Bowel Conditions Flashcards
What is intestinal failure?
Inability to maintain adequate nutrition or fluid status via the intestines.
What causes intestinal failure?
Obstruction, dysmotility, surgical resection, congenital defect, or disease associated loss of absorption
Of the 3 types of intestinal failure, which are acute and which are chronic?
Type I & II IF are acute. Type III IF is chronic
Describe Type 1 IF
Self limiting short term postoperative or paralytic ileus
Describe Type II IF
Prolonged, associated with sepsis and metabolic complications. Often related to abdomen surgery with complications
Describe Type III IF
Long term but stable - home parenteral nutrition often indicated. e.g. short gut syndrome
What is the management of Type I IF?
- Replace fluids/electrolyes through IVs
- Parenteral nutrition if can’t tolerate food/fluids > 7 days post op
- Acid suppression (PPIs)
- Octreotide (minimises movement and secretion of gut)
What is parenteral nutrition?
Also known as intravenous feeding, is a method of getting nutrition into the body through the veins
What are the main complications of parenteral feeding?
Pneumothorax, arterial puncture, misplacement, sepsis
What are some of the causes of Type II IF?
• Surgical complications • Coeliac disease • Vascular ischaemia • Crohn’s • Malignancy • Radiation
What is the management for Type III IF?
- Home parenteral nutrition - Intestinal transplantation Newer methods: - GLP2 treatment for short bowel syndrome - Bowel lengthening (regrowing lost bowel)
What is the length criteria for short bowel syndrome?
250-850cm
What is the 5 year survival for HPN vs intestinal transplant?
HPN: 70% 5year survival Intestinal Transplant: 50-60% 5y survival (eating but also requires stoma)
What is the main priority with IF?
Look for and address malnutrition
Where does the vasculature supply for small bowel come through?
The mesentery
What are the histological characteristic of small intestine?
Villi (which are lined by enterocytes and goblet cells full of mucin). Enterocytes are lined with brush border with microvilli
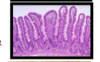
What does the jejunum have that the ileum doesnt?
Jejunum has a ‘stack of coins’ appearance because of plicae circularis (mucosal folds) while ileum is ‘characterless’, and appears a cylindrical tube
What are the 2 main mechanisms behind ischeamia of the small bowel and give examples of each
1) Mesenteric arterial occlusion (e.g. atherosclerosis of SMA or thromoelbolism from AF) 2) Non occlusive perfusion insufficiency (e.g. shock, strangulation obstructing venous return, drugs, hypervoscity)
What is the classification of small bowel ischaemia based on?
Degree of infarction caused i.e. mucosal to transmural

What is Meckel’s Diverticulum?
Result of incomplete regression of vitello-intestinal duct where used to get nutrients from the yolk sac (outppuch structure of the small bowel)
Why is Meckel’s a disease of 2s?
-Pts present around the age of 2 - It is 2 inches long - 2 feet above the IC valve - Affects 2% if the population
Which condition can Meckel’s mimic if it become diverticulitis?
Appendicitis
True or False: Primary tumours of the small bowel are more common than secondary tumours
False, secondary tumours are much more common, such as from ovary, colon and stomach
What are the 3 main primary tumours of the small bowel?
1) Lymphomas (mostly Maltomas) 2) Carcinoid tumours 3) Carcinomas
What is the commonest site for carcinoid tumours of the small bowel?
Appendix
What is carcinoid syndrome and when does it often occur?
Often occurs when carcinoid tumours spread to the liver and hormones such as serotonin are released into the bloodstream, and involves a collection of symptoms: -diarrhoea, abd. pain and loss of appetite - flushing of the skin, particularly the face - fast HR - SOB and wheezing
What are carcinoid tumours?
Tumours of the endocrine system
Which disease are associated with carcinoma of the small bowel?
Crohn’s and coeliac
What are the histological characteristics of carcinoid tumours?
They produce these islands of cells which are homogenous/monotonous throughout

What is the commonest cause of an acute abdomen?
Appendicitis
What are the signs and symptoms of appendicitis?
Vomiting, abdominal pain, RIF tenderness and increased WCC
What are the main causes of appendicitis?
- Unknown - Faecoliths (dehydration) • Impacted faeces - Lymphoid hyperplasia - Parasites - Tumours (rare)
What are the histological findings of appendicitis?
Muscosal ulceration and mural inflammation, and pus/neutrophils in lumen

What are the complications of appendicitis?
- Peritonitis - Rupture - Abscess - Fistula - Sepsis
What is the underlying pathophysiology of Coeliac Disease?
An abnormal reaction to gliadin, a constituent of wheat flour, gluten, which damages enterocytes and reduces absorptive capacity (essentially an auto-immune disease)
What is coeliac disease strongly associated with?
- HLA-B8 haplotype (gene thingy) - Dermatitis herpetiformis - Strong association with childhood diabetes
What happens to gliadin, the toxic gluten component, in Coeliac disease?
Gliadan, instead of being broken down as normal, start an auto-immune inflammatory response
Which cells mediated the inflammatory response in Coeliac disease?
T-cell lymphocytes which exist within the small intestinal epithelium ‘intraepithelial lymphocytes’ (IELS)
What is seen histologically in Coeliac disease?
- There is increasing loss of enterocytes leading to loss of villous structure, loss of surface area, a reduction in absorbtion and a flat duodenal mucosa - No villi, only crypts as it is all flat - On surface can also see lots of lymphocytes and inflammation in lamina propria - Stem cells cant keep up with the regeneration so becomes flat - Also massive infiltrate of toxic t cells

What is the most sensitive test for coeliac disease and what are the positive findings?
Serology: Antibodies anti-TTG, anti-endomesial, anti-gliadin
What are the symptoms of malabsorption?
• Loss of weight • Anaemia (Fe, Vit B12, Folate) • Abdominal bloating • Failure to thrive • Vitamin deficiencies
What are the complications of Coeliac disease?
- Malabsorption
- T-cell lymphomas of GI tract
- Occurs because the t cells have become autonomous and have the inflammatory effect even without the gluten trigger
- Increased risk of small bowel carcinoma
- Gall stones
- Ulcerative-jejenoilleitis
What does the clinical features of small bowel obstruction depend on and what are they?
Depends on the level obstruction Proximal: vomiting, no distension Dista: late vomiting, gross distension
What are the 2 main types of small bowel obstruction?
• Mechanical • Adynamic (ileus) (Essentially stops functioning)
What are the mechanical causes of small bowel obstruction divided into?
- Intraluminal (in lumen) (e.g. Tumour, Gall stone ileus)
- Intramural (in wall) (e.g.Crohn’s)
- Extrinsic compression (e.g. Adhesions, Hernia, Volvulus)
What are the overall causes of any bowel obstruction
B - bolus
A - adhesions (congenital or surgical)
T - tumour
H - hernia
V - volvulus
I - ileus/inflammatory/intussusception
P - pseudo-obstruction
S - strictures
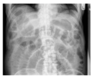
What are the main investigations for diagnosis small bowel obstruction?
- AXR (erect if possible) -CT
What is the management of small bowel obstruction?
Generally conservative without surgery:
- Fluid resuscitation potassium as fluid is pooling in bowel and usually hypokalaemic
- Analgesia
- Catheterise
- NG tube (to decompress stomach)
- Antithrombolitics (high risk of DVT)
- Operate if there is a risk of hernia, cancer or strangulation
What is the cause of mesenteric ischaemia?
Embolus or thrombosis (arterial and venous)
What condition is ‘angina of the gut’ referring to?
Chronic mesenteric ischaemia - often due to atherosclerosis in the SMA
What us the investigation of choice for mesenteric ischaemia?
CT
As well as pancreatitis, which condition can cause a raised amylase?
Small bowel ischaemia
Is Meckel’s diverticulum a true or a false diverticulum?
True
What is the clinical presentation of Meckel’s?
Often asymptomatic In children it may cause: - Rectal bleeding, obstruction and perforation
What is the road bump sign?
When you ask what brough them in or if anything bothered them on the way in, they will often say the road bumps
What are the clinical features of appendicitis both initially and progressively?
Initial visceral: - Nausea - Anorexia - Central abdominal pain Progressive parietal: - Right iliac fossa pain - Puritanism
What is the main investigation for carcinoid tumour of the appendix?
Chromafrannin A staining
What is diverticular disease?
Protrusion of a cavity through its contents, such as like a hernia
What is the difference between a true and false diverticulum?
- True diverticulum – all the layers - False diverticulum – just the mucosa comes through
What would you use to diagnose diverticular disease?
- Barium enema -Colonoscopy/sigmoidoscopy
What are the clinical features of diverticulitis?
• LIF pain/tendernss • Altered bowel habit • Septic (palpitations, fever, lethargy, anorexia)
What are the complications of diverticulitis?
• Pericolic abscess – infection gets walled off • True perforation • Lumen haemorrhage • Stricture • Fistula
How would you class acute diverticulitis?
Hinchey classification
How would you treat uncomplicated diverticulitis?
Oral antibiotics (if anything)
How would you treat complicated diverticulitis?
- Hartmen’s procedure (Remove the sigmoid colon and leave with an end colostomy )
- Primary resection/anastomosis
- Percutaneous drainage
- Laparoscopic lavage and drainage
What are the causes of colitis?
- IBD (Crohn’s disease and ulcerative colitis)
- Bacterial infections (campalo bacter, shigaella, e. coli, C. difficile -causes pseudomembranous colitis)
- Ischaemic colitis due to chronic vascular insufficiency
What are the symptoms of colitis?
- Diarrhoea +/- blood
- Abdominal cramps
- Dehydration (due to diarrhoea)
- Sepsis
- Weight loss or anaemia
How would you diagnose colitis?
- Xray - lead piping (loss of mucosal folds), thumb printing, toxic colon
- Sigmoidoscopy and biopsy
- Stool cultures (rule out infective colitis)
What is the management for colitis?
- IV fluid resuscitation (to address dehyrdration)
- IV steroids
- GI rest?
- Monitor with x-ray
- If failure to settle:
- Rescue medical therapy
- Surgery
- Colectomy will be curative but extreme
What is colonic angiodysplasia?
Small vascular malformation of the gut
Which part of the column does colonic angiodysplasia normally affect?
Right colon
What is the treatment of colonic angiodysplasia?
- Injection of pro-embolitic to cause it to clot (embolization) - Endoscopic ablation - Surgical resection (rare)
What are the 4 cardinal symptoms of bowel obstruction?
- Abdominal distension
- Absolute constipation (no gases or faeces)
- Abdominal pain
- Vomiting
How would you diagnose a sigmoid volvulus?
- AXR (huge coffee-bean shaped loop)
- Rectal contrast

How would you treat a sigmoid volvulus?
- Flatus tube (deflates and untwists it)
- Resection (particular if recurring)
What would you see histologically with diverticular disease?
Histologically quite boring - can see normal mucosa but with out pouches.
But also see acute and chronic inflammationn which is the cause of the weakened tensile strength
What are the underlying causes of diverticular disease?
Related to increased intralumenal pressure causes inflammation and weakening. Also associated with low fibre diet, as this means stools aren’t as bulky so need to work harder to pump them along
What will ischaemia of the bowel look like histologically?
Muscosa is diffusely erythematous and ulcerative. Can see withers crypts and build of fibrin etc.

What are some of the causes of ischaemia of the bowel?
- Atherosclerosis of mesenteric vessels (inferior mesenteric a.)
- A.Fibrillation
- Shock
- Embolus
- Vasculitis
What is pseudomembranous/c. diff colitis characterised by?
Patchy areas of exudates (adherent raised yellow and white plaques) adhering onto the inflamed mucosa surface

What does pseudomembranous/c. diff colitis look like histologically?
Can see the top mucosal layers has been sloshed off so see fibrin/exudate lying over it instead

What is the main cause of pseudomembranous/c. diff colitis?
Broad spectrum antibiotics/c. difficile
What is the pathophysiology of pseudomembranous/c. diff colitis?
Toxin A and B produced by the C. difficile attack the endothelium and epithelium
What are the cardinal symptoms of pseudomembranous/c. diff colitis?
Massive diarrhoea and bleeding
What is the treatment for pseudomembranous/c. diff colitis?
Metronidazole if mild/moderate or Vancomycin if severe. May need colectomy
Which conditions come under microscopic colitis?
Collagenous colitis and lymphocytic colitis
What is the characteristic symptoms of microscopic colitis?
Watery diarrhoea with more than 10 stools a day
What will be seen histologically with collagenous colitis?
Mucosa appears normal with normal crypts, but thick layer of collagen is laid down adjacent to the mucosa

What is the only way of diagnosing microscopic colitis?
Biopsy (appears normal on endoscopy)
What will be seen histologically with lymphocytic colitis?
Surface epithelium is entirely lymphocytes

What should be thought of in patients who previously had prostate/cervical cancer and now have colitis symptoms?
Radiation colitis
What does radiation colitis look like histologically?
The mucosa no longer looks like rack of test tubes, but its fairly irregular. Can see blood vessels with abnormal, thickened walls
What is Telangiectasia, which is common with radiation colitis
Dilatation of the capillaries causing them to appear as small red or purple clusters, often spidery in appearance, on the skin or the surface of an organ.
What does semi-digested food in the vomitus suggest about the bowel obstruction?
Gastric outlet obstruction
What does copies bile-stained fluid in the vomitus suggest about the bowel obstruction?
Small bowel obstruction
What does thicker, brown, foul smelling vomitus (‘faeculent’) suggest about the bowel obstruction?
Distal obstruction
What causes the distension symptoms in bowel obstruction?
Caused by swallowed air and intestinal fluid secreted proximal to an obstruction causes pain.
Why is there colicky pain with bowel obstruction?
Peristalsis attempts to overcome the obstruction
True or False: Symptoms are more gradual in large bowel obstruction compared to small
True, due to the large capacity of the colon/caecum and their absorptive activity
What happens if the bowel is only partially obstructed (incomplete obstruction)?
Clinical features may be less clearly defined e.g. Vomiting may be intermittent and bowel habit erratic. Chronic incomplete obstruction leads to gradual hypertrophy of the muscle of the bowel wall proximally.
What are the physical signs of obstruction?
- Dehydration (dry mouth, loss of skin turgor and elasticity)
- Abdominal distension
- Visible peristalsis
- Relative lack of abdominal tenderness (obstruction with tenderness may indicate bowel strangulation)
- Obstructing abdominal mass may be palpable
- Resonant on percussion
- Bowel sounds are traditionally described as high-pitched and tinkling.
Where do distended small bowel loops tend to lie?
In a central position
What are valvular coniventes?
Rings in the obstructed small bowel crossing the whole width of SI only. Like ‘stacked coins’
Where do distended large bowel loops tend to lie and with what features?
Anatomical position with haustra coli
What are some of the inflammatory causes of bowel obstruction?
Crohn’s or diverticular disease
Which areas of the bowel are most commonly affected by diverticular disease?
Sigmoid colon, as it is the most affected by increased pressure due to hardened faeces etc
What is intussusception in terms of bowel obstruction?
A segment of bowel wall becomes telescoped into the segment distal to it, like stacked cups. Usually initiated by a mass in the bowel wall

What is bowel strangulation?
Strangulation occurs when a segment of bowel becomes trapped so that its lumen becomes obstructed (incarcerated) and its blood supply compromised (strangulated). e.g. if twisted
What are the 2 main types of adynamic bowel obstruction?
Paralytic ileus (small intestine) or pseudo-obstruction (large intestine)
What is an important feature on CT scan of adynamic bowel obstruction?
There is no transition point as with other bowel obstructions (i.e. no distended bowel proximal and collapsed bowel distal to the site of obstruction)
What is paralytic ileus?
Disruption of the normal propulsive activity of the GI tract, due to failure of peristalsis
What are the 3 main risk factors for paralytic ileus?
- Recent GI surgery
- Inflammation with peritonitis
- Diabetic ketoacidosis
What is pseudo-obstruction (oglivies syndrome)?
Acute dilatation of the colon in the absence of colonic obstruction in acutely unwell patients
What is the underlying cause of pseudo-obstrctuion?
Sympathetic system has overridden the parasympathetic, preventing peristalsis contraction. The colon fills with gas.
What is pseudo-obstruction associated with?
- Hip replacement
- Coronary artery bypass (CABG)
- Spinal procedures
- Pneumonia
- Frail/elderly patient
What is Irritable Bowel Syndrome (IBS)?
Chronic, relapsing problem of abdominal pain associated with bloating and change in bowel habit
What group of people is IBS most common in?
Females aged 20-40
What are the 3 types of IBS?
- Diarrhoea predominance – IBS-D
- Constipation predominant – IBS- C
- Mixture (alternating of the 2) – IBS –M
What are the 4 main factors in the pathophysiology of IBS?
1) Visceral hypersensitivity
2) Disturbed GI motility
3) Environment
4) Genetics
What is the disturbed motility associated with IBS and how does it manifest?
High-amplitude propagating contractions. Manifests as exaggerated gastro-colic reflex (urge to go to the toilet after every meal rather than just in morning) and pain
What are the mechanisms of visceral hypersensitivity in IBS?
- Peripheral sensitisation:
- Inflammatory mediators, eg. Cytokines, up-regulate sensitivity of nociceptor terminals
- Central sensitisation:
- Increased sensitivity of spinal neurones
What is the Rome III criteria for IBS?
- Recurrent abdominal pain/discomfort for at least 3 days per month for 3 months + 2 or more of:
- Improvement with defecation
- Onset assoc. with change in stool frequency
- Onset assoc. with change in stool form (appearance)
Which other conditions are associated with IBS?
- Fibromyalgia
- Chronic fatigue syndrome
- Temporomandibular joint dysfunction
- Chronic pelvic pain
True or False: 50% of IBS is associated with psychological features e.g. depression, anxious
True
What are the red flag symptoms which should prompt you to look for more sinister conditions before IBS?
- Age > 50
- Short duration of symptoms
- Woken from sleep by altered bowel habit
- Rectal bleeding
- Weight loss
- Anaemia
- FH of colorectal cancer
- Recent antibiotics
What is the management of IBS?
Diet: regular meal times and reduce fibre Drugs: stop any opiates, and give antidiarrhoeals, anti-spasmodics or anti-depressants depending on predominance
What are examples of anti-spasmodics?
Mebeverine and Hyoscine
What is a common antidiarrhoeal?
Loperamide
What is an example of a tricyclic anti-depressant?
Amitriptyline
What is the adenoma-carcinoma sequence?
All colonic adenocarcinoma originate from colonic adenomas: Normal > APC mutation > Early adenoma > K-ras mutation> Late adenoma > p53 mutation> Adenomacarcinoma. (but not all adenomas are pre-malignant)

What are the molecular events associated with the adenoma-adenocarcinoma sequence?
- loss of methyl groups in DNA,
- activated oncogenes, such as K-ras,
- mutation and inactivation of p53 gene
Which 2 staging systems are used in colorectal cancer?
Dukes’ (A, B, C and D) or TNM
What are 3 protective factors in colorectal cancer?
Vegetables, fibre and exercise
What are 4 causative factors in colorectal cancer?
Red and processed meat, smoking, alcohol and obesity
What are the 2 autosomal dominant conditions associated with colorectal cancer?
Familial Adenomatous Polyposis (FAP) and Heridtory Non-Polyposis Colorectal Cancer (HNPCC)
What is Familial Adenomatous Polyposis (FAP) characterised by?
Multiple (>100) colonic adenomas which may progress to carcinoma (due to probability from sheer number)
Which gene is mutated in Familial Adenomatous Polyposis (FAP)?
APC gene
Which mutation is involved in HNPCC?
Mismatch repair genes
What are predisposing conditions for colorectal cancer?
Adenomatous polyps, UC and Crohn’s
Which are the 3 most colon areas for colorectal cancer (in order)?
1) Rectosigmoid
2) Left and transverse colin
3) Right colon
Which symptoms are particularly associated with colorectal cancer in the caecum?
Anaemia
Which symptoms are particularly associated with distal colorectal cancer e.g. in the rectum?
- Blood in stool
- Altered bowel habit
- Tenesmus (rectal specifically)
What investigations would you do for colorectal cancer?
- Barium enema
- CT colonography
- Sigmoidoscopy
- Colonoscopy
What characteristic feature might you see on barium enema for colorectal cancer?
Apple core strictures
What is Faecal Occult Blood Testing (FOBT)?
Main form of screening for colorectal cancer. Stool Guaiac test - which means looking for hidden traces of blood in faeces (‘occult’ = hidden)
In colorectal cancer, what causes emergency presentation?
Obstruction mainly (but also bleeding and perforation)
What is the surgical options for colorectal cancer?
- Hemicolectomy (L or R)
- Transverse colectomy
- Sigmoid colectomy
- Subtotal colectomy
- Anterior resection
- Abdomino-perineal excision
When is radiotherapy and chemotherapy used with colorectal cancer?
Radiotherapy - palliative.
Chemotherapy - for advanced disease (media survival of 5 months)
What is the normal histological of the bowel?
Normal bowel is lined with epithelium organised into folds with goblets cells. These secrete mucous to help lubricate the movement along the bowel

What is a polyp?
A polyp is a protrusion above an epithelial surface (a tumour/swelling)
What are the 3 main types of colonic polyp?
Adenoma, serrated polyp and polypoid carcinoma
What are the 3 different shapes of polyps?
Pedunculate - hand on stalk like a mushroom
Sessile - flat carpet like
Flat - barely protrude above epithelium

True or false: all adenomas are dysplastic
True
What are Dukes stages?
A - confined to muscular propria
B - Through muscular propria
C - Metastatic to lymph nodes
How many polyps characterise HNPCC?
<100
When does FAP and HNPCC normal present?
FAP - early onset (teens/20s) and HNPCC - late onset (50-60s)
What are haemorrhoids?
Enlarged vascular cushions in the lower rectum and anal canal
How do haemorrhoids present?
- Painless bleeding
- Fresh, bright red blood, not mixed with stool, usually on the paper
- Perianal itchiness – occurs due to mucous discharge so like a nappy rash as wet all the time
- No change in bowel habit, no weigh loss or other associated symptoms
Where are haemorrhoids most commonly fund in the rectum and why?
The classical position of haemorrhoids corresponds to the branches of the superior haemorrhoidal artery occuring at 3 , 7 and 11 o’clock position with the patient in the lithotomy position
How would you diagnose haemorrhoids?
- PR exam
- Sigmoidoscopy
- Proctoscopy
What is the management of haemorrhoids?
- Symptomatic
- Surgical: HALO/THD procedure most common now
- haemorrhoid artery ligation
In which group of people is rectal prolapse most common?
Older ladies
How does rectal prolapse present?
- Protruding mass from anus especially during defecation
- Bleeding and passing mucus per rectum is common
- Examination usually shows poor anal tone
What is the management for complete rectal prolapse?
- Bulking agent and education on manual reduction in those too frail for surgery
- Delorme’s procedure
- Stitching everything up from the bottom and fixing it
- Perineal rectopexy
- Resect the prolapsed bowel
- Abdominal rectopexy
- Lifting rectum via keyhole surgery and fixing it to the sacrum
What is the management for incomplete rectal prolapse?
Dietary advice and treatment of constipation. Similar to that of haemorrhoids
What are anal fissures?
Tear in the anal margin due to passage of a constipated stool
How do anal fissures present?
- Acute onset of severe anal pain usually following episode of constipation “like passing glass”.
- Pain lasts for up to half an hour after defecation
- Bright rectal bleeding
What is the treatment for anal fissures?
- Dietary advice, stool softeners
- Pharmacological sphyncterotomy
- Causes relaxation of the sphincters
- Lateral sphyncterotomy
- Botox injection
What are fistulas in ano?
Abnormal communication between the internal anal canna and one or more external openings on the peri-anal skin
What are some of the conditions that can cause fistulas in ano?
Anorectal abscess. Crohn’s, TB and carcinoma
