucent appearance (generalized osteopenia) What we see in the bones is one of the earliest radiographic features that we see = sudden erosions in the phalanges in the bones of the hands followed by mineralization of the skeleton including max and mand, skull base. As a
result, you have generalized osteopenia. 10% of these patients have brown tumors
▪ Brown tumors: Brown tumors are the same as central giant cell granulomas. When they are associated with hyperparathyroidism, we call them brown tumors.
▪ Punctate or nodular calcifications in the joints and kidneys =stones
▪ Entire calvaria has a granular appearance classically known as the “salt and pepper” skull as a result of the generalized osteopenia, we have this granular appearance in the skull
Which systemic disease shows radiographically like this?

Osteoporosis
- reduction in bone density,
- larger bone marrow spaces.
We need more tests to confirm osteoporosis besides dental radiographs.
Hypoparathyroidism
Radiographic features
What is Hypoparathyroidism:
Insufficient secretion of PTH
o Damage or removal of the parathyroid glands during thyroid surgery
Principal radiographic change: calcification of the basal ganglia
Sometimes we have pseudohypoparathyroidism. This happens when we have a normal amount of PTH, but there is something wrong with the response of the target tissue. So, we have normal PTH but abnormal response to PTH.
dental enamel hypoplasia, external root
resorption, delayed eruption, or root dilaceration
Which systemic disease shows radiographically like this?

medical CT scan with a patient with osteopetrosis- very dense. Not a
nice definition of the cortical bone. We see decreased in size of skull
foramina.
Which systemic disease shows radiographically like this?

pt with Osteopetrosis
we see
Hypovascular bones so they are more prone to osteomyelitis. This is a sign of sequestrum which is a sign of osteomyelitis.

pt with Osteopetrosis
- Generalized increase in bone density, increased trabeculation, loss of large bone marrow spaces.
- These patients are more prone to osteomyelitis because they are Hypovascular.
- We have to be careful in extractions because they don’t have the same vascularity as other healthy patients have.
- We see an onion skin appearance by the white arrow.
Hyperpituitarism
What is it?
What is its types
What is it?
- Hyperfunction of the anterior lobe of the pituitary gland caused by a benign functioning tumor of the anterior lobe
- it’s a systemic endocrine disease
What is its types ?
▪ Types based on age of onset
- Gigantism happens in children, generalized overgrowth of most long bones, hard and soft tissue. These patients are usually very tall. Proportion in these patients may be normal, but very large appearance.
- Acromegaly Increased hyperfunction in adult patients. In these patients, the epiphysis of the long bones already closed, you can see in the mand or max. One of the observable features is enlargement of the whole mandible/skull/sinuses/soft tissue. Patients usually present with “My hat is not fitting anymore, my denture is not fitting anymore”
Hyperpituitarism
Radiographic
Features
▪ General features
- Enlargement (ballooning) of the sella turcica
- Enlargement of the paranasal sinuses (especially the frontal sinus)
- Thickening of the outer table of the skull
▪ Jaws
- Enlargement of the jaws, most notably the mandible
- Class III skeletal as a result of the mandible enlargement with growth centering in the condylar head
▪ Teeth and associated structures
- Spacing of the teeth, enlargement of tongue, it could result in spacing of teeth in the anterior region
o Hypercementosis the forces are higher now
- so you may see Hypercementosis
- Hypercementosis is excessive deposition of non-neoplastic cementum over normal root cementum, which alters root morphology. This cementum may be either hypocellular or cellular in natur*
Which systemic disease has this radiographic manifestation?

Ricket / Osteomalacia
hyperplasia or thinning of mineralization of teeth. We
can see hyperplasia of enamel in patients.
Hypopituitarism
What is it?
What is it called?
How it appears radiographically?
What is it?
Reduced secretion of pituitary hormones
it’s a systemic endocrine disease
What is it called?
Dwarfism
How it appears radiographically?
▪ Finding of the jaws
o Normal eruption of primary dentition but delayed exfoliation
o Small jaws -> crowding and malocclusion because there is not enough space for the teeth to erupt
Which systemic disease manifest radiographically like this?

Renal
Osteodystrophy 1
Presentation is variable. Sometimes you see denser or granular
appearance of bone. You see increase here
but you sometimes will also see loss of definition of lamina dura, sometimes a sclerotic appearance
and trabeculation.
Which systemic disease manifest radiographically like this?

Renal
Osteodystrophy 2
sometimes you see:
- increase in bone density
- loss of definition of lamina
- dura and cortical bone
Osteoporosis
What is it?
Why it happens?
What the bone are like?
What is it?
▪ Generalized decrease in bone mass in which the histologic appearance of bone is normal, it is a metabolic bone diseases (MBD)
Why it happens?
- Aging process (postmenopausal women) bone mass usually increases until 30 years of age, and then there is a gradual decrease- about 8% loss in females and 3% loss in males
- Nutritional deficiencies
- Hormonal imbalance
- Inactivity
- Corticosteroid or heparin therapy
What the bone are like?
▪ More prone to fracture (distal radius, proximal femur, ribs, and vertebrae)
Which systemic disease manifests radiographically like this?

Hypophosphatasia
Which systemic disease manifests radiographically like this?

large root canal structures, large root chambers, premature loss of
teeth = hypophosphatasia.
Osteopetrosis
What is it?
How is the bone is like?
What are the effects on other structures?
What are the consquences?
What is it?
Defect in the differentiation and function of osteoclasts, (osteoclasts that are used to resorb bone in the bone modeling process. They are not functioning properly ►so we have an increase in bone density.) It is a metabolic bone diseases (MBD)
How is the bone like?
Bone is dense, fragile, and susceptible to fracture _and infection ►we now have a_n osseous structure but small bone marrow spaces
What are the effects on other structures?
It compromised vascular structures and cranial nerves
Which systemic disease manifests radiographically like this?

Hypophosphatemia
- Periapical lesions with radiolucency but no caries on the crown.
- There is loss of definition of cortical bone.
- On the teeth, you have:
- large pulp chambers
- hypoplasia of enamel and dentin
- periodontal and periapical lesions.
Osteopetrosis
What are the consquences?
- Compression of the cranial nerves as they pass through the narrowed skull foramina -> blindness, deafness, vestibular nerve dysfunction, and facial nerve paralysis.
- Compromises hematopoiesis Poor vascularity -> osteomyelitis
Which systemic disease manifests radiographically like this?

Progressive Systemic
Sclerosis
(scleroderma)
sharp areas of resorption in the bones near muscles attached to the
angle of the mandible= masseter and medial pterygoid. You see
resorption at the coronoid process at the attachment of the temporal
bone as well.
Which Systemic disease manifests radiographically like this?
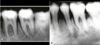
Progressive Systemic
Sclerosis
(scleroderma)
- presence of widening of the PDL space everywhere around the root of the tooth.
Rickets and
Osteomalacia
What are they
Differences
Effects on Bones
What happens?
They are metabolic bone diseases (MBD)
Inadequate serum and extracellular levels of calcium and phosphate, failure of normal activity of vitamin D.
There are different levels in the conversion from I,12- dihydroxy vitamin D that can have errors, not just
the consumption of vitamin D.
Differences
Rickets: disease affects the growing skeleton in infants and
children
Osteomalacia: disease affects the mature skeleton in adults
Effects on bones:
A softening and weakening of bones
Which systemic disease mainfest radiographically like this?
On a sickle cell anemia patient, you see:
- loss of this cortical bone area
- the hair-on-end appearance on the skull
Which systemic disease mainfest radiographically like this?

Sickel Cell Anemia
enlargement of bone marrow spaces, less trabeculation, more
osteoporotic bone. You see periapical pathology associated with teeth
with no obvious reason. You see the radioluscencies around the apex of
the mandibular teeth.
In Rickets and
Osteomalacia, there is Failure of normal activity of vitamin D, what causes it?
o Lack of vitamin D in the diet
o Gastrointestinal malabsorption problems
o Lack of exposure to UV light
o Liver disease
o Kidney disease
o Defect in the intestinal target cell response
Clinical presentation
Ricket
vs
Osteomalacia
Rickets
o Growth retardation
o Short stature
o Bowing of long bones of the legs, waddling gait
o Radiograph manifestations in the teeth (especially <3 years of age) and jaws
Osteomalacia
o Weak fragile bone structure
o Diffuse skeletal pain
o Susceptible to fracture with minor injury
o Radiographic manifestations in the jaws are uncommon
o you may see hyperplasia or thinning of mineralization of teeth. You can see hyperplasia of enamel in patients.
Which systemic disease mainfest radiographically like this?

Thalassemia
- osteopenic bone (loss bone mass and bones get weaker)
- radiolucent appearance of bone
- thinning of cortical bone around the mandible and maxilla.
- Usually there is hypoplasia of the paranasal sinuses.
Renal
Osteodystrophy
What is it?
what can it lead to?
What is it?
Chronic renal failure produces bone changes by interfering with the hydroxylation of vitamin D in the kidneys -> hypocalcemia -> inhibit the normal calcification of bone and teeth (it is a metabolic bone disease)
what can it lead to?
(secondary hyperparathyroidism)
level of calcium is low leads to having hyperparathyroidism secondary to osteodystrophy
Hypophosphatasia
What is it?
What are the types?
What is it?
- Rare metabolic bone disease due to lack of tissue-nonspecific alkaline phosphatase
What are its types?
Four types: prenatal, infantile, childhood, adult
- The younger the age of onset, the more severe the
- manifestations
- It may have premature loss of these patients because loss of function of the lungs in these patients
Hypophosphatasia
Common factors?
Dental manfestations?
Common factors?
- Low levels of tissue-nonspecific alkaline phosphatase
- High blood and urinary phosphoethanolamine
- Rickets-like skeletal malformations
Dental manfestations?
- Premature shedding of primary incisors
- Enamel hypoplasia
- Enlarged pulp chambers and root canals
Hypophosphatemia
What is it?
_Clinical Manifestations?
Dental Manifestations?_
What is it?
- A rare, heterogeneous group of inherited metabolic disorders characterized by decreased phosphate reabsorption in the distal renal tubules
Hypophosphatemia
Clinical Manifestations?
Dental Manifestations?
Clinical Manifestations
- Rickets-like skeletal malformations
Dental Manifestations
- Enlarged pulp chambers and root canals
- Periapical and periodontal abscesses of no obvious cause
- Enamel hypoplasia
Progressive Systemic
Sclerosis
(scleroderma)
What is it?
Demographics?
What is it?
- Excessive collagen deposition resulting in hardening (sclerosis) of the skin and other tissues can have involvement of GI tract, heart, kidney,etc
Demographics?
- Middle aged female
Progressive Systemic
Sclerosis
(scleroderma)
Clinical symptoms
Oral Manifestations
Clinical Presentation
- Thickened, leathery quality skin
- joint pain
- exaggerated response to cold (Raynaud’s disease)
- heartburn.
- more prone for heart problems and respiratory
insufficiencies,
Oral Manifestations
- microstomia (small mouth)
- Xerostomia (dry mouth)
- telangietasia (“spider veins”)
- Increased decayed, missing and filled teeth.
- higher Gingivitis scores (usually)
- Deeper Periodontal Pockets
Progressive Systemic
Sclerosis
(scleroderma)
Treatment
Treatment for generalized symptoms may involve:
- corticosteroids
- immunosuppressants, such as methotrexate or Cytoxan
- nonsteroidal anti-inflammatory drugs
Depending on your symptoms, treatment can also include:
- blood pressure medication
- medication to aid breathing
- physical therapy
- light therapy, such as ultraviolet A1 phototherapy
- nitroglycerin ointment to treat localized areas of tightening of the skin
(from google)
Sickle Cell Anemia
What is it?
What causes it?
What is it?
Chronic hemolytic blood disorder
What causes it?
▪ Abnormal hemoglobin, resulting in anemia -> by increasing the production of red blood cells -> requires compensatory hyperplasia of the bone marrow
Sickel Cell Aniema
Radiographics findings
- loss of this cortical bone area
- See the hair-on-end appearance on the skull
- enlargement of bone marrow spaces
- less trabeculation, more osteoporotic bone
- periapical pathology associated with teeth
with no obvious reason
Thalassemia
What is it?
What causes it?
What is it?
- Defect in hemoglobin synthesis
What causes it?
- RBC with reduced hemoglobin content and short life span
Thalassemia
Clinical and Radiographic findings
- Hyperplasia of the bone marrow component of the bone which results in fewer trabeculae per unit area and can change the overall shape of the bone
- Protrusive premaxilla
- Radiographic appearance very similar to Sickle Cell Anemia
Suspect systemic endocrine and metabolic disease if radiographs show what?
generalized decrease in bone density of jaws (thin cortices; granular cancellous bone; loss of lamina dura).
- Refer to physician for lab tests to make the diagnosis
We can include certain systemic endocrine and metabolic diseases as radiographic differentials in the presence of:
o Localized focus of radiolucency- think what?
o Mandibular prognathism and incisor flaring- think what?
o Premature shedding of primary incisors-think what?
o Enamel hypoplasia, enlarged pulp chambers and periapical abscesses of no obvious cause- think what?
o Localized focus of radiolucency► think brown tumor and
hyperparathyroidism
o Mandibular prognathism and incisor flaring► think acromegaly
o Premature shedding of primary incisors► think
hypophosphatasia
o Enamel hypoplasia, enlarged pulp chambers and periapical
abscesses of no obvious cause► think hypophosphatemia
What are the 3 types of Benign Fibro‐Osseous
Lesions?
- Fibrous Dysplasia
- Cemento-osseous Oysplasia
- Ossifying Fibroma
Fibrous Dysplasia
Cemento‐osseous Dysplasia
are both type of
Type of Bone Dysplasia
Ossifying Fibroma is a ———
Benign neoplasm
What are the types of Fibrous Dysplasia?
Monostotic
Polystotic
McCune‐Albright Syndrome
Craniofacial
Mazabraud Syndrome
What is the most common type of Fibrous dysplasia?
Monostotic
What is Monostotic Fibrous dysplasia?
a Fibrous dysplasia involving one bone
o Ex: when only the mandible involved or only the maxillae
(Most common type (70%)
What is Polystotic Fibrous dysplasia?
a Fibrous dysplasia involving more than one bone
What is the Second most common type of Fibrous dysplasia?
Polystotic Fibrous dysplasia
What are the two types of Polystotic Fibrous dysplasia?
Jaffe Type
McCune‐Albright Syndrome (involving multiple bones with
endocrine abnormalities)
What is Craniofacial Fibrous dysplasia?
-a Fibrous dysplasia limited to Skull and Facial Bones...
What is Mazabraud Syndrome
-Fibrous dysplasia with intramuscular myxomas
What happens in Fibrous Dysplasia?
an aberrations in osteoblastic/osteoclastic function ► normal bone turn over affected ► normal bone structure will be affected!
What is
fibrous dysplasia ?
Developmental lesion characterized by substitution of normal bone by poorly organized woven bone and fibrous tissue.
What is the etiology of fibrous dysplasia?
GNAS1 gene mutation in fibrous dysplasia is a potential diagnostic adjuvant, as it is not
found in normal bone tissue (etiolog
What gender and age affected by Fibrous Dysplasia?
- No gender predilection
- commonly seen in pediatric patients and young adults
What are the clinical charcterstics of fibrous dysplasia?
- Clinically, it causes bone expansion and asymmetry
- most typical presentation of monostotic fibrous dysplasia is a slow growing painless enlargement in the affected area.
- so the patient may notice a slight asymmetry that won’t bother them intially, but over time~months to years ►they’ll notice that this area is slowly and steadily growing more and more ( slow and painless)
What are the most common sites of Fibrous Dysplasia?
• Most common sites of FD include the ribs, femur, tibia, maxillae and mandible
the Maxillae is affected more than the mandible
What is this disease?
Patient CC: painless mass that is growing on one side

FD
Radiographically: you have altered trabecular pattern
Clinically: Painless mass slowly growing over time
is is typical
presntation of Fibrous Dysplasia
What is this disease?

Fibrous Dysplasia
- ill‐defined radiolucent/radiopaque/mixed radiolucent‐radiopaque entities that blend with normal bone.
- The left side is affected. Left body of the mandible and the ramus.
- The cortical outlines have been expanded near the inferior border of the mandible.
What is the radiographic features of Fibrous dysplasia (FD)

• Maxillae affected more than mandible
• Ill‐defined borders, blends in with the surrounding bone (not necessary to be corticated)
• Variable density and orientation of the trabecular pattern (radiolucent, radiopaque or a combination)
- *• Ground‐glass appearance** (common)
- *• Peau d’orange (surface of an orange)** (common)
- *• Cotton wool appearance** (common)
- *• Fingerprint pattern** ( uncommon pattern)
• Typically the lesionss in the maxillae are more homogenous and radiopaque, whereas they may appear more heterogenous and mixed in the mandible.
*typically you’ll see the ground glass appearnce and Peau d’orange on the maxilla as they are homogenous the cotton wool appearance more commonly found in the mandible since it is heterogenous.
What is this trabecular pattern of the FD?

Fingerprint pattern
The arrow indicating the inter‐radicular area of this molar. You can see the trabecular
bone has been altered into a fingerprint pattern.
This is a case of localized fibrous dysplasia.
Very uncommon.
What is this trabecular pattern of the FD?

Cotton wool
appearance
Irregullary shaped and outlined radiopacities blending in with adjacent bone
What is this trabecular pattern of the FD?

Peau d’orange
surface of an orange – the bone shows a “pitting” appearance.
What is this trabecular pattern of the FD?

Ground Glass Pattern
it appears granular in nature. (Grainy)
What is this Radigraphical finding?

Fibrous dysplasia on
the right mandible.
Note the superior displacement of the IAN Canal
This is not odontogenic ( as they are usually above the canal)
Anything below th canal ►think of it as originiating from the bone itself
What is this Radigraphical finding?

Fibrous Dysplasia in
the left of the
maxillae.
Always compare both side left and right
- We see granular/glass appearance of the bone ( blue arrow) and compare it to the contralateral maxillae. The trabucular pattern has changed signficantly.
- Also compare the maxillary sinus space. The left maxillary sinus appears radiopaque.
- That is because the maxillae has been enlarged to the point where it is pushing the floor of the maxillary sinus superiorly and reducing the total volume of the sinus.
- The purple arrows indcate the displaced floor of the maxillary sinus.
what is this radiographic finding?

FD
Note the normal left maxillary sinus and the obliterated space of the right maxillary sinus ( blue arrows).
A ground glass appearing entity (humogenous radiopaque lesion) has obliterated the space secondary to expansion of the right maxilla.
These findings are consistent and quiet common in advanced cases Firbous dysplasia
How does Fibrous dysplasia affects the
Surrounding structures?
- May have no effect ( especially if it hasn’t reached the cortical outlines)
- Expansion and thinning of cortical walls
- Displacement of teeth ( espically in advanced cases)
- One of the few entities that cause SUPERIOR displacement of the mandibular canal
What is this radiologic finding

Periapical COD
green arrow
Simple bone cysts may develop in regions of COD ( periapical or florid type)
So look for areas void of trabucular bone and has scalopping of the lesion.
red arrow
What is this radiologic finding

mature Periapical COD
Coronal cross section of the posterior mandible in the region of the premolar
~ mixed radiolucent/radiopaque entity, the center is radiopaque and the periphery is
radiolucent.
What is this radiologic finding

mature Periapical COD
You can have these lesions in endentulous areas as well.
So this is is an endeulous area, but if there was a tooth here, this would be in the
periapicel region or near it with mixed radiolucent/radiopaque entity the differential
diagonsis of this area could include Periapical COD.
What is this radiologic finding?

mature Periapical COD
You see a nice radiolucent rim and radiopaque center
so mixed radiolucent/radiopaque
entity in the periapical region of tooth #31
most likely diagonsis would be Periapical
COD.
What is this radiologic finding

A very mature Periapical COD
( purple arrow)
Well‐defined radiopacity in the periapical region.
Sometimes you may or may not be able to differentiate a very thin radiolucent line as in
this case.
you might include ddx of other lesions which might present with
radiopacity in the preapical region
There are certain tests you can do clinically to differentiate too.
or do clinical tests
What is this radiologic finding

Periapical COD
Sagital cross section of the anterior Mandible.
Mixed radiolucent/radiopaque area (green circle)
What is this radiologic finding

Early & mature Periapical COD
Preapical radiographs of the anterior mandible of the same patient at different times.
Note the differnece in density between the two radiolecency:
Note the internal structure of the radiopacity is quite radiolucent ( purple arrow)
The Preapical radiographs of the same region taken at a later time shows a more
radiopaque internal structure (pink arrow). This reflect the maturing of the COD lesion.
The lesion with Pink arrow can be described as well‐defined mixed
radiolucent/radiopaque entity. ( because you have radioleucent part and radipaque part)
What is this radiologic finding

Early Periapical COD
well defined radiolucency surrounding the apeces of these two central
When looking at such cases, it is also imporant to:
1. look at the crowns to look for carious lesions. If there is no restorations or no
evidence of caries, it is likely that these lesions are arising from the bone and not
secondary to pulpal involvement.
2. It also important to look at the PDL and Lamina dura, typically in COD lesions they
should be visisulized and intact ( but because this is a 2D image and this area may
superimpose on this region and obsecure the visulizing of the lamina dura and the
PDL)
what’s the difference between COD and Inflammatory lesion?
COD won’t have effect on the PDL space itself, because it orginates from the bone!
Vitality testing can help us differntiate between inflmmatory lesion and something that happeing inside of the bone.
What is this radiologic finding

Florid COD
Axial section of the mandible.
- Notice mixed radiolucent/radiopaque entity on the patient right side. And on the left the area is more radiopaque centrally and has a thin radioluceny around it.
- The arrows indicate well‐defined radiopacities immedietly surrounded by radiolucent rims.
- Note that the radiolucent rim on the left side is thin when compared to the lesion on the right. This likely means that the lesion on the left is more mature ( more time has passed for the entity to produce more woven bone).
What is this radiologic finding

Florid COD
Two periapical radiographs of the left and right posterior mandible of the same patient.
In this case, note the areas of radiolucency and radiopacity are rather ill defined but widepsread to affect most of the teeth.
Most of the teeth noted here are restored.
So even if the radiographs suggest a cemento‐osseous process, it is important to keep an eye for these teeth in term of vitality and prevent a periapical infections which would otherwise secondarily infect the altered bone of COD.
What is this radiologic finding

Florid COD
Multiple regions of COD.
Notice the wide areas of scelortic/radiopaque areas on mandible and also on maxillae
What is Differential Diagonsis
for Firbous Dysplasia
(FB)
?
Generalized FD
- Metabolic bone diseases (hyperparathyroidism) (any disease that incrase trabacular bone density)
- Paget’s disease
Localized FD
- Osteomyelitis
- Osteosarcoma
What is the management of Fibrous Displysia?
- Consultation with an OMFR is advisable. Monitoring of the area is also advised.
- Typically treatment is not needed unless there are clinical symptoms or patients present with cosmetic concerns if clinical symptoms are severe
- Implants and surgical intervention should be avoided when possible as these areas are void of blood supply
Cemento‐ossifying
Fibroma
Types
and
Location

There are two types: classic and juvenile form
-juvenile seen in younger patients and
tend to be more aggressive in nature ( both radiographically and clinically aggressive features)
• Young adults and females affected mostly
• Bony expansion and displacement of teeth can be seen in many cases ( not suprising
since it acts like a neoplasm)
• More commonly seen in the mandible and in posterior regions
what is this radiographic finding?

Cemento‐ossifying
Fibroma
Note the internal granular appearance of the trabucular bone ( black arrows)
The purple arrows shows the wall of the expanded buccal/facial and lingual cortical plates caused by the neoplastic entity.
This was a confirmed cased of ossifying fibroma* mainly because of two things:
1. siginficant cortical expansion on buccal and lignual side
2. altered trabacular pattern.
ddx of fibrous dysplasia but you should look for a radiolucent rim
if you can and if not, they maybe considered under the same differential diagosnsis.
Note that may help you in differentiating :
The maxilla is affected more in Fibrous dysplasia
The mandible is affected more in Ossifying fibroma
What is this radiographic finding?

Cemento‐ossifying
Fibroma
Axial section of the
mandible
- The granular radiopacity immediately surrounded by a radiolucent rim ( purple arrow)
- Also note the extent of the expansion of the buccal and lingual cortical plates, a feature which is common of ossifying fibroma.
- This is more clear radiographically where we see a radiolucent rim surrouding a mixed radiolucent/radiopaque center and there is a siginficant expansion of the buccal and lingual plates. ► very common in ossifying fibroma
Cemento‐ossifying
Fibroma
is classifed as ———–
and why?

Classified as a benign neoplasm
Because it acts like a benign neoplasm.
Once you examine it under microscope, you’ll see features resmeble benign fibrous osseous lesions. You’ll see:
Fibrous connective tissues
cementum like material
even altered bone material (woven bone)
Cemento‐ossifying
Fibroma
Radiographic features

- Well‐defined, round or oval lesion
- Periphery of the lesion is corticated and may exhibit a radiolucent periphery (sometimes referred to as a soft tissue capsule)
- Internally, the lesion is typically granular or radiopaque but may show variations (mixed radiolucent/radiopaque)
- Strong tendency to displace teeth and cortical outlines
what is this radiographic finding?

Cropped Panaromic showing
a case of
Cemento‐ossifying
Fibroma
- Appreciate the radiolucent rim indicated by the black arrows.
- Also note the internal structure of the trabucular bone and compare it to adjacent unaffected areas. It is more granular and radopaque compared to adjacent areas.
- Another important feature to appreciate is the displacement of the anterior teeth (diverging roots)
- These features are usually seen in lesions with benign neoplastic characterstics.
What is CEMENTO‐OSSEOUS
DYSPLASlA (COD)?
Dysplastic lesions that are confined to the jaws.
What is this disease?

Cleido-Cranial
Dysplasia
Treatment: For children, facial reconstructive surgery on the bones of the face to reshape the forehead or cheekbones. Spinal fusion procedures to support the spinal column. Lower leg surgery to correct knock knees (knees that bend inward toward the center of the body)

What is this disease?

Gardner’s Syndrome
Synonym: Familial Multiple Polyposis.
Remember this:
GarDENse Bone Island.
GARDEN-FOREST:
F- Familial adenomatous polyposis.
O- Osteomas.
RE- Retinal epithelial hypertropy.
ST- Supernumerary teeth.
Treatment:
Because people with Gardner’s syndrome have a higher risk of developing colon cancer, treatment is usually aimed at preventing this.
Medications such as an NSAID (sulindac) or a COX2 inhibitor (celecoxib) may be used to help limit the growth of colon polyps.
Treatment also involves close monitoring of the polyps with lower GI tract endoscopy to make sure they do not become malignant (cancerous). Once 20 or more polyps and/or multiple higher risk polyps are found, removal of the colon is recommended in order to prevent colon cancer.
If dental abnormalities are present, treatment may be recommended to correct problems.

What is this disease?

Osteopetrosis
Osteomyelitis is a complication in patients with osteopetrosis as can be seen in pan image!
Treatment: Bone marrow transplant (to stimulate osteoclast formation).

What is this disease?

Paget’s disease stages
Early Linear lines: The bone is being resorbed in a very distinct
pattern > linear patterns of trabeculation
Middle -MAY see the “cotton wool” appearance (but this is more
pronounced in the third stage)
-the trabecular pattern may or may not be slightly affected
Late - There is MORE bone deposition -the “cotton wool” appearance
is very very clear in this stage! Also-hypercementosis and spacing of teeth.
What is this disease?

Paget’s Disease
Also Known As: Osteitis Deformans.
Skeletal disorder involving osteoclasts
Treatment: Osteoporosis drugs (bisphosphonates) are the most common treatment for Paget’s disease of bone

What is this disease?

Cherubism
Treatment: Usually not needed as the cyst-like lesions fill in with granular bone during adolescence- conservative surgical procedures may follow for cosmetic reasons.

What is this radiographic finding??

Idiopathic
Osteosclerosis
AKA: Dense Bone Island
Not associated with any dysplastic, neoplastic, inflammatory or systemic disorder.
Common incidental finding.
Slow growing, typically stops growing by the time of skeletal maturity.
Peak prevalence in the third decade of life.
No treatment required; monitoring is suggested.

Idiopathic
Osteosclerosis
vs

PCOD

Differentiating factor: Radiolucent zone surrounding the radiopacities of COD lesions. No such radiolucent areas for idiopathic osteosclerosis.
Important: The root of the tooth #28 appears to be resorbed but is likely not.
Look at the root of #29. These teeth are still undergoing development in a young patient.
Left is showing dense bone island.
Right is showing Periapical COD- this is intermediate stage, not fully mature. You should see a radiolucent rim.
Another more obvious radiographic feature: you see radiolucent areas surrounding in both images, the common feature is: because PCOD and dense bone island do not affect the PDL spaces – you should be able to see the PDL spaces.
Sometimes it’s not the case. Look for the PDL, look for radiolucent area surrounding possible central radiopacity, idiopathic osteosclerosis can cause resorption; PCOD hasn’t been associated with root resorption.
Idiopathic
Osteosclerosis
vs

Hypercementosis

Differentiating Factor: A well-defined radiolucent border that is continuous with the PDL of the tooth, in the case of hypercementosis. This means that whatever is happening is within the confines of the tooth-bearing region. In this case, the
cementum.
Hypercementosis- Cementum is overraeacting, so there’s enlargement of cementum.
If cementum is larger, it should be pushing the PDL out (black arrow). So the PDL is enlarged meaning you should be able to see a radiolucent rim around the area. And the radiolucent rim should be continuous with the PDL of the
remaining root structure.
Idiopathic
Osteosclerosis
vs

Cementoblastoma

Differentiating Factor: A well-defined radiolucent border that is continuous with the PDL of the tooth, similarly seen in the previous case of hypercementosis.
(sometimes it is difficult to differentiate hypercementosis and cementoblastoma, in this case, the beige arrow indicates the resorbed root surface, which normally occurs in benign neoplastic cases, such as cementoblastoma.
Cementoblastoma is more of a heterogenous radiopacity- meaning you may see
gaps, like radiolucent voids, in between the areas.
See radiolucent rim.
But more common feature include root resorption because it’s a neoplastic condition. It should act like a neoplasms in which it’s destroying some of the root structure.
Idiopathic
Osteosclerosis
vs

For condensing osteitis, look for heavily restored or carious teeth. Condensing osteitis typically surrounds the initial rarefying osteitis lesion. The teeth in these cases are non-vital as they represent a condition that is secondary to pulpal necrosis.
Open necrosis, eventual PDL space widening and then once the infection reaches the bone, you have bone loss.
Now you have an overreaction or inflammatory reaction surrounding the initial inflammation.

What is this disease?

Focal Osteoporotic
Marrow Defect
A large marrow defect that may mimic a
cystic/neoplastic radiolucency in the jaw.
common incidental finding
a variation of normal anatomy within trabecular bone.

What is this disease?

Simple Bone Cyst
Also known as
1.) Solitary Bone Cyst.
2.) Traumatic Bone Cyst.
3.) Idiopathic Bone Cyst.
4.) Hemorhhagic Bone Cyst.
Remember radiographic feature
tend to Scalop between teeth
Treatment includes surgical curettage- spontaneous healing has been reported.

What are these two disease?

Sometimes, simple bone cysts should be differentiated from odontogenic keratocysts (OKCs)

CGCG should be differentiated from ————-

brown tumor.

What is this disease?

central giant cell granuloma
CGCG

What is this disease?

Aneurysmal Bone Cyst

What is this radiographical presentation?

Mucositis
Thickening of the mucous of the sinus
- normally we don’t see mucosa
because it is very thin membrane
10 to 15 times thicker.
Most common
incidental findings
that we can see on
radiographs
What is this radiographical presentation?

Sinusitis
Sinus mucosa becomes inflamed and thickened from infection or
allergen, which may lead to ciliary dysfunction, retention of sinus
secretions and blockage of sinus drainage
● 10% of maxillary sinusitis are related to dental infections
What is this radiographical presentation?

Sinusitis
In this cone beam CT scan, we can see opacification of the sinus +
sometimes we see gaseous bubbles. It is fluid that is forming inside the
sinus.
What is this radiographical presentation?

Sinusitis
Sinusitis can be secondary to oral antral communication (communication
between maxillary sinus and oral cavity)
this can happen due to
extraction
What is this radiographical presentation?

Antral Pseudocyst (Retention Pseudocyst)
Localized, submucosal accumulation of fluid forming a sessile, domeshaped
swelling along a sinus border
● Common incidental radiographic finding on panoramic
● Well-defined, non-corticated and dome shape radiopacity mostly along
the floor of maxillary sinus
What is this radiographical presentation?

Antral Pseudocyst (Retention Pseudocyst)
What is this radiographical presentation?

Antral Pseudocyst (Retention Pseudocyst)
What is this radiographical presentation?

Antrolith
Deposition of mineral salts (calcium phosphate/carbonate/magnesium) around an exogenous or endogenous (due to blood, pus or mucous) nidus
● Pediatric and adult population
‐ Small antroliths – incidental radiographic finding
‐ Large antroliths – sinus obstruction, sinusitis, nasal discharge,
pain
● Mostly adjacent to the floor of the maxillary sinus
● We see combination of radiopacity and radiolucency due to layers
of calcification.
Radicular Cyst VS
Antral Pseudocyst

One of the ways to differentiate antral pseudocyst from radicular cyst is by the presence of cortication.
‐ Reticulosis is a cystic lesion that happens around the apex of the nonvital
tooth.
‐ They have a round and domed shaped appearance too, but they are from
a different origin happening inside the alveolar processes
What is this radiographical presentation?

Antrolith
Deposition of mineral salts (calcium phosphate/carbonate/magnesium) around an exogenous or endogenous (due to blood, pus or mucous) nidus
We see a presence of radiopacity which is antrolith inside the
maxillary sinus
What is this radiographical finding?

Foreign Body in
Maxillary Sinus
What is this radiographical finding?

Foreign Body in
Maxillary Sinus
What is this radiographical finding?

Periostitis
•Lamellar, periosteal reaction from periapical inflammatory disease
•Exudate from infected tooth diffuses through the cortical bone,
(elevation of periosteum) lifts and stimulates the periosteal lining to
produce layer(s) of new bone
•Floor of maxillary sinus
•Inferior, buccal, lingual mandibular cortices
COD can be divided in to:
1) Periapical COD
2) Focal COD ( not covered)
3) Florid COD
Two types of COD
instead of three
Perapical COD
&
Florid COD
Cemento‐Osseous Dysplasia is Similar to Fibrous dysplasia where
cancellous bone is
replaced with fibrous tissues & cementum‐like material.
CEMENTO‐OSSEOUS
DYSPLASlA
COD
is it symptomatic?
is there bony expansion?
- Typically asymptomatic, almost always captured as incidental finding
- Generally, no bony expansion but is not uncommon in the florid type
Cemento‐osseous dysplasia COD
Gender?
Age?
Ethincity?
• Commonly seen in middle‐aged patients
female predilection
- more commonly seen in the Black population
- also frequently seen in Asian population
What are the Radiographic
features of Cemento‐osseous dysplasia COD?
- Usually well‐defined borders in perapical type (may be ill‐defined in florid type).
- Early lesions show radiolucent features in the periapical area of the teeth
_As times progresses, the lesion matures =_the entity may become radiopaque.
‐ as a result there is also an intermideate mixed phase
• The lesions mature from the center outwards
‐ as a result, a radiolucent rim surrounding the lesion is commonly noted.
• Typically the periodontal ligament space of affected areas are intact but my not be visualized because they are superimposed over the region.
What is Florid COD?
Widespread form of periapical COD
There is some discreppency on how to consider a lesion a florid COD
Some people say the radiopacity entities have to be on at least 2 qudarants And other says if you have the radiopacity entities crossing the midline of the bone.
If it is in 3 quadrant ► then you can defentitly say it’s the Florid type, but even if you see itone bone and it has crossed the midline ► you may consider it Florid COD
What is differential diagnosis for Periapical COD?
PCOD
Florid COD
Rarefying osteitis (radiolucent lesions) ( it would differentiate in the more early stages of the COD ( the radiolucent stage)
Condensing osteitis (considered in the differential when the lesion is more mature and more radiopaque lesions)
Cementoblastoma ( benign neoplasm of the cementum so we
should be able to see certain features that reflect benign neoplastic lesions )
Dense bone islands ( a common differential when considering COD)
What is differential diagnosis for florid COD?
FCOD
- Paget’s disease ( t generalized areas)
- Osteomyelitis ( localized area because we have mixed radioluecent/radiopaque areas)
What is the Management of COD?
- Typically, no treatment is required unless these regions show clinical/radiographic evidence of secondary infection
- Ex if patient complain of some pain of that area –> we
want to follow up that region - Surgery within the dense bone has a high risk of causing osteomyelitis
-
Patients should be seen regularlyfor preventive treatment
Want tooth supported rather than tissue supported RPD and CD
Treatment of
Cemento‐ossifying
Fibroma
- Surgical excision ( need to send to biopsy in order to confirm the diagosnsis of that)
- Wider resection with bone maybe necessary in soma larger or more clincally aggressive cases.
