3 - ECGs and Bradyarrhythmias Flashcards
What is the protocol for reading an ECG?
- Confirm patients name and ECG date
2. Rate
3. Rhythm
4. Axis
5. P waves
6. Intervals: PR interval, QRS complex, QT interval, ST segment, T waves
- R wave progression

What time interval does each of the following on an ECG represent:
- 1 small box
- 1 large box
Small box: 0.04 seconds
Large box: 0.2 seconds
1 second is represented by 5 large boxes

How do you calculate the rate on an ECG? (assuming speed is 25mm/s)
Regular: 300 ÷ Number of Big squares between R-R
Irregular: Number of QRS complexes on rhythm strip (10 seconds) x 6
Normal is 60-100bpm

How do you work out the rhythm of an ECG?
Use card method to mark position of 3 successive R waves and see if all intervals equal
Can be irregularly irregular or regularly irregular or sinus arrhythmia (p waves but irregular)

What is sinus rhythm?
- All QRS complexes preceded with a P-wave
- Regular rhythm
- Between 60-100bpm
What is sinus arrhythmia?

Slight but regular lengthening and then shortening of RR intervals. All QRS have P waves so sinus node still working
Common in young people, lengthening and shortening corresponds to breathing

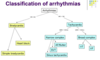
What is the difference between AF and atrial flutter?
AF: has no p-waves and is irregularly irregular
Atrial flutter: sawtooth baseline with no discernible p-waves but it is regular

What is the axis on an ECG and what is a normal axis?

Describes the direction of depolarisation across the heart, should spread from 11 to 5 o clock (-30 and +90)
Need to look at JUST LIMB LEADS/ leads I, II and III. There should be positive deflections for a normal axis.
Most positive deflection should be in II and most negative should be aVR

How do you work out axis on ECG easily?
Normal: Lead II or I most positive
Left deviation: aVL/Lead I most positive
Right deviation: Lead III most positive

What are the causes of right and left axis deviation?
Right: right ventricular hypertrophy, PE, anterolateral MI, WPW, left posterior fasicle block
(normal in very tall individuals, associated with pulmonary oedema as RVH)
Left: conduction abnormalities, left anterior hemiblock, inferior MI, WPW, LVH

How can you distinguish right and left axis deviation on an ECG?

Right: lead I becomes negative and lead II, III/aVF become more positive (Lovers Returning)
Left: lead III and II become negative and lead I more positive (Lovers Leaving)

What are the normal time values for the following and where are these intervals on ECG:
- PR interval
- QRS complex
- QT interval
- ST interval
PR: start of P to start of QRS. 0.12-0.2s (3-5 small squares)
QRS: <0.12S
QT: start of QRS to end of T. Should be 0.38-0.42s
ST interval: end of S to start of T

After looking at rate and rhythm on ECG you look at P waves. What are you looking for?
- Are they present?
- Are they followed by a QRS
- Should be upright in II, III, aVF but upside down in aVR
- Flat, flutter or chaotic baseline?

What is the normal PR interval and what can shorten and lengthen this?
3-5 small squares (0.12-0.2 seconds)
Prolonged: Delayed AV conduction e.g heart block
Shortened: fast AV conduction via accessory pathway e.g WPW or SA node in different place

What is a normal QRS complex like and what can cause changes to the QRS complex?
- Width
- Height
- Morphology
Should be <0.12s with Q waves being <0.04s wide and <2mm deep
Prolonged QRS: bundle branch block, metabolic disturbance, ventricular origin
Tall QRS (>5mm in limb leads, >10mm in chest leads): LVH
Pathological Q-Waves: following MI

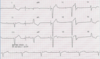
What are the QRS complexes on this ECG showing?

Delta wave which is common in Wolf Parkinson White Syndrome
Sign that ventricles are being activated earlier than normal from a point distant to the AV node. Early activation spreads slowly across myocardium causing slurred upstroke of QRS

WPW cannot be diagnosed with the delta wave alone. What other ECG abnormality has to be present?
Tachyarrhythmia + Delta Wave
When is a Q wave pathological?
> 25% the depth of the QRS that follows it or > 2mm in height and >1mm (40ms) in width.
Single Q wave is ok, need to look for Q in whole territory for evidence of previous MI e.g look at all inferior leads
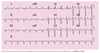
What is wrong with the QRS complexes in this ECG and why might this have occured?

Poor R wave progression
R wave should go from small to big from V1 to V6. Transition of S>R to R>S should be around V3/V4
Poor lead position or previous MI

What is the J point?
Where the S wave joins the ST segment

What is the Osborn wave (J wave)?
Positive deflection of the J point due to hypothermia, SAH or SEVERE hypercalcaemia

What is a normal ST segment and what is ST elevation/depression?
Should be isoelectric
ST elevation: greater than 1 mm (1 small square) in 2 or more contiguous limb leads or >2mm in 2 or more chest leads.
ST depression: >0.5mm in >2 contiguous leads
What is the cause of ST elevation and ST depression?
Elevation: full thickness myocardial infarction
Depression: myocardial ischaemia
What do T waves represent and what leads are they normally inverted on?
Ventricular repolarisation
Usually inverted in aVR, V1 and V2 and sometimes V3
Abnormal if inverted in I, II, V4-V6