11 - Ophthalmology Conditions 1 Flashcards
What is the worldwide leading cause of irreversible blindness?
Glaucoma
Collection of disorders resulting in progressive optic neuropathy. Can have raised IOP but doesn’t need to be raised for a diagnosis
What is the pathophysiology of acute angle closure glaucoma?
EMERGENCY!
Angle of the anterior chamber narrows acutely so rise in IOP >30mmHg, this leads to optic nerve damage.
This is due to the iris bulging forward blocking off the trabecular meshwork so aqueous humour cannot drain. Increased pressure on iris then blocks it off further
Primary angle closure: Anatomical predisposition
Secondary angle closure: Due to pathological processes e.g traumatic haemorraghe pushing the posterior chamber forwards

What are some of the risk factors of acute angle closure glaucoma?

- Increasing age
- Female
- Chinese and East-Asian ethnicity
- FHx
- Hypermetropia (long-sightedness/shallow anterior chamber)
- Medications: TCA, anticholinergics (as parasympathetics constrict pupil). Adrenergics

How will somebody with acute angle closure glaucoma present and what will you find on examination?
Presentation (Systemically unwell)
- Severely painful red eye
- Blurred vision
- Halos around lights
- Headache, Nausea, Vomiting (often mistaken for gastroenteritis until you look in their eye)
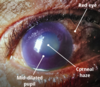
Examination
- Red eye
- Fixed mid-dilated pupil
- Corneal haze
- Teary
- Decreased visual acuity
- Firm eye on palpation
What investigations are done if you suspect acute angle closure glaucoma?
- Tonometry
- Gonioscopy: look at anterior chamber and drainage system
- Slit lamp/Opthalmoscopy: optic disc cupping
- OCT?

How do you manage acute angle closure glaucoma?
Initial (Triad)
- Lie on back, avoid dark room as will dilate pupil and make worse
- Timolol (B-blocker to reduce aqueous humour production)
- Pilocarpine drops (muscarinic that causes miosis so pupil constriction opening angle up)
- Acetazolamide 500mg IV (carbonic anhydrase inhibitor that reduced aqueous humour production)
- Analgesia and Antiemetic
Definitive
- Bilateral Peripheral Laser Iridotomy once IOP lowered. Remove piece of iris so always drainage between anterior and posterior chamber. Often do other eye too as at risk of angle closure

Apart from the triad of pilocarpine (4% for darker eyes, 2% for lighter), azetazolamid and timolol for acute angle closure glaucoma, what are some other medications that can be used?
- Hyperosmotic agents: e.g glycerol or mannitol increase the osmotic gradient between blood and fluid in eye
- Brimonidine: sympathomimetic that reduces the production of aqueous fluid and increase uveoscleral outflow
What is the prognosis with acute angle closure glaucoma?
- If not treated can lead to visual loss
- Can occur to contralateral eye so make sure definitive treatment is done on both eyes
- CRAO (due to dramatic rise in IOP)

There is no formal screening test for glaucoma, however what patients are recommended to have regular reviews by optometrists?
Elderly: over 60 every 2 years, over 70 every year, free on NHS
FHx of Glaucoma: over 40 with first degree relative that has/had glaucoma then every year have eye test, free on NHS
Black African: over 40 should have test ever year, not free on NHS
Important to screen as asymptomatic until visual fields are affected and by this point it is too far!!!

What tests are performed to screen for and diagnose open angle glaucoma?

- Tonometry (Non-Contact or Goldmann Application is gold standard): increased pressure
- Fundoscopy: optic disc cupping (>0.5)
- Visual fields
- Can also measure corneal thickness and do gonioscopy to look at drainage of humour

What is the pathophysiology of open-angle glaucoma?
Increased resistance in trabecular meshwork so more difficult for aqueous humour to flow through so builds up in the eye and increases the pressure slowly over time

Why is there cupping in chronic glaucoma?

Normal optic cup is <0.5 the size of the optic disc.
When there is an increased pressure in the eye this puts pressure on the cup making it wider and deeper so >0.5 the size of the optic disc
Loss of disc makes the cup look larger

What are some risk factors of chronic open angle glaucoma?
- Increasing age
- FHx
- Myopia (short sighted)
- Black ethnicity
- ?Diabetes
- ?HTN

How does chronic simple (open-angle) glaucoma present?

- Asymptomatic at start and only picked up on screening
- Tunnel vision as gradual loss of peripheral vision
- Fluctuating pain
- Headaches
- Blurred vision
- Halos around lights especially at night

How are patients with open angle glaucoma managed?
When does treatment commence?

Treatment starts when IOP is 24 or more. Aim is to reduce IOP to slow progression but cannot reverse
1st Line:
- Topical prostaglandin analogue (Latanoprast): increase uveoscleral outflow
2nd Line:
- Topical beta-blocker (Timolol): reduce production of aqeuous humour
- Topical carbonic anhydrase inhibitor (Dorzalamide): “
- Topical sympathomimetic (Brimonidine):” and increases uvoscleral outflow
3rd Line:
- Trabeculotomy or Laser Trabeculoplasty: path from sclera to conjuctiva by bleb

What are some complications of a trabeculotomy?
- Early failure
- Hypotony
- Bleb leakage
- Infection
What are the side effects of the following topical drugs used in treatment of open angle glaucoma:
- Lanatoprost
- Timolol (beta blocker)
- Brimonidine (alpha agonist)
- Dorzalamide
- Pilocarpine

- Lanatoprost: eyelash growth, iris browning, skin pigmentation
- Timolol: dry eyes, corneal anaesthesia, reduced exercise tolerance, be careful in heart failure and asthma as can be absorbed systemically
- Brimonidine: lethargy, dry mouth
- Dorzalamide: lethargy, reduced K+, dyspepsia, avoid in pregnancy
- Pilocarpine: brow ache, decreased visual acuity
ALL DROPS CAN BE ABSORBED SYSTEMICALLY SO S/E

What is blepharitis and how is it managed?
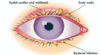
- Inflammation of the eyelid margins causing itchy, dry, gritty eyes
- Could be due to staphs, seborrhoeic dermatitis, or rosacea
- Management: lid hygeine, hot compress, cotton bud with diluted baby shampoo cleaning twice a day, lubricating eye drops

What is a stye and how is it managed?
Hordeolum externum: Infection of the glands of Moll (sweat) and glands of Zeiss (sebaceous). They point outwards and are a red tender lump
Hordeolum Internum: Infection of tarsal glands, points inwards, more painful, can turn into chalazion
- Mx: apply hot compress several times a day until disappears, analgesia

What is a chalazion (meibomian cyst) and how is it managed?
- Inflammation of the tarsal meibomian glands due to blockage of the gland. Points inwards and is painless
- Mx: hot compress, analgesia, rarely surgery to remove
What is entropion and how is it managed?
- Lid inturning due to degeneration of lower lid fascial attachments and their muscles
- Inturned eyelashes irritate cornea and can cause corneal ulceration
Mx
- Tape lid to cheek. Use lubricating drops to prevent eye drying out
- Surgery is definitive
- Same day referall if worried about sight

What is ectropion and how is it managed?
- Eyelid turns outwards so the inner aspect of the eyelid is showing
- Can lead to exposure keratopathy
Mx:
- May need no treatment if mild
- Regular lubricating eye drops to protect tear film
- Surgery
What is trichiasis and how is it managed?
- Inward growth of eyelashes
- Pain, ulceration, corneal damage
- Mx: epilation, laser therapy if recurrent
What is Pinguecula?
- Degenerative vascular yellow-grey nodules on the conjunctiva
either side of the cornea. Can try topical steroids if inflammed - If invading the cornea this is a ptyergium
- Usually in adult male, increased hair and skin pigment, sun-related
skin damage

What is blepharospasm, what causes it and how is it treated?
Focal dystonia resulting in involuntary eye closure. Made worse by exaggerated blinking
Causes: Idiopathic, Parkinson’s, Neuroleptics, paraneoplastic
Treatment: Botox injections, Anticholinergics, Dopamine agonists

What are some causes of dry eyes and how are they treated?
- Reduced tear production due to old age
- Sjogrens, Sarcoidosis
- Mucin deficiency in tears
- Excessive evaporation of tears in post-exposure keratitis
- Allergies
- Blepharitis
Ix: Schirmer’s Test >15mm in 5 minutes
Mx: Artificial tears, Lubricating drops, surgery to decrease size of punctum lacrimale so slower drainage of tears

What is the aetiology of conjunctivitis and how can you tell the difference between them?

- Bacterial: mucopurulent discharge, can be bilateral but starts unilateral and spreads to other, worse in the morning
- Viral (usually adenovirus): watery discharge, usually unilateral, lasts longer, often lymph node swelling pre-auricular
- Allergic: watery discharge, seasonal or triggers, bilateral, cobblestone papillae on eyelid

How does conjunctivitis present?

- Red eyes
- Bloodshot
- Itchy or gritty sensation
- Discharge from the eye (watery in viral, mucopurulent in bacterial)
- Should be no pain, photophobia or decline in visual acuity
- Highly contagious
What are the following subtypes of conjunctivitis:
- Hyperacute
- Ophthalmia neonatorum
- Trachoma
Hyperacute: rapidly progressive that is caused by N.Gonorrhoea and N.Meningitidis. Eye produces large amounts of purulent discharge. Severe and potentially sight-threatening.
Opthalmia Neonatorum: conjunctivitis in the first 28 days of life, usually due to Chlamydia or Gonorrhoea
Trachoma: Inflammation of cornea and conjunctivitis. Chlamydia trachomatis in children in sub-Saharan Africa. Leading cause of infective blindness worldwide.
Conjunctivitis is usually a clinical diagnosis. What are some red flags that point away from conjuncitivitis and prompt and urgent referral to opthalmology?

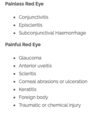
What are some differentials for a painful and painless red eye?
How is bacterial/viral conjunctivitis managed?
- Self limiting in 1-2 weeks
- Symptomatic relief: cool compress, lubricating eye drops, cleaning eyes with cooled boiled water
- Prevent spread: good hand hygeine and separate towels
- Safety netting: if photophobia, change in vision etc
- Don’t wear contact lenses until resolved
- Medical: if bacterial can give Chloramphenicol and fuscidic acid drops to speed up recovery but will still resolve on it’s own without these
- If in baby <1month urgent referral as sight threatening and risk of complications like pneumonia

Topical antibiotics should be started straight away in bacterial conjunctivitis for which patients?
- Contact lens wearers
- Immunocompromised
- Sexually transmitted
How is allergic conjunctivitis treated?
- Antihistamine drops or PO: Emedastine or olopatadine
- Sodium cromoglicate: Mast cell stabilisers to stop mast cells producing histamine. Need to use for few weeks before seeing effect
- Steroid drops

What is cataracts and what are some of the causes of this?
Opacifiation of the lens. One of the leading causes of blindness
- Congenital
- Age related
- Trauma
- Uveitis
- Scleritis
- Intra-ocular tumours
- Radiation
- Medications (e.g. corticosteroids, amiodarone)
- Systemic disease (e.g. diabetes mellitus, myotonic dystrophy, severe atopic dermatitis)

What are some risk factors for cataracts?
- Increasing age
- Smoking
- Alcohol
- Diabetes
- Steroids
- Hypocalcaemia
- UV exposure

What are the different classifications of cataracts?

Depending on the location of the lens affected
Nuclear: Involves central nucleus of the lens. Clinically there is central opacification, significant loss of colour and slow progression
Cortical: Involves the cortex of the lens. Less degradation of vision and slow progression
Posterior subcapsular: Involves the subcapsular cortex. Disabling glare to bright lights, quicker progression. Linked to diabetes and steroid use

How is congenital cataracts detected?
Absence of red reflex in newborn screening
What is the pathophysiology of cataracts?
Lens is made of soluble protein crystallin
Due to poor blood supply, containment within a capsule and inability to shed non-viable cells, lens is susceptible to damage from normal ageing and environmental insults (e.g. UV light and oxidative stress)
Central nucleus may become compressed, hardened and undergo nuclear sclerosis, which is seen clinically as opacification
Without transparency, light is unable to be refracted onto the retina

What are the signs and symptoms of cataracts?
Symptoms
- Painless slow loss of vision
- Blurring of vision
- Poor night vision
- Seeing ‘Starbursts’ around lights and sensitivity to light
- Reduction in colour intensity, everything yellow/brown
Signs on Examination
- Reduced visual acuity on Snellen charts
- Loss of red reflex
- White/grey pupil
- Nystagmus

How is cataracts diagnosed and how do you refer it onwards?
Clinical diagnosis by finding opacification on opthalmoscopy:
- Loss, or darkening, of the red reflex
- Opacification seen within the red reflex
- Obscuration of ocular detail
Refer non-urgently to opthalmologist to look in slit lamp
How is cataracts managed?
Cataracts surgery is indicated when vision is impaired to the point it is having a significant effect on activities of daily living
Removal of the diseased lens and replacement with an artificial lens
Can be done by Phacoemulsification or Standard extracapsular cataract extraction
After surgery can see retina and may be underlying pathology e.g AMD, diabetic retinopathy

What is the difference between phacoemulsification and standard extracapsular cataract examination?
- Phacoemulsification used in the UK
- Done under local anaesthetic with patient prone
- Entry to eye made via limbus (peripheral cornea) with self sealing incision
- Circular incision in anterior lens capsule is made and lens removed via US
- New lens with refractive correction placed in patients eye

What are the post-op complications with a cataracts surgery?
- Retinal detachment
- Anterior uveitis
- Vitreous haemorraghe
- Glaucoma
- Posterior capsule thickening and opacification
- Astigmatism
- Endophalmitis: Inflammation of the inner contents of the eye, usually infection that can lead to loss of vision. Intravitreal antibiotics injected into the eye

What is the recovery time following cataracts surgery?
- Use topical antibiotics for 3-6 weeks postop
- If phacoemulsification can return home immediately and resume normal activities the next day. Other methods take longer to recover
How can cataracts be prevented?
- Stop smoking
- Wear sunglasses with UV protection
- Eat antioxidants e.g vit c, caffeine
Why is it important to pick up congenital cataracts early?
Needs to be treated within first 4 weeks to prevent significant deprivation amblyopia

What is CRAO?
Occlusion of the central retinal artery (branch of ICA) which causes ischaemia of the retina and sudden monocular visual loss
Opthalmic emergency as is a stroke of the CRA

What are some of the causes of CRAO?
- Carotid artery atherosclerosis
- GCA
- Cardioembolic event from AF
- Carotid artery dissection
- Fibromuscular dysplasia

What are some risk factors for a CRAO?
- Any atherosclerosis risk factors
- Any GCA risk factors

How does a CRAO present?
- Sudden painless loss of vision
- May have central vision sparing if patent cilioretinal artery
- RAPD
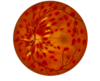
- Fundoscopy: will see pale retina (lack of blood supply) and cherry red spot (macula thinner so can see choroid through it)

If a patient has CRAO what is essential to rule out?
GCA!!! As steroids can be sight saving.
Always do ESR/CRP and temporal artery biopsy and start high dose steroids in case!!!!

How is CRAO managed?

Immediate (<100 min still poor chance of regaining vision)
- Ocular massage
- Remove fluid from anterior chamber to reduce IOP
- Inhaling carbogen (a mixture of 5% carbon dioxide and 95% oxygen) to dilate the artery
- Sublingual isosorbide dinitrate to dilate the artery
Long term:
- Reduce CVS risk factors
- Consider need for antiplatelets, statins, antihypertensives

What is the prognosis with CRAO?
- Permanent loss of vision: even if caught early
- Increased risk of CVD
- Glaucoma and Vitreous haemorraghe: the retinal ishcaemia may lead to neovascularisation and these vessels can leak

What are some of the causes and risk factors of retinal vein occlusion?
- Arteriosclerosis
- HTN
- Diabetes
- Polycythaemia
- Glaucoma

What is the presentation of central retinal vein occlusion and what is the pathophysiology behind this?
Sudden painless loss of vision if central retinal vein due to macular oedema and ischaemia. If branch retinal vein can be asymptomatic.
More common than CRAO
Pathophysiology: Blockage of blood flow so pooling of blood in retina, fluid leakage that causes macular oedema and retinal haemorraghes. Leads to the release of VEGF so neovascularisation occurs
What does fundoscopy show in CRVO?
- Flame and blot haemorrhages (cotton wool spots)
- Optic disc oedema
- Macula oedema

Apart from fundoscopy what other investigations should you do for CRVO?
- Full medical history
- FBC for leukaemia
- ESR for inflammatory disorders
- Blood pressure for hypertension
- Serum glucose for diabetes
How is CRVO managed?

- Refer immediately to oncall opthalmologist
- Treatment to control secondary complications e.g macular oedema, vision loss, neovascularisation
Treatment:
- Anti VEGF if vision loss to prevent neovascularisation
- Intravitreal steroid (dexamethasone)
- Laser photocoagulation if neovascularisation has already occured
Intravitreal steroids (e.g. a dexamethasone intravitreal implant)

What is the pathophysiology of diabetic eye disease?

Always vascular occlusion or vascular haemorraghe!!!

- Hyperglycaemia damages retinal small vessels and endothelial cells Increased vascular permeability leads to leakage from the blood vessels, blot haemorrhages and the formation of hard exudates
- Damage to blood vessel walls leads to microaneurysms and venous beading
- Damage to nerve fibres in the retina causes fluffy white patches to form on the retina called cotton wool spots
- Intraretinal microvascular abnormalities (IMRA) is where there are dilated and tortuous capillaries in the retina. These can act as a shunt between the arterial and venous vessels in the retina.
- Neovascularisation due to VEGF released
What are the different classifications of diabetic retinopathy and what do you see om fundoscopy?

Non-proliferative diabetic retinopathy: (Ischaemia)
- Mild: microaneurysms
- Moderate: microaneurysms, blot haemorhages, hard exudates, cotton wool spots and venous beading
- Severe: blot haemorrhages plus microaneurysms in 4 quadrants, venous beating in 2 quadrates, intraretinal microvascular abnormality (IMRA) in any quadrant
Proliferative Retinopathy (New vessels on retina that can leak)
- Neovascularisation
- Vitreous haemorrhage
Maculopathy (Vessels leak close to macula)
- Macular oedema
- Ischaemic maculopathy

Which diabetic retinopathy needs to be referred urgently?

- Maculopathy
- Severe NPDR
- Proliferative retinopathy

Most diabetic retinopathy is asymptomatic until it is irreversible. How is this progression prevented?

Pre-symptomatic screening to allow faster laser photocoagulation treatment
Both type 1 and type 2 need screening on diagnosis and annualy after
Screening by dilated fundus photography. Usually in posterior pole

How is diabetic retinopathy managed?
- Ensure good diabetic control and BP <140/80: do not correct refractive errors until good glycaemic control as refractive index becomes more hypermetropic with treatment
- Laser photocoagulation: for proliferative retinopathy and macula oedema
- Intravitreal Anti-VEGF and Vitreoretinal surgery: addition to photocoagulation with macula oedema

What are some things that can accelerate diabetic retinopathy and lead to blindness faster?
- Pregnancy
- Dyslipidaemia
- HTN
- Renal disease
- Smoking
- Anaemia

What are the different fundoscopy appearances of proliferative and non-proliferative diabetic retinopathy?


What are some complications of diabetic retinopathy?
(IMPORTANT)
- Retinal detachment
- Vitreous haemorrhage
- Rebeosis iridis (new blood vessel formation in the iris)
- Optic neuropathy
- Cataracts
- Glaucoma
- CN palsies (3 and 6) with pupil sparing

What is keratitis and what are some of the causes of this?
Inflammation of the cornea, usually due to infection
- Viral: Herpes simplex
- Bacterial: Pseudomonas or Staphylococcus
- Fungal: Candida or Aspergillus
- Contact lens acute red eye (CLARE)
- Exposure keratitis: Inadequate eyelid coverage (e.g. eyelid ectropion)

What are some risk factors for infective keratitis?
Usually need disruption to the epithelial surface of the cornea:
- Contact lenses
- Dry eyes
- Trauma
- Corneal disease
- Immunocompromised
How does infective keratitis present in general?
- Painful red eye (free nerve endings exposed and increased vascularity)
- Watery eye
- White deposit on cornea (corneal infiltrate)
- May have hypopyon
- Drop in visual acuity (due to corneal oedema)

How does herpes keratitis present and why is it important to be diagnosed early?
Presentation: painful red eye, photophobia, watery eye
Can lead to stromal necrosis, vascularisation and corneal scarring so corneal blindness!!!
Need to ask about previous mouth and genital ulcers

What investigations should you do if you suspect infective keratitis?

- Slit lamp exam with fluroscein staining: will show dendritic ulcer
- Corneal scrapings/swab: send for PCR

How is herpes keratitis managed?
- Same day referral to opthalmology
- Topical aciclovir or ganiclovir ointment
- Steroid drops (for stromal keratitis only use with aciclovir cover as otherwise risk of scarring and blindness)
- Corneal transplant (if significant blindness from stromal keratitis)

What are the different types of uveitis?
Can be acute or chronic (>3months and often granulomatous)
Anterior uveitis: inflammation affecting the iris (iritis) or ciliary body (iridocyclitis)
Intermediate uveitis: inflammation of posterior part of ciliary body and nearby peripheral retina and choroid
Posterior uveitis: inflammation of retina and choroid
Panuveitis: inflammation of whole uveal tract

What are some causes of anterior uveitis and some associations with other diseases?

- Autoimmune conditions
- Infection
- Trauma
- Ischaemia
- Malignancy

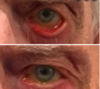
Anterior uveitis is the most common type of uveitis. How does it present?
Symptoms
- Unilateral symptoms that occur spontaneously with no trauma
- Painful red eye
- Photophobia
- Epiphoria (watery eye)
- Reduced visual acuity
- Floaters
Signs
- Ciliary flush (circumcorneal injection)
- Keratic precipitates
- Cells and flare in anterior chamber
- Posterior synaechiae
- Miosis
- Hypopyon

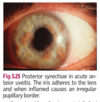
What is posterior synaechiae?
Adhesions between iris and anterior lens capsule due to inflammation
(image important for anterior uveitis)

What are important questions to ask when someone presents with anterior uveitis?
- Headache?
- Features of systemic disease?

How is anterior uveitis diagnosed?
Slit lamp with dilated pupil
If anterior will see keratic precipitates (leucocytes) and may see flare. If posterior will not see these
Can do fundus fluorescein green-angiograph

How is anterior uveitis managed?
- Red eye so same day referral to opthalmology
- Treatment is to prevent glaucoma, as adhesions can block humour flow, and decrease inflammation to improve pain
Mx:
- Prednisolone drops: decrease inflammation
- Cyclopentalate drops (antimuscarinic): keep pupil dilated to stop posterior synaechiaea, open up iridocorneal angle, stop ciliary spasm as cycloplegic to stop pain
- Biologics (anti-TNF): if systemic disease
- Laser therapy if severe

What are some of the complications of uveitis?
- Vision loss: less chance in anterior than posterior, panuveitis worse
- Macular oedema
- Cataracts
- Chorioretinal scarring
- Glaucoma
- Retinal detachment
- Vitreous opacities.

What is the pathophysiology of age related macular degeneration?
Degeneration of the macula causing gradual vision loss. Drusen present.
Most common cause of irreversible blindness
- Proteins and lipids deposit between retinal pigment epithelium and Bruch’s membrane (Drusen)
- Atrophy of the retinal pigment epithelium
- Degeneration of the photoreceptors

What is the difference in the pathophysiology of wet AMD opposed to dry AMD?
There are new vessels that grow from the choroid (Bruch’s membrane) into the retina under control of VEGF
These vessels leak and cause oedema and rapid loss of vision

What are some of the risk factors of AMD?
- Age
- Smoking
- White or Chinese ethnic origin
- Family history
- Cardiovascular disease

What is the presentation of AMD?

- Gradual worsening central visual field loss (difficulty reading, making out faces, night vision)
- Reduced visual acuity
- Crooked or wavy appearance to straight lines
- Fluctuating vision changes (some days poor some days good)
More acute over days in wet AMD that can lead to full bilateral vision loss in 2-3 years

What examinations and investigations should you do if you suspect AMD and what will they show?
Exam:
- Snellen chart: reduced visual acuity
- Scotoma in Visual Field test: a central patch of vision loss
- Amsler grid test
- Fundoscopy: Drusen (lipid deposits)
Ix:
- Slit lamp fundus exam
- OCT for wet AMD
- Fluorescein angiography can see neovascularisation in wet AMD

What do you see on fundoscopy with dry AMD and how is dry AMD managed?

- Just see drusen, visual loss occurs over decades
Mx
- Refer to opthalmologist
- No specific treatment just modify risk factors (stop smoking, control BP, vitamin supplements for antioxidants)

What do you see on fundoscopy with wet AMD and how is it managed?

- Drusen, haemorraghes, neovascularisation, fluid exudation, localised detachment of the pigment
Mx (needs to be prompt as fast vision loss)
- Stop smoking and eat lots of greens
- Intravitreal VEGF (ranibizumab, bevacizumab): give every 1/12 for a year, within first 3 months and can reverse progress
- Laser photocoagulation
- Photodynamic therapy
- Self screening
- Visual aids if lost vision

How is wet AMD followed up?
- Arrange a fluorescein angiogram at the outset and then 4–6-weekly photograph and an OCT
- Use Amsler grid, if distortions in straight lines then refer as sign of neovascularisation

Why is there a cherry-red spot in CRAO?
- The retina is pale due to a lack of blood supply.
- The macula is the cherry red spot as it has a collateral blood supply from the cilioretinal artery.
