5 - Hepatobiliary Flashcards
What is a splenic infarct?
Occlusion of the splenic artery or one of its branches resulting in tissue necrosis
Often not complete necrosis due to collateral supply from splenic artery and short gastric (left gastroepiploic)

What is the aetiology of a splenic infarct?
- Haemotological Disease: Lymphoma, Myelofibrosis, Sickle cell, CML, Polycythemia Vera, Hypercoagulable states
- Thromboembolism: endocarditis, AF, post MI mural thrombus,
- Rare causes: trauma, vasculitis, liver surgery, panreatectomy

How do haemtological diseases cause splenic infarction?
Congestion of the splenic artery with abnormal cells
What are the clinical features of a splenic infarct?
- Often asymptomatic
- LUQ pain/tenderness that radiates to the left shoulder (Kehr’s sign)
- Fever
- N+V
- Pleuritic chest pain

What differential diagnoses can be considered when a patient presents with symptoms of a splenic infarct?
- Peptic ulcer disease
- Pyelonephritis
- Ureteric colic
- Left sided basal pneumonia
What investigations should be done if you suspect a splenic infarct and what will the findings be?
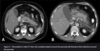
- Gold standard: CT abdomen with IV contrast
Will show segmental wedge shaped infarct towards hilum of the spleen. Whole spleen hypoattentuated if splenic artery occluded not a branch
- Routine bloods: FBC, LFTs, U+E’s, coagulation screen

What is the immediate and long term management for a patient with a splenic infarct?
Immediate:
- Analgesia
- IV fluids
- Manage underlying condition
- Consider long term anticoagulation
- Avoid splenectomy due to OPSI
Long-term:
- Vaccination against encapsulated bacteria NHS
- Prophylatic low dose abx (Penicillin V)

What are the complications of a splenic infarct?
- Splenic rupture: do splenectomy
- Splenic abscess: when cause of infarct was non-sterile embolus e.g infective endocarditis. May be seen on CT scan but confirmed with explorative surgery
- Pseudocyst formation
- Autosplenectomy: causes asplenism. Repeated splenic infarcts leads to progressive fibrosis and atrophy of the spleen. Common in sickle cell as when crises there is splenic artery occlusion. Leaves patient susceptible to infection

What are some of the causes of splenic rupture?
- Blunt trauma: seatbelt injuries, falls onto the left side
- Iatrogenic
- Splenomegaly: EBV, haemtological malignancy. Cause capsule to stretch and thin so susceptible to rupture

What are the clinical features of splenic rupture?
- Abdominal pain
- Hypovolemic shock
- LUQ tenderness/Peritonism
- Kehr’s sign due to diaphragm irritation

What investigations do you do for a suspected splenic rupture?
Haemodynamically unstable with peritonism: immediate laparotomy
Haemodynamically stable: urgent CT chest-abdomen-pelvis with IV contrast

How do you grade splenic injuries?
- American Association for the Surgery of trauma.
- Used to help guide which patients should have conservative maagement and which should have surgical

How should we manage patients with splenic rupture?
All: assessed and resuscitate with ATLS protocol
Haeodynamically unstable/Grade 5: Urgent laparotomy
Haemodynamically stable/Grade 1-3: Conservative. Move to high dependency area on strict bed rest and regular abdominal exams for deterioration. CT repeated 1/52 post injury. Increasing tenderness or peritonitis re-image/laparotomy/embolisation. Prophylatic vaccinations on discharge

What are the main complications of conservative treatment and embolisation treatment for splenic rupture?
- Ongoing bleeding
- Splenic necrosis
- Splenic abscess or cyst formation
- Thrombocytosis (give aspirin if platelet count rises)
- OPSI so give prophylatic Penicillin V and vaccinations to prevent sepsis

What is bile made from?
Stored in the gallbladder until released to duodenum:
- Cholesterol
- Phospholipids
- Bile pigments from Hb metabolism

What are the three main types of gallstones?
- Cholesterol: linked to poor diet and obesity
- Pigment : due to excess bille pigment production, seen in haemolytic anaemias
- Mixed: both cholesterol and bile pigments

What are the risk factors for gallstones?
5 F’s:
- Fat
- Female
- Fertile
- FHx
- Forty
Also: pregnancy, COCP (oestrogen causing more cholesterol in bile), haemolytic anaemia, malabsorption (e.g Crohn’s)

What are the clinical features of biliary colic?
- Sudden, dull, colicky pain in RUQ that may radiate to back or epigastrium
- Precipitated by eating fatty foods due to release of CCK causing gallbladder contraction
- Can be N+V
- Settles with pain relief and no inflammatory response

What are the clinical features of acute cholecystitis?
- Constant pain and tenderness in RUQ/epigastrium
- Signs of inflammation e.g fever or lethargy
- Murphy Sign +
- Guarding may suspect peritonitis/sepsis

What investigations should you do if someone presents with RUQ pain that you suspect to be gallbladder related?
- Lab tests (see image):
- FBC, CRP, LFTs, Amylase, Pregnancy
- Imaging:
- Transabdominal US 1st line
- MRCP Gold standard if US inconclusive

What would you see on ultrasound with gallstone pathology?
- Gallstones or sludge
- Thickened gallbladder wall if inflamed
- Bile duct dilatation (stone in the distal bile ducts)

How is biliary colic managed?
- Analgesia
- Lifestyle advice (weight loss, low fat diet, exercise)
- Elective laparoscopic cholecystectomy within 6 weeks due to high risk of recurrence/complications

How is acute cholecystitis managed?
- IV Abx (Co-amoxiclav +/- Metronidazole)
- Analgesics
- Antiemetics
- IV fluids
- Laparoscopic cholecystectomy within a week, better within 72 hours of presentation
- Percutaneous cholecystostomy if not fit for surgery/not responsive to abx. Drains infection

What is the difference between MRCP and ERCP?
MRCP - Identifies any biliary obstruction
ERCP - Identifies any biliary obstruction and allows for intervention