9 - Rheumatology Histories and Exams Flashcards
What are the main symptoms of rheumatological disease?
- Pain
- Swelling
- Stiffness
- Fatigue
- Weakness

What questions do you need to ask in the history if someone is complaining of pain?
What?
Why?
When?
How bad?
Where?
Who? (patient’s social support, mental health etc)

Why do many patients with arthritis develop chronic pain?
Central sensitisation of pain processing cells in dorsal horn
Pain can come from synovium, joint capsule, subchondral bone, peri-articular muscle
How can you tell if pain is articular or peri-articular in origin?
If peri-articular usually only triggered by certain movements but articular is all movements
e.g Tennis elbow pain is felt on resisted wrist extension
How can the pattern of pain in joints help to make a diagnosis?
Certain rheumatological diseases have characteristics that make them more likely
e.g if the spine is involved not likely to be RA, more likely to be ankylosing spondylitis

What are some causes of acute and chronic monoarthritis?

What are some causes of acute and chronic polyarthritis?

What are the differentials for arthritis of the DIPJs?
- OA (most common cause and often Herbeden’s nodes)
- Psoriatic arthritis (will be nail dystrophy)
When a patient presents complaining of stiffness, what are some questions you need to ask?
Stiffness is a feeling of difficulty moving a joint

- Early morning stiffness? (> or < 30 minutes)
- Generalised or loalised?
- Worse after resting?
When a patient presents with joint swelling, what are some questions you need to ask?
- How rapidly did it come on?
- How long goes the swelling last?
- Does the swelling occur parallel to joint line indicating true joint swelling or does it cross the joint line?
- Is the swelling bony?
- Does the swelling extrude any material?
Fill in this table to distinguish the differences between mechanical and inflammatory diseases.


After taking a history of the presenting complaint, what other areas of the history do you need to explore?
ALWAYS CHECK EXTRAARTICULAR SYMPTOMS

What are constitutional symptoms?
Symptoms that are not disease specific e.g fever, weight loss, fatigue, and lymphadenopathy but can indication underlying inflammatory disease, infection or neoplasia
Common in: AS, Primary vasculitis, GCA
Uncommon in: RA and PsA. SLE has fever but not others
What rheumatological diseases are the following extra articular symptoms and signs associated with?


What rheumatological diseases are the following extra articular symptoms and signs associated with?


What are the basics of an MSK exam?
- Introduction
- GALS
- Look
- Feel
- Move (Active and Passive)
- Special tests

How do you perform a GALS assessment?

- Introduction and gain consent
- Screening questions
- Gait
- Arms
- Legs
- Spine
- Regional exam of a joint if any problem detected
- Thank patient and ask if they need any help dressing

How do the following gaits present?
- Antalgic
- Trendelenberg
- Sensory ataxia
- Cerebellar ataxia
- Hemiplegic
- Festinant
- Waddling
- Psychogenic

How do you perform a hand examination for an OSCE?
- Introduce and gain consent
- Hands on pillow and ask if any pain
- Inspect distal to proximal on dorsum, palmar and elbows. Look at thenar/hypothenar
- Feel
- Move
- Neurovascular
- Function
- Special tests

What would indicate a positive Tinel’s and Phalen’s test?
Test for carpal tunnel syndrome (can be caused by arthritis)
Tinel’s: tap on carpal tunnel with your index and middle finger for 30-60 seconds. If irritation in thumb and radial two figners it is positive for median nerve irritation
Phalen’s: hold wrist in forced flexion for 60 seconds, if symptoms develop then positive
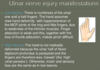
What is the sensory and motor supply of the median nerve to the hand?
Sensory: see image
Motor:
- All anterior forearm except FCU and medial two FDP
- LOAF (lateral two lumbricals, opponens pollicis, APB, FPB)

How would a median nerve palsy present?
- Weakness of thumb opposition and abduction
- Numbness in median nerve distribution (palmar sparing if lesion at wrist)
- Late thenar muscle wasting
(If damage in arm will have weak finger flexion but be able to flex ring and little finger)

What is the sensory and motor supply of the ulnar nerve?
Sensory: see image (not just fingertips on back)
Motor:
- FCU
- Medial FDP
- Interossei and adductor pollicis

How will an ulnar nerve palsy present?
- Wasting of hypothenar
- Numbness in distribution of ulnar nerve
- Froment’s test
- Claw Hand in low lesion
What are some important blood tests to order if you suspect rheumatological disease and why are they abnormal?

What are the advantages and disadvantages of the following inflammatory markers
- ESR
- CRP
- PV
ESR and PV looks at immunoglobulins and fibrinogen

What auto-antibody tests should you order if you suspect a patient has RA?
- Rheumatoid Factor (RF is antibody against Fc region of human IgG)
- Anti-CCP/ACPA (more specific for RA)

Antinuclear antibodies are produced against nuclear antigens. You order these tests if you suspect an autoimmune disease. What are the following ANA’s associated with?
- Anti-dsDNA
- AntiRO and AntiLa
- Anti centromere and anti Scl70
- Anti Jo-1

What is HLA-B27?
Class 1 surface antigen associated with ankylosing spondylitis, iritis, juvenile arthritis
Apart from taking blood tests for autoantibodies, HLA-B27 and general bloods, what other investigations can you do for a suspected rheumatological disease?
- Urinalysis: proteinuria and haematuria could be present in SLE/Vascultitis
- Joint aspiration: synovial fluid aspiration to look at crystals and rule out sepsis
- Radiology (US, XR, MRI, DEXA for osteoporosis): look for common radiological features
- Biopsy: such as temporal artery biopsy for GCA, muscle biopsy for polymyositis, lymph node biopsy to rule out TB/lymphoma in SLE
- NCS and EMG: confirm peripheral nerve entrapment and record spontaneous muscle activity

What medical specialities are on a rheumatic MDT?
- Rheumatologist
- Rheumatology nurse specialist
- Physiotherapist
- OT
- Orthotist
- Dietician
- Orthopaedic surgeon
- Psychologist
What are some causes of positive ANA?
- Auto-immune rheumatic diseases e.g. SLE, RA, Sjogren’s sydrome
- Chronic liver disease
- Chronic infection
- Malignancy
- Drug-induced e.g. minocycline
What are some mono, oligo and poly-arthritis?

What drugs are used to treat RA and therefore what monitoring is needed?
1st Line:
- DMARDs like methotrexate, sulfasalazine and hydroxychloroquine
- Steroid cover with Prednisolone for 3 months until start to work
- Need to monitor FBC and LFT
2nd Line:
- Biologics (see image)
- Need to do pretreatment screening for TB, Hep B/C and HIV

What are the side effects of the following DMARDs used for RA treatment:
- Methotrexate
- Leflunomide
- Sulfasalazine
- Hydroxychloroquine
Methotrexate: nausea, oral ulcers, hepatitis, hair thinning, pneumonitis (do pretreatment CXR), teratogenic, bone marrow suppression
Leflunomide: teratogenic, GI upset, hypertension, hepatitis, oral ulcers, bone marrow suppression
Sulfasalazine: GI upset, rash, hepatitis, oral ulcers, decreased sperm count
Hydroxychloroquine: retinopathy so pre treatment and annual eye screening

What DMARDs are completed contraindicated in pregnancy and breast feeding?
- Methotrexate
- Leflunomide
- Cyclophosphamide
What advice is given to patients started on DMARDs?
- Patient nurse-led education on side effects
- Annual flu and pneumovax
- Avoid live vaccinations with more immunosuppressive DMARDs
What are the mechanism of action of the following biologics used for RA treatment?
- Infliximab/Adalimumab/Etanercept
- Rituximab
- Tocilizumab
- TNF-a inhibitor which is 1st line biologic
- CD20 inhibitor so B-cell depletion
- IL-6 inhibitor used in combination with methotrexate if TNF-a inhibitor has failed. Measure for hypercholesterolaemia
What are some of the side effects of biologics?
- Reactivation of Hep B and TB so make sure to screen
- Immunosuppression so risk of infection
- Malignancy risk

What are some biologics that can be used to treat AS and psoriatic arthritis?
IL-17A antagonists
What are some biologics that can be used to treat Crohn’s and enteropathic arthritis?
-IL-12/23 inhibitors (Ustekinumab)
-Anti-TNF (Infliximab or Adalimumab)
What are the side effects of azathioprine, ciclosporin and cyclophosphamide?
Cyclophosphamide can also cause haemorrhagic cystitis.

Vitamin D and Calcium are also co-prescribed for osteoporosis. Oral bisphosphonates like alendronic acid can also be used. If these are not tolerated, what other drugs can be given?
- IV bisphosphonate e.g zoledronic acid
- Subcutaneous denosumab
What gout medication should be avoided in renal failure?
- Allopurinol
- Colchicine
When starting a patient on steroids for PMR, what information should you give then?
- No long lasting damage to muscles or joints / excellent prognosis
- Rapid improvement in symptoms with corticosteroids
- Likely to need treatment for 1-2 years
- Relapse common but responds to re-starting/ increasing dose of steroids
- Side effects of long-term steroids
What other investigation for GCA can you do apart from temporal artery biopsy?
Temporal Artery US

What are the lyrics to Prince of Kurdistan?
Na, na-na
Na, na-na
Na, na-na
Na, na-na
I don’t want Mo, I just want Birun
I don’t need Mo, I just want Birun
I don’t want Mo, I just want Birun,
I don’t need Mo, I just want Birun
Just wanna be honest,
I’ll get my trims with you regardless
