Risk Calculations in Mendelian Inheritance Practice Questions Flashcards
II3 in the pedigree below has two brothers with hemophilia A, a bleeding disorder that is inherited as an X‑linked recessive trait. What is the risk of hemophilia for her first child?
A. 1 in 4 for a son, close to zero for a daughter
B. 1 in 2 both for sons and daughters
C. 1 in 2 for a son and 1 in 4 for a daughter
D. 1 in 2 for a son, close to zero for a daughter
E. 1 in 4 both for sons and daughters

A
Comment: With two affected sons, person I-1 definitely is a carrier (carrier risk = 1). Her daughter has equal chance of inheriting the good and the bad allele, so II-3 has carrier risk = ½ times ½ risk for passing on to next generation. The answer choices are divided into sons and daughters so nothing further is needed. If the answer choice just said, e.g., “1/8 for the child” then 1/8 would be the correct answer because that child would have ½ risk for being a boy and only boys can get the disease, girls are only carriers. Therefore an answer that is just “1/8” and answer A are saying the exact same.
II-3 in the below family has two brothers and three sons with classical hemophilia (factor VIII deficiency). Now she is pregnant again. How likely is it that this child will also have hemophilia?
A. 100% for a son, 50% for a daughter
B. 100% for a son, close to zero for a daughter
C. 50% for a son, close to zero for a daughter
D. 50% for both sons and daughters
E. 25% for a son and close to zero for a daughter

C
Comment: Person II-3 in this question is definitely a carrier now that she has affected children. The risk for the next child to receive the bad allele is ½. The answer choices are divided into sons and daughters so nothing further is needed. If the answer choice just said, e.g., “1/4 for the child” then 1/4 would be the correct answer because that child would have ½ risk for being a boy and only boys can get the disease, girls are only carriers.
Charlene’s brother has an extremely rare autosomal recessive disease. Charlene is now pregnant. What is the risk that her child will be a carrier for this disease?
A) 1/2
B) 1/4
C) 2/3
D) 1/3
E) 1/300
F) 1/150
D.
Comment: With the disease being an extremely rare disease, there is a very low chance that any of the parents would have the disease, so ignore that risk. Therefore, Charlene’s risk of being a carrier is 2/3 (sibling of affected in autosomal recessive disease, no affected parents). The risk that her partner is a carrier is also very small: therefore, the risk that the child is a carrier is = the risk that the child receives the bad allele from Charlene = 2/3*1/2 = 1/3.
In the following pedigree, you see a family with two people affected by a disease characteristic by immunodysregulation, polyendocrinopathy, and enteropathy. What is the best estimate of the risk that the unborn child III-2 will also have this disease?
A) 1/2
B) 2/3
C) 1/8
D) 1/3
E) 1/4

E.
Comment: This is a two step question where first step is to recognize inheritance pattern. The two affected children has no affected parents so this is recessive. The presence of two affected males who are nephew-uncle to each other makes this most likely X-linked recessive. Second step: under that assumption, then II-2 is a carrier for sure. Her risk of passing the bad allele on is ½, times ½ risk that the child is a boy = ¼ risk that the child is affected.
Given that the onset of the disease shown in the pedigree below is by 40 years of age and given that all of the individuals shown are at least 45 years old except III‑2 who is only 30 years old, what is the probability that the fetus (IV-1) will be affected?
A. 75%
B. 50%
C. 25%
D. 100%
E. virtually zero
C
Comment: This is a two step question where first step is to recognize inheritance pattern. The affected children in generation II and III all have affected parents so this is dominant. The presence of father to son inheritance (I-2 to II-1) makes this autosomal dominant. Second step: III-2 is too young to show symptoms, so her own phenotype does not tell us anything. Her mother (II-3) is a heterozygote (that is the rule for dominant diseases) so III-2 has a ½ risk of having received the bad allele. Her risk of passing the bad allele to her first child is another ½, so the total risk for IV-1 is ½*1/2 = ¼.
. A 4-year-old boy presents to the physician’s office with coarse facies, short stature, stiffening of the joints, and mental retardation. Both parents, a 10-year-old sister, and an 8-year-old brother all appear unaffected. The patient’s mother is pregnant. She had a brother who died at 15 years of age with similar findings that seemed to worsen with age. She also has a nephew (her sister’s son) who exhibits similar features. Based on the probable mode of inheritance, what is the risk that her fetus is affected?
A) 100%
B) 67%
C) 50%
D) 25%
E) virtually none
D
Comment: This is a two step question where first step is to recognize inheritance pattern. The several affected children have no affected parents so this is recessive. They are all males who are connected through females (the bad gene at no point would have passed through a healthy male) so this is most likely X-linked recessive. Second step: under that assumption, then the mother of our proband is a carrier for sure. Her risk of passing the bad allele on is ½, times ½ risk that the child is a boy = ¼ risk that the child is affected.
The pedigree below shows a family with a rare disease. Based on your assessment of the inheritance pattern, what is the risk that the child of III-13 (with an unrelated spouse) will have this disease?
A) ½
B) 0
C) 1/8
D) ¼
E) 1/3
D.
Comment: This is a two step question where first step is to recognize inheritance pattern. The affected children in generation II and III all have affected parents so this is dominant. The presence of father to son inheritance (II-11 to III-12) makes this autosomal dominant. Second step: The most frequent cause of getting this question wrong is to overlook the word “of” in the phrase “the child of III-13”. – II-11 is a heterozygote (that is the rule for dominant diseases) so III-13 has a ½ risk of having received the bad allele. The risk of passing the bad allele to the first child is another ½, so the total risk for IV-1 is ½*1/2 = ¼.
The following pedigree shows a family in which two members have Huntington disease. What is the most likely genotype at the Huntingtin gene of the three children (III-1 to III-3)?
A) Heterozygote, homozygote normal, heterozygote
B) Homozygote normal, heterozygote, homozygote affected
C) Heterozygote, heterozygote, homozygote normal
D) Homozygote normal, heterozygote, homozygote normal
E) Homozygote affected, heterozygote, homozygote normal

D
Comment: Huntington disease is autosomal dominant – either that is a fact that you know or you can conclude that from looking at I-1 and II-1. The fact that Huntington only shows symptoms later in life is one you need to know. On this basis, you should realize that the marker shared by I-1 and II-1 is on the same chromosome carrying the disease-causing allele. This allele is shared with III-2 who therefore is a heterozygote. The other two kids did not receive the bad allele and therefore are homozygous normal.
Albinism is an autosomal recessive trait. If we assume that 2% of the general population are carriers of the albinism gene, how likely is it that the child of an albino with a healthy unrelated partner is an albino?
A. 1 in 4
B. 1 in 200
C. 1 in 50
D. 1 in 100
E. 1 in 25
D
Comment: The albino is a homozygote and therefore for sure will pass on the bad allele to any offspring. The risk that the child becomes affected therefore is the same as the risk that the child receives a bad allele from the partner. That risk is ½ * the risk that the partner has the bad allele = ½*1/50 = 1/100. You should be aware that albinism is autosomal recessive, that could easily be deleted from the question.
. Now assume that the unaffected sister of an albino asks you how likely it is that her child with a healthy unrelated man will be an albino. Her parents are both unaffected. Assume a carrier frequency of 2% in the general population.
A. 1 in 800
B. 1 in 75
C. 1 in 300
D. 1 in 50
E. 1 in 150
C
Comment: The sister of an albino has 2/3 as her risk for being a carrier. The partner has a risk of 1/50. Each number needs to be multiplied with ½ and the results multiplied with each other = 2/3*1/2 * 1/50*1/2 = 1/300
. A healthy couple who have no children seeks genetic counseling because the husband’s two brothers died in their teens of the X-linked recessive Duchenne muscular dystrophy. Which of the following describes the husband’s risk of being a carrier of DMD?
A) 0
B) ¼
C) 1/3
D) 1/2
E) 3/4
A
Comment: With an X-linked recessive disease, a healthy male cannot be a carrier of the bad allele, risk = 0. (unless the male has undetected Klinefelter, for which the risk is less than 1/1000, and then he would likely be infertile)
A woman (I‑1) is deaf from an autosomal recessive disease. She marries a hearing man and has four children: two of the four children are deaf at an early age. Genomic DNA was isolated from peripheral blood lymphocytes from all family members and subjected to Southern blot analysis using a radiolabeled DNA probe known to be closely linked to the disease gene. Which of the following statements is TRUE about the offspring in generation II?
A. II‑1 will be a carrier and II‑3 will be normal
B. II‑1 will be normal and II‑3 will be a carrier
C. both II‑1 and II‑3 will be carriers
D. both II‑1 and II‑3 will be normal
E. II‑1 will be affected and II‑3 will be normal

C
Comment: The father (I-2) must be a heterozygote for the disease-causing allele. The affected daughter II-4 has received the lower of his two alleles, so that is the bad allele in him. The mother has two bad alleles. With this information, the rest should be straight forward.
A 4‑year‑old boy was brought to the emergency room by his mother after falling down three steps. The boy had skinned his knee and forearm on the cement and showed unusual and extensive bruising. To determine the genotype of the family members, genomic DNA was isolated from peripheral blood lymphocytes and subjected to Southern blot analysis using a radiolabeled DNA probe known to be closely linked to the X-linked disease gene. The boy is indicated by the arrow. Which of the following statements is TRUE about his siblings in generation III?
A. III‑1 will be a carrier and III‑2 will be normal
B. both III‑1 and III‑2 will be affected
C. both III‑1 and III‑2 will be normal
D. III‑1 will be affected and III‑2 will be a carrier
E. both III‑1 and III‑2 will be carriers
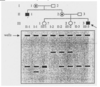
A
Comments: If you knew hemophilia well enough, the information about this being an X-linked disease would have been superfluous. Person III-3 has received his bad allele from his mother, so her lower allele is the bad allele in her. The allele at the same size in the father is a good allele, as is evident by his phenotype. (If you have difficulty with this, see your genetics professor). Once you have accepted this, the rest is straight forward
The figure below shows the pedigree of a family with Huntington disease. Which of the following statements best describes the linkage analysis for person III‑2?
A. This is an x‑linked recessive disease, the mutant allele was received from the mother (II‑2), and she will be a carrier
B. This is an x‑linked recessive disease, the mutant allele was received from the father (II‑1), and she will she a carrier
C. This is an autosomal dominant disease, the mutant allele was received from the mother (II‑2), and she will be affected
D. This is an autosomal dominant disease, the mutant allele was received from the father (II‑1), and she will be affected
E. This is an autosomal dominant disease, the mutant allele was not inherited from either the mother or father, and she will not be affected

E
Comment: the inheritance pattern clearly is dominant due to the affected children having affected parents. The marker allele shared among the affected people is the upper fragment, so one copy of this fragment is marking the bad allele. However, person II-1 is healthy and a homozygote for the same marker allele, so from him there is introduction of that marker allele going with the good allele at the gene. Person II-2 has the upper fragment from him (good allele) and the lower fragment from the mother (good allele) so is homozygote normal.
. A normal male mates with a female who is homozygous for an x‑linked recessive disorder. Of the offspring that they may have, it is probable that
A. no sons will be affected, and all daughters will be carriers
B. all sons will be affected, and all daughters will be affected
C. all sons will be affected, and all daughters will be carriers
D. no sons will be affected, and all daughters will be affected
E. all sons will be affected, and 1/2 the daughters will be carriers
C.
Comment: The homozygous mother must pass on one copy of the disease-causing allele to all offspring. The father does not have a disease-causing allele to pass on, it will either be good X or Y.
