What are some features of cutaneous immunity?
both the physical means to keep pathogens out and responses centered in the skin when pathogens get in
can be broken down into innate and adaptive responses
What are the layers of innate immunity in the skin?
encompasses those elements that are not specific to the pathogen and require no memory
- physical barrier
- epidermal production of protective proteins
- local cytokine production
- blood derived cells
What is the most superficial barrier of the skin?
stratum corneum
filaggrin - blocks microbes from penetrating the skin
atopic dermatitis when filaggrin breaks down
normal skin flora are competitive for spots to bind to skin
What is the second layer of barrier in the skin?
the microbe encounters constitutively expressed anti-microbial proteins in the stratum corneum
defensins are the most common
What is the third layer of barrier of the skin?
after the stratum corneum, the microbe separates tight junctions and activates toll-like receptors inducing and immune reaction
new AMPs are produced and blood borne immune cells are activated
What are the important factors of immune activation in the skin?
activation of TLRs to induce the production of cytokines like tumor necrosis factor-alpha (TNF) and interleukin-1 (IL-1)
blood borne cells including dendritic cells, neutrophils, mast cells, T cells can all be activated
dendritic cells, in particular, produce IL-23
What is the hypothesized pathophysiology of a psoriatic plaque?
TNF -> IL-23 -> IL-17 -> keratinocyte proliferation -> psoriasis
vicious cycle of keratinocyte release of proinflammatory cytokines and epidermal remodeling
chemotaxins are also involved in exacerbating the disease
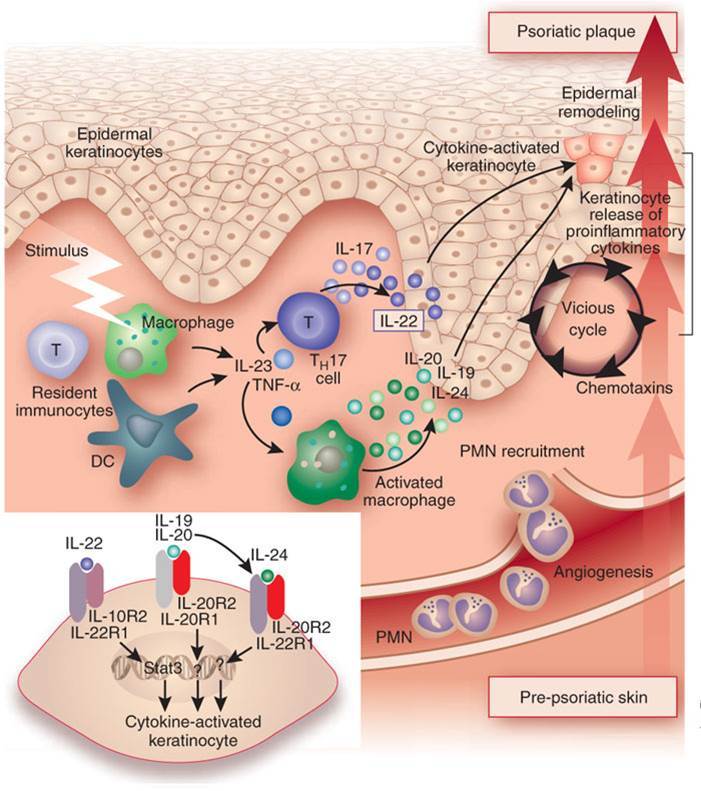
What is the effect of IL-23?
impacts many blood borne cells including T cells, neutrophils, and basophils
multiple cytokines are produced with the most interesting being the IL-20 family (IL-20,22, and 24) and, most importantly IL-17 of multiple types
What is the role of IL-17?
induces further changes in the epidermis, including thickening and induced AMP production
promotes increased recruitment of new cells
What is the epidemiology psoriasis?
most common inflammatory skin diseaes in adults - about 3% of the population
men = women
significant gentic predisposition, though about 50% of patients do not report a family history
Where are the most common areas for psoriasis?
elbos, knees, and scalp
these areas are most common place of trauma
What are the types of psoriasis?
limited plaque psoriasis
extensive plaque psoriasis
palmar-plantar psoriasis
scalp psoriasis
psoriatic nails
pustular psoriasis
erythrodermic psoriasis
What are histological findings of psoriatic skin?
thickened skin, scaly - live to dead keratinocyte is 7 days as opposied to 24 days
inflammation is present underneath
redness of the skin
What are some co-morbidities with psoriasis?
psoriatic arthritis
depression
diabetes mellitus
chron’s disease
psoriasis decreases work productivity
What are the risks of MI in patients with psoriasis?
increased risk in patients with severe psoriasis
risk is about 6.2% over 10 years, about quivalent to very high cholesterol
What are the common treatments for psoriasis?
topical therapies - corticosteroids, topical vitamin A and D derivatives
photoherapies - UV B, psoralen + UVA
synstemic therapies - methotrexxate, cyclosporine, retinoids
What is the clinical presentation of psoriasis?
scale - abnormal keratinocyte maturation, abnormal keratin expression (keratin 16)
thickness - rapid keratinocyte proliferation, increase in cell cycle markers (Ki-67)
redness - cutaneous vascular proliferation and dilation
What is the role of STAT-3 in psoriasis?
links activated keratinocytes and immunocytes required for development of psoriasis in a novel transgenic mouse model
Ustekinumab
useful drug for psoriasis
human monoclonal antibody that blocks IL-12 and IL-23
Brodalumab
monoclonal antibody that blocks IL17RA
inhibits IL17 A, C, and F
Ixekizumab and Secukinumab
monoclonal antibodies that inactivate only IL17A
treatment for psoriasis
What is IL-12, and what is its role in psoriasis?
heterodimer composed of p35 and p40 subunits
produced by activated dendritic cells and macrophages
promotes growth and differentiation of naivev T cells into Th1 cells and cytotoxic T cells
down regulates Th2 cytokines such as IL-10
What is the role of the p40 subunit in psoriasis?
subunit of IL-12 and IL-23
upregualted in lesional skin of psoriatic patients
initially interpreted as increased IL-12
later analysis showed not increase of p35 subunit in psoriatic plaques
IL-23, rather than IL-12, mediates psoriasis
What is the role of IL-23 in psoriasis?
can activate local inflammatory cells to produce:
- IL-17 family cytokines
- IL-20 family cytokines
-
Cartilage Histology33
-
Bone Histology and Development50
-
Bone Physiology - Endocrine34
-
Orthopedic Pathology56
-
Functional Anatomy of the Spine37
-
Structure and Function of the MSK System48
-
Organization and Development of the Limbs38
-
Osteoarthritis48
-
Muscle Mechanics and Physiology23
-
Inherited Disorders of Connective Tissue43
-
Functional Anatomy of the Forearm and Hand63
-
Musculoskeletal Imaging48
-
Musculoskeletal Trauma23
-
Pediatric Musculoskeletal Injuries36
-
Blood Supply of the Upper Extremity45
-
Blood Supply of the Lower Extremity57
-
Adult Sports Medicine and Overuse Injuries53
-
Sports Injuries Unique to Young Athletes51
-
Immunosuppressive Therapies for Auto-immune MSK Diseases16
-
Neuropathies of the Upper Limb43
-
Seronegative Spondyloarthropathies (SpA)51
-
Neoplasms of Bone and Joint Pathology62
-
Scleroderma (Systemic Sclerosis)26
-
Bone and Joint Infections38
-
Pediatric Rheumatology51
-
Crystalline Arthropathies28
-
Inflammatory Myopathies22
-
Systemic Lupus Erythematosus42
-
Functional Anatomy of the Lower Limbs22
-
Vasculitis37
-
Acute and Chronic Pain49
-
Glucocorticoids22
-
Rheumatoid Arthritis51
-
Biologic Response Modifiers in Rheumatologic Disease18
-
Opioids47
-
NSAIDs33
-
Integrative Medicine10
-
Hip and Knee Replacements27
-
Back Pain17
-
Skin Structure and Function45
-
Melanocytes, Nevi, and Melanoma33
-
Cutaneous Manifestations of Systemic Disease77
-
Eczema and Itchy Skin22
-
Psoriasis24
-
Dermatologic Manifestations of Bacterial Infections32
-
Cutaneous Manifestations of Viral Infections47
-
Benign Skin Neoplasms24
-
Wound Healing36
-
Nonmelanoma Skin Cancer40
-
Drug Reactions and Blistering Disorders55
-
Peds Derm Topics24
-
KOH and bugs10
-
ID Derm Part 237
-
Connective Tissue Disease26
