Follow-up: Device assessment Flashcards
Hones pattern recognition of IEGMs for various complications and arrhythmias commonly encountered in-clinic and discusses appropriate resolution. Currently weighted 10% in the CCDS exam.
True / False
Hyperkalemia typically causes loss of atrial capture before loss ventricular capture.
True.
If atrial loss of capture has occurred due to significantly increased thresholds, suspect hyperkalemia.
If a patient presents with an unusually wide QRS, what metabolic state should you consider?
Hyperkalemia.
True / False
Hyperkalemia decreases stimulation threshold.
False - Hyperkalemia increases stimulation threshold.
When looking at the pacing state histogram.
If total % of Ap state (shown as ApVp + ApVs) is greater than all other states, what can be inferred?
A large amount of pacing is likely at the base rate. Suggestive of SSS or Atrial incompetence.
When looking at pacing state histogram.
If total % of As state (shown as AsVp + AsVs) is greater than all other states, what can be inferred?
- If AsVp is large then the condition is likely CHB or the AVD is programmed too short.
- If AsVs is large then Sinus Rhythm is prevalent and pacemaker is on standby most of the time.
When looking at pacing state histogram.
If total % of Vp state (shown as AsVp + ApVp) is greater than all other states, what can be inferred?
Condition is likely CHB or AVD is programmed too short.
When looking at pacing state histogram.
If total % of Vs state (shown as AsVs + ApVs) is greater than all other states, what can be inferred.
AV conduction is present in this patient.
True / False
A normal P-wave amplitude histogram follows a bell shaped curve distribution.
True.
When viewing a P-wave amplitude histogram, there a two distinct groupings. One grouping is larger in amplitude, while another is smaller in amplitude. There is a void of data in-between the two groupings, what is most likely?
- Signals recorded in the larger amplitude group are likely sinus beats
- Signals recorded in the smaller amplitude group are likely some form of atrial tachycardia
CRT pacing shows dominant RV pacing on an ECG. The patient has CHB, RV and LV thresholds are appropriate and V-V delay is 0ms. What could be occurring at the LV site?
LV exit block or LV conduction delay due to substrate in vicinity of LV electrode.
Describe the rhythm on the IEGM.

Atrial Fibrillation with rapid ventricular response.
R-R variability is distinctive of AF. It is impossible to know 100% however as this is a single chamber device. A dual chamber device would allow true discrimination by visualising atrial activity.
Describe the rhythm on the IEGM.

Atrial tachycardia with 1:1 conduction.
Describe the rhythm on the IEGM.

2:1 AV Block
Describe the rhythm on the IEGM.

Atrial Tachycardia.
Does this patient likely have CHB or not?

Patient likely has CHB.
Note how there is no conduction of P-waves and Vp throughout the strip. This remains true even when an atrial tachycardia starts.
Is this a short duration A-Tach or A-Fib episode?

Short duration A-Tach.
Note how R-R interval is regular. The rate is also too slow to be AF.
Describe the rhythm on the IEGM.

Sinus Rhythm.
There is atrial lead noise respondent to lead damage. Unlikely to be EMI interferrence as this would display on both leads.
You ask a patient to perform provocation manouvers in clinic and witness this. Both leads are programmed Bipolar. Describe what is happening.

Atrial lead noise likely respondent to lead insulation failure.
Source of noise is likely myopotentials. Unipolar sensing would also give rise to myopotential.
Is the device detecting this bipolar lead noise? How best to program around it?

- The atrial lead noise is being detected by the device. This would inhibt output, which could be catastrophic if this was the ventricular lead in a CHB patient.
- Try programming the lead to the unipolar. Retest provocation manouvers in clinic.
- Ultimately a lead revision is necessary.
Which conductor has likely failed in the following biploar leads?

Atrial ring conductor has likely failed.
Rarer for the tip conductor to fracture first. This can be tested by programming the lead unipolar tip to can and asessing the IEGM.
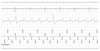
What is the atrial threshold?

Atrial threshold is 1.5V.
Note how a P-wave is evident on the ECG immediately following the 1.5V stimulus but not evident immediately following the 1.4V stimulus. Note also that an intrinsic P-wave breaks through following the 1.4V stimulus, also indicating non capture.
A reversion to 2.4V inbetween is characteristic of Biotronik threshold testing and should be ignored for the purpose of threshold determination.
Describe the rhythm on the IEGM.

Atrial Flutter with variable conduction.
Rhythm is too regular to be AF.
Describe the rhythm on the IEGM.

Flutter with 2:1 conduction.
What can be said about this rate trend?

Highlights some form of sustained atrial arrhythmia at varying rates.
Patient also likely has CHB as there is little ventricular rate deviation during Tach/Sinus.